

Who Me?
Well-Known Member
Serum BAFF and APRIL Levels, T-Lymphocyte Subsets, and Immunoglobulins after B-Cell Depletion Using the Monoclonal Anti-CD20 Antibody Rituximab in Myalgic Encephalopathy/Chronic Fatigue Syndrome

http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0161226
- Sigrid Lunde,
- Einar K. Kristoffersen,
- Dipak Sapkota,
- Kristin Risa,
- Olav Dahl,
- Ove Bruland,
- Olav Mella,
- Øystein Fluge
- Published: August 18, 2016
- http://dx.doi.org/10.1371/journal.pone.0161226
cont.Abstract
mce-anchor
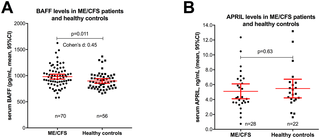
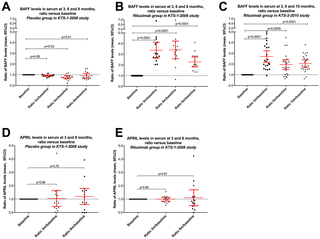
Myalgic Encephalopathy/Chronic Fatigue Syndrome (ME/CFS) is a disease of unknown etiology. We have previously suggested clinical benefit from B-cell depletion using the monoclonal anti-CD20 antibody rituximab in a randomized and placebo-controlled study. Prolonged responses were then demonstrated in an open-label phase-II study with maintenance rituximab treatment. Using blood samples from patients in the previous two clinical trials, we investigated quantitative changes in T-lymphocyte subsets, in immunoglobulins, and in serum levels of two B-cell regulating cytokines during follow-up. B-lymphocyte activating factor of the tumor necrosis family (BAFF) in baseline serum samples was elevated in 70 ME/CFS patients as compared to 56 healthy controls (p = 0.011). There were no significant differences in baseline serum BAFF levels between patients with mild, moderate, or severe ME/CFS, or between responders and non-responders to rituximab. A proliferation-inducing ligand (APRIL) serum levels were not significantly different in ME/CFS patients compared to healthy controls at baseline, and no changes in serum levels were seen during follow-up. Immunophenotyping of peripheral blood T-lymphocyte subsets and T-cell activation markers at multiple time points during follow-up showed no significant differences over time, between rituximab and placebo groups, or between responders and non-responders to rituximab. Baseline serum IgG levels were significantly lower in patients with subsequent response after rituximab therapy compared to non-responders (p = 0.03). In the maintenance study, slight but significant reductions in mean serum immunoglobulin levels were observed at 24 months compared to baseline; IgG 10.6–9.5 g/L, IgA 1.8–1.5 g/L, and IgM 0.97–0.70 g/L. Although no functional assays were performed, the lack of significant associations of T- and NK-cell subset numbers with B-cell depletion, as well as the lack of associations to clinical responses, suggest that B-cell regulatory effects on T-cell or NK-cell subsets are not the main mechanisms for the observed improvements in ME/CFS symptoms observed in the two previous trials. The modest increase in serum BAFF levels at baseline may indicate an activated B-lymphocyte system in a subgroup of ME/CFS patients.
Figures


.
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0161226



![ME/CFS lecture | Dr Nancy Klimas | 2011 [Chronic Fatigue Syndrome / SEID / New Zealand] - YouTube](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)







