


Geoff’s Narration
The GIST
Fluvoxamine’s “success” didn’t exactly send long-COVID patients jumping for joy. While its success was modest, it was, however, a large study that moved the needle – something only one other clinical trial was able to do.
Because it was a large study, we need to pay attention to its results. Among other things, the results suggested that sphingomyelinase drugs, called FIASMAs, which reduce sphingomyelin levels, particularly sphingomyelin-derived ceramides, might be helpful.

Is something different happening in ME/CFS and long COVID?
High ceramide levels have been associated with a number of neurological disorders (including multiple sclerosis) and could help produce the endothelial and microvascular damage, neuroinflammation, and metabolic stress that lock these diseases into place. They’re found in a number of neurological conditions including multiple sclerosis, Parkinson’s disease, depression, as well as cancer.

These drugs may inhibit the formation of the “platforms” that viruses use to enter cells.
Note that we don’t know if ceramide levels are increased in long COVID – it’s just a possible supposition. If they are, FMASMA drugs might help, but the latest studies suggest not in ME/CFS.
The ME/CFS Switch?
FIASMA drugs make sense if sphingolipids and ceramides are high in long COVID. They do not make sense if, as some studies suggest, sphingolipids and ceramides in the membrane are low in ME/CFS. In fact, they could reduce energy levels and worsen things.
Recently, in “SMPDL3B, a novel biomarker and therapeutic target in myalgic encephalomyelitis“, the Open Medicine Foundation’s Research Center at the CHU Sainte-Justine Université de Montréal, took a deep dive into a sphingolipid regulator called SMPDL3B.
We’ve heard very little about SMPDL3B, but Moreau first presented on it at a 2020 conference. The key thing is that SMPDL3B is a “regulator”. It’s a sphingolipid-altering enzyme that sits at an inflection point and affects both cellular lipid membranes and the innate immune system. In fact, this regulator could conceivably both enhance innate immune system-driven inflammation and inhibit antiviral activity.

Voila! The Open Medicine Foundation presents a “novel immunomodulatory approach” to ME/CFS
THE GIST
- The modest success of fluoxamine in a large COVID trial suggested that sphingomyelinase drugs, called FIASMAs, might be helpful.
- A recent study, “SMPDL3B, a novel biomarker and therapeutic target in myalgic encephalomyelitis“, from the Open Medicine Foundation’s Research Center at the CHU Sainte-Justine Université de Montréal, suggested that something different may be happening in ME/CFS.
- SMPDL3B is a sphingolipid-altering enzyme and regulator that sits at an inflection point and affects both cellular lipid membranes and the innate immune system. This regulator is particularly interesting because it could conceivably both enhance inflammation driven by the innate immune system and inhibit antiviral activity.
- High SMPDL3B levels in ME/CFS patients’ plasma paired with low cell membrane levels suggested that it was being cleaved off the cell membranes and dumped into the plasma. High levels of the cleaving agent, PLCXDI, in ME/CFS patients indicated this was so.
- Ultimately, this meant ME/CFS patients’ cell membranes were low in important structural elements called sphingolipids – including the ceramides. Reduced ceramide levels, in turn, could produce a situation we’ve seen before and will see again (in the next blog): it may leave cells inert and unresponsive to external signals, impair their mitochondrial functioning, and prevent them from responding to stress.
- One wonders if the low ceramide levels could help explain why so many systems fail to kick in during the post-exercise period.
- A more recent paper, “Circulating Levels of SMPDL3B Define Metabolic Endophenotypes and Subclinical Kidney Alterations in Myalgic Encephalomyelitis“, from the Moreau group in Canada, took the SMPDL3B finding in a rather surprising but potentially promising direction – the kidneys.
- How to explain the increased sphingolipids/ceramide levels found in COVID-19 and the decreased levels Naviaux found ME/CFS? Perhaps, the same way Hornig and Lipkin accounted for the intense immune activation found in shorter-duration ME/CFS patients, and the immune downregulation found in patients with longer-duration ME/CFS: exhaustion.
- Kidney cells called podocytes were assessed because they contain high levels of sphingolipids in them. These cells, which filter the blood, are under high structural stress and need the sphingolipids to work perfectly.
- Similar results (high plasma SMPDL3 levels) were found, and a plasma metabolomics analysis suggested that a broad dysregulation of metabolites associated with impaired kidney function had occurred. (Note that this kind of dysregulation would not show up in standard kidney tests.)
- Now to a question not raised in this paper: could these kidney findings bear on one of the most mysterious aspects of ME/CFS (and POTS): the renin-aldosterone paradox?
- The renin-aldosterone paradox describes a situation in which ME/CFS patients’ blood volume is low, but so are the factors (renin/aldosterone) that are supposed to kick in to resolve it. Instead of increasing, they’re actually lower than normal (!).
- Nobody knows why this is happening, but the SMPDLB3 issue could help explain it. Low SMPDLB3 levels in podocytes could prevent them from performing their filtration function properly. That could allow the kidneys to believe more salt is present in the blood than actually is and cause them to shut down the renin-aldosterone system, which increases blood volume by increasing salt levels.
- The idea that low SMPDL3B levels in cellular membranes in ME/CFS could be contributing to hypovolemia, impaired response to exertion, and metabolic and mitochondrial problems is indeed enticing. These are, however, all untested hypotheses, and other factors could account for them.
- SMPDL3B’s regulatory function, though, is beyond intriguing. ME/CFS and long COVID, with their disrupted immune networks and dysregulated stress responses, appear to be diseases of regulation; that is, diseases in which central regulators, perhaps like SMPDL3B, have gone awry.
- That might be a good thing if fixing these diseases simply requires fixing central regulators.
- The Moreau team restored SMPDL3B membrane levels in the lab using two diabetes drugs called saxagliptin and vildagliptin (marketed in Europe). The authors proposed that these drugs may provide a “novel immunomodulatory strategy” for ME/CFS.
- The OMF will use its new decentralized, virtual, and remote CTN-Lite clinical trial program, as well as its MEDUSA program, to assess the safety and efficacy of low-dose saxagliptin plus myo-inositol in ME/CFS. Not only will it assess their effects on symptoms, but on the biological pathways involved as well.
- Time will tell how this all will work out, but what an interesting saga this is! Suddenly, we have a new, plausible cause or contributor to ME/CFS that could explain much (including a paradox), and a brand-new treatment approach.
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit
The ME/CFS Sphingolipid Saga
Indications that something has gone wrong with the sphingolipids – key structural elements in cellular membranes – first showed up in Naviaux’s 2016 paper “Metabolic features of chronic fatigue syndrome“. Naviaux’s study found dramatic reductions in sphingolipids (and other lipids) in ME/CFS. Naviaux proposed that a hypometabolic state existed in ME/CFS.
Several studies suggest that sphingolipids – including ceramides – may be affected in ME/CFS.
From there, things get a little muddier. Two years later, Lipkin and Nazy-Gul’s metabolomic study found evidence of decreased sphingolipid metabolism in ME/CFS patients without IBS, and some evidence of increased plasma ceramide levels in ME/CFS patients with IBS. Their meta-map concluded that increased triglycerides and fatty acids and decreased carnitines, ceramides, sphingomyelins, and phosphatidylcholines characterized ME/CFS.
Then came the 2020 Hanson/Germain plasma metabolomics study, which found increased sphingolipids (oops!). Hanson/Germain proposed that sphingolipid abnormalities were probably more the result of dietary changes and physical activity than anything central to ME/CFS.
The large 2020 Che/Lipkin plasma metabolomics study (n=197), though, put the sphingomyelins/ceramide issue front and center again by finding significantly decreased ceramides, sphingomyelins, lysophosphatidylcholines, phospholipid ethers, and prostaglandins. An enrichment analysis also found reduced levels of sphingomyelins and unsaturated ceramides.
This study was important because it potentially linked sphingolipid abnormalities to peroxisomes, plasmalogens, mitochondrial function, and GCPR receptors (GPCRs), which could be affecting autonomic and immune function in ME/CFS.
Lastly, an Australian researcher, Junhua Xiao, recently proposed that sphingolipid metabolism was “the dominant metabolic pathway” in ME/CFS, and suggested restoring sphingolipid levels by modulating an enzyme called sphingosine 1-phosphate lyase in ME/CFS.
That brings us to the recent Afshari-Moreau paper, which potentially links sphingomyelins/ceramides to immune and cell membrane problems in ME/CFS.
SMPLD3 – A Key Player in ME/CFS?

Could reduced ceramide levels also be contributing to the PEM found in ME/CFS?
Moreau, Rofstami-Afshar, and company found significantly elevated plasma levels of a sphingolipid regulator called SMPDL3B in two large ME/CFS cohorts (n=350+).
These elevated plasma SMPDL3B levels correlated with symptom severity, were higher in ME/CFS females, were influenced by estrogen, and modulated by TLR4 signaling (see low-dose naltrexone); i.e., they look like a real winner in ME/CFS.
It’s not as simple as that, though. Low SMPDL30 cell membrane levels and increased levels of a cleaving agent, PLCXDI, suggested that SMPDL30 was being cleaved from cell membranes and then released into the plasma. The real problem was not high plasma SMPDL3B levels but low SMPDL30 levels in cellular membranes.
Because SMPDL30 converts sphingomyelins into ceramides in cellular membranes, reduced SMPDL30 levels there could result in reduced plasma ceramide levels, as Naviaux found earlier.
Inert and Unresponsive…Again?
By removing a core structural element of lipid membranes, reduced ceramide levels could render cells inert and unresponsive to external signals, impair mitochondrial function, disrupt insulin signaling, and prevent cells from responding to stress. (Shades of Naviaux’s Dauer response?)
Because ceramides play a key role in helping the body adapt to stress, it seems conceivable that low membrane ceramide levels could even help explain the mysterious inability of many systems in the bodies of ME/CFS patients to respond to exertion.
Without sufficient ceramide membrane levels, cells may not be able to respond on many levels – from mechanical stress to mitochondrial stress to protein production and muscle repair – to the stress caused by exertion.
Impaired cellular signaling has always seemed like a kind of amorphous explanation for ME/CFS, but it could affect almost everything.
When It Comes to ME/CFS and Long COVID, Duration May Matter
But how to explain the increased sphingolipids/ceramide levels found in COVID-19 and the decreased levels Naviaux found ME/CFS? Perhaps, the same way Hornig and Lipkin accounted for the intense immune activation found in shorter-duration ME/CFS patients, and the immune downregulation found in patients with longer-duration ME/CFS patients: exhaustion over time.
Perhaps chronic activation/injury to the cellular membranes over time results in a similar exhaustion there. Perhaps the cells shut down ceramide production, aka Naviaux’s Dauer hypothesis, in order to avoid the toxic hits they’re getting. (A similar duration-produced scenario is going to show up in the next blog.)
If you tried a FIASMA drug and had a negative experience, one conclusion might be that the drug depleted your cellular membranes of sphingolipids and ceramides they needed. (???)
On the other hand, if that’s not the case and a stressor like exercise or a cytokine spike causes your ceramides (stress-response chemicals) to spike, then FIASMA drugs might help. Or, if endoplasmic reticulum stress is a problem – and some studies suggest it may be – FIASMA drugs could conceivably help as well.
The Moreau team’s recent study (see below) suggests ME/CFS patients lean toward the first scenario, but we don’t know, and subsets surely exist. We need much more data on sphingolipids, ceramides, peroxisomal function, and related areas to know for sure. We are a heterogeneous group, and either low or high ceramide levels could be causing problems.
The Kidneys?
We’re not done yet, though. A more recent paper, “Circulating Levels of SMPDL3B Define Metabolic Endophenotypes and Subclinical Kidney Alterations in Myalgic Encephalomyelitis“, from the Moreau group in Canada, took the SMPDL3B finding in a rather surprising but potentially promising direction – the kidneys.

The kidneys have rarely been discussed in ME/CFS, but kidney cell (podocyte) issues might not show up in routine kidney tests. (Image from CDC via Wikimedia Commons)
This study focused on kidney functioning – a rarely discussed topic in ME/CFS. The researchers clearly wanted to see if they could extend the SMPLD38 finding from immune cells to other cells, and they picked kidney cells called podocytes because SMPDL3B is most highly expressed in them. (It’s more moderately expressed in immune cells.)
Because podocytes are responsible for the kidneys’ filtering properties, they’re under a lot of stress, which means the sphingolipids that make up the structural elements of their membranes need to function perfectly.
The second study backed up the first study’s findings. Lower urine-to-plasma ratios of soluble SMPDL3B suggested that SMPDL3B was being dumped into the plasma at high levels. The reduced renal clearance (lower urine levels) suggested that the kidney cells (podocytes) were not filtering it from the blood as effectively.
Plus, a plasma metabolomics analysis suggested that a broad dysregulation of metabolites (succinic acid, benzoic acid, phenyllactic acid, 1,5-anhydroglucitol, histidine, and citrate) associated with impaired kidney functioning was present. Several of these could also help explain the reduced mitochondrial functioning often found.
In another sign they were on the right track, females exhibited greater reductions in renal clearance and urinary-to-plasma SMPDL3B ratios. While these abnormalities would not show up in a kidney screen, they suggest the kidneys may be playing a role in ME/CFS.
Three SLMP3B ME/CFS groups were found: high, intermediate, and low. The high group appeared to have the greatest kidney involvement, but interestingly, the data suggested that both the high and low SLMP3B groups were found – both of which may have problems with kidney cell (podocyte) and mitochondrial function.
Paradox Solved?
Now to a question not raised in this paper: could these kidney findings bear on one of the most mysterious aspects of ME/CFS (and POTS): the renin-aldosterone paradox?
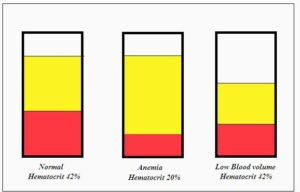
Despite the low blood volume problems found in ME/CFS, both the factors designed to increase blood volume are lowered in ME/CFS.
During periods of low blood volume, the body increases renin and aldosterone levels to retain more sodium and increase blood volume. Despite the low blood volume found in these diseases, that’s not happening. Both renin and aldosterone levels in ME/CFS and POTS are actually lower than normal, and that’s the paradox.
The results from the Moreau paper pointed to problems with the kidney’s “tubular functioning”. After the glomerulus in the kidney filters the blood, the tubules process what’s left over; i.e., they decide what the body should retain and what it should get rid of. Importantly, for us, the tubules also regulate sodium levels via the macula densa.
If low SMPDL3B podocyte levels impair the ability of the cells in the glomerulus to filter the blood properly, abnormally high or low sodium levels could land in the tubules, and produce a false high sodium reading that causes the macula densa to reduce renin/aldosterone production even in the presence of low blood volume, which is what we see in ME/CFS.
The RAAS paradox in ME/CFS – and the low blood volume that accompanies it – could, then, conceivably be traced back to low cellular membrane SMPDL3B levels in the kidney cells.
The ACE2 receptor provides another possible point of intersection. It did not escape notice that the same receptor the coronavirus uses to enter cells – the ACE2 receptor – also appears to be impaired in ME/CFS and POTS. (Activation of the ACE2 receptor starts off the renin-angiotensin-aldosterone system.) It turns out that reduced membrane SMPDL3B levels could also affect ACE2 function.
Regulatory Diseases?
Could ME/CFS, in part, be a disease of impaired regulation?
The idea that low SMPDL3B levels in cellular membranes in ME/CFS could be contributing to hypovolemia, impaired response to exertion, and metabolic and mitochondrial problems is indeed enticing. These are all untested hypotheses, and each of these issues could be explained by other factors. Time will tell.
SMPDL3B’s regulatory function, though, is beyond intriguing. ME/CFS and long COVID, with their disturbed immune networks and dysregulated responses to stress, look like they could be diseases of regulation; that is, diseases in which central regulators, perhaps like SMPDL3B, have gone awry. The nice thing about these regulators is that fixing them could potentially solve many problems.
We need to learn a lot more about SMPDL3B. Where does it fit, for instance, in the river of dysregulation that produces these diseases? Is it a causal agent that lives upstream? Or does it simply reflect a core cause that lives upstream?
For now, though, the SMPDL3B findings are clearly presenting an exciting opportunity for further research and treatment.
A Novel Immunomodulatory Strategy for ME/CFS?
By inhibiting the SMPDL30 cleaving agent PLCXDI with two diabetes drugs, vildagliptin (marketed in Europe) and saxagliptin (approved in the U.S.), Moreau et al. was able to restore SMPDL3B membrane levels in the lab. The authors proposed that these drugs may provide a “novel immunomodulatory strategy” for ME/CFS, and the Open Medicine Foundation looks like it’s ready to test it.
The Open Medicine Foundation’s (OMF’s) CTN-Lite Premiers

The OMF’s CTN-Lite clinical trial program just appeared. The program reminds me of how blessed the ME/CFS field is to have so many forward-thinking organizations. How we garnered so much support over time, I don’t know. (I do think the early emergence and staying power of the IACFS/ME and Solve M.E. in the US helped.)
I searched for private fibromyalgia research funders and found one. Compare that to ME/CFS: the OMF (US, Canada, Sweden, Australia), Solve M.E. (US), (PolyBio – long COVID and ME/CFS, US), Simmaron Research Foundation (US), Invest in ME (UK), MERUK (UK), Action For ME (UK), ME/CFS Research Foundation (Germany). Plus, private research efforts like Amatica and PrecisionLife are engaged in bold research projects. Cynthia Addington reports that the AI engines, predictive algorithms, and structural tools propelling one of the newest efforts on the block – Cynaera – “are transforming what we know about ME/CFS” and similar diseases.
Ten times as many people have fibromyalgia, but for some reason, when it comes to creativity, participation, and innovation, the ME/CFS field is the clear winner. How this small field has fostered so much creativity, I don’t know, but we’re clearly in a potentially fruitful time.
Now here comes the Open Medicine Foundation’s “Clinical Trials Network Lite” (CTN-lite) – a robust, decentralized clinical trials network that will include multiple research sites offering both virtual and remote participation opportunities, thus allowing sicker patients to participate, and improving trial efficiency.
These trials will also be “smarter”. Instead of simply assessing symptoms, the OMF will determine how the treatments they test are influencing biological pathways. In fact, they’ll prioritize treatments that allow them to do that.
With this two-fer approach, they’ll learn about treatment efficacy as they’re learning about the disease’s biological underpinnings. PolyBio is taking the same approach with its clinical trials. No clinical trials are being conducted that aren’t exploring the biological effects of these drugs. These trials are miles ahead of past trials.
The OMF would like to know what your priorities for this new approach are – click here to take a survey.
Saxagliptin and Vildagliptin
While these drugs are used to lower glucose levels in diabetes, they would, as explained above, inhibit the PLCXDI enzyme from knocking SMPDL30 off the cellular membrane. These drugs usually produce mild side effects, but at times, they can produce some nasty problems. Vildagliptin is not available in the US, and saxagliptin will be used in low doses.
A novel immunodulatory treatment strategy is proposed.
Since this paper was published, the Open Medicine Foundation reported that “additional unpublished work suggests that combining low-dose saxagliptin with myo-inositol may allow clinically realistic dosing.”
In a published response to a question, the authors explained why they took this route. The amount of saxagliptin needed in the laboratory to inhibit the PLCXDI enzyme was too high for the drug to be used in human trials.
To reduce the dose, they combined saxagliptin with the myo-inositol supplement. They found that adding 4,000 µM myo-inositol allowed them to use only 0.5 µM saxagliptin – a safe dose.
Saxagliptin appears to be the first drug used in the Open Medicine Foundation MEDUSA (ME/CFS Adaptive Therapeutic Solution) platform developed by Alain Moreau in Montreal. MEDUSA uses deep phenotyping and multi-omics testing to identify biologically-based subgroups and match them to repurposed drugs.
What an interesting saga this is! Suddenly, we have a new, plausible cause or contributor to ME/CFS and a brand-new treatment approach.
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit



Interesting, thanks Cort.
Moreau is one of the more interesting and hope-giving researchers in the ME/CFS field. He’s doing some great stuff
Yes, that accent makes it hard to understand what he’s saying, but he’s clearly very innovative and creative. Glad we have him!
That accent is beautiful. Vive le professeur Moreau!
I just read both studies, fascinating.
In a research field that often feels stale and not going anywhere fast, it’s great to see such creative and compelling research. Would be interesting to know next steps in terms of whether there are therapeutic studies / trials planned.
I love creative research, but I would love even more than that effective treatments 😎 hopefully one will lead to the other
Menu
Wake Forest University School of MedicineSearch
Human Urine-derived Stem Cells Have Robust Regenerative Potential
July 26, 2022
Wake Forest Institute for Regenerative Medicine (WFIRM) researchers who were the first to identify that stem cells in human urine have potential for tissue regenerative effects, continue their investigation into the power of these cells. In their latest published study, they focus on how telomerase activity affects the regenerative potential of these and other types of stem cells.
Telomerase is an enzyme that is essential for the self-renewal and potential of different types of stem cells. Telomerase activity is also closely related to longevity. The research team investigated the regenerative significance of telomerase activity, particularly in terms of characteristic cell surface marker expression, multipotent differentiation capability, chromosomal stability, and safety of in vivo formation of tumors.
Their findings provide a novel perspective to evaluate the capacity of telomerase-positive human urine-derived stem cells to become a wide variety of other cell types, and to be used as an optimal cell source for stem cell therapy or cell-based tissue regeneration.
WFIRM’s Yuanyuan Zhang, Ph.D, lead author of the paper published by Frontiers in Cell and Developmental Biology, said that human urine-derived stem cells can be easily isolated from urine samples which offers clear advantages over stem cells from other sources, like bone marrow or fat tissue which often require a surgical procedure for collection.
“Being able to use a patient’s own stem cells for therapy is considered advantageous because they do not induce immune responses or rejection,” said WFIRM Director Anthony Atala, MD, who is a co-author of the paper. “Additionally, the non-invasive collection method is suitable for rapid clinical translation.”
The study demonstrates that human primary urinary stem cells with positive telomerase activity act as a distinct subpopulation with potential regeneration capacity in both cell growth and its capacity to become other cells, Zhang said. Better understanding of alterations in this cell subpopulation throughout the human lifespan, and how they translate into, aging, kidney damage, or cancer, among others will be beneficial overall.
“As a safe cell source, telomerase-positive human urine-derived stem cells have a robust regenerative potential, which might induce better tissue repair,” said Zhang.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This work is partially supported by Research Grants from the National Institutes of Health NIDDK (R21DK071791), (R56DK100669), NIAID (R21AI152832), and (R03AI165170)
How does Fluvoxamine relates with this?
Fluvoxamine relates to this because it appeared to help (modestly) in long COVID. Fluvoxamine is an FIASMA drug that REDUCES ceramides.
This study, on the other hand, suggested that, instead of being too high, the ceramides in ME/CFS patients are getting cleaved off their cellular membranes, and are ending up in their plasma; i.e. they are too low in ME/CFS.
At this point this is all conjecture, though. We don’t actually know what the ceramide levels in long COVID are. We know that ceramide levels rise in COVID-19 – which makes sense – as they rise during times of stress, and it’s possible that they are still high in long COVID but we don’t actually know.
Plus it wouldn’t be surprising at all – as this study showed – to have subsets with high ceramide and subsets with low ceramide levels.
Thanks Cort. I’m having trouble following along without the written form of “the gist.” Have you stopped posting this? I can’t process (understand) the recording. Maybe because of the long scientific words, maybe because of the monotone. Not criticizing, but do some people need it to be monotone in order to process it? Thanks for all you do!
Hi Barbara, The Gist is tucked into the Read More box this time, I was very glad to find it there as I am in the same boat as you re understanding/processing anything very complex via the spoken word. (Or even anything not very complex!)
Thanks Alison!
The written form of The Gist is there – right under the paragraph headed “The ME/CFS Switch?”
Thank you Fay! I had to click on the graphic and there it was.
Cort, did the researchers give any reason why they’re choosing saxagliptin over sitagliptin (Januvia) for their study, given the cardiovascular risks of saxagliptin? I realize they’re going low dose for the study, but sitagliptin definitely has a lower risk profile, especially for heart failure.
I find it curious that some of us with the RAAS Paradox benefit from ARBs like losartan (I do), which I take to normalize my elevated TGF-Beta1 levels. After I began taking losartan, my renin levels actually tripled from below normal to mildly normal (aldosterone is still in the single digits). There has to be a connection if someone like me with ME/CFS who had five times the upper normal level of TGF-Beta1 can drop that level to the mid-normal range with the lowest tablet dose of 25mg losartan each day without making much of a dent on my blood pressure.
The researchers are definitely onto something here, regarding kidney involvement. Those of us with the RAAS Paradox have suspected kidney involvement forever.
I have thought the same thing about RAAS paradox for the last 8 years. How the heck can we get nephrologist to even conceive of this at upcoming appt? We are already planning to introduce the recent Swedish study on fluid homeostasis in Long Covid patients.
https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2026.1741517/full
Why resort to drug therapy?
Both high dosage NAC and MSM can help kidney function
“Dr Markov’s chronic bacterial intoxication syndrome (CBIS) theory of ME/CFS – MEpedia” https://me-pedia.org/wiki/Dr_Markov%27s_chronic_bacterial_intoxication_syndrome_(CBIS)_theory_of_ME/CFS
On CFS and kidneys
I was in touch with Dr. Markov’s office and considered his treatment protocol, but decided that there might be significant problems getting the samples and vaccines back and forth since he is in the Ukraine. I am surprised no one in the states has tried this protocol since nothing else seems to work.
The reason I was interested in Dr. Markov’s protocol is a family experience. Many years ago, my grandmother, grandfather and their 3 sons went to Colorado because the doctors thought the climate would help my grandfather’s tuberculosis. My grandmother was exhausted taking care of everyone and had recurrent urinary tract infections. Finally, one doctor suggested making a vaccine from the bacteria in her urine. This cured her. I think they did a lot of this before the advent of antibiotics. They even do it now in veterinarian practice. “Veterinarians use vaccines created from bacteria or viruses isolated directly from an animal or its herd to treat that specific animal or group, especially when commercial vaccines are ineffective or unavailable.”
If you would like to know more about autogenous vaccines, you can read about their history on this Wikipedia page. They are used in Eastern Europe, but I am not sure where except the Markov Clinic.
https://en.wikipedia.org/wiki/Autogenous_vaccine#:~:text=autogenous%20vaccines.%20%5B1%5D,for%20example%20chronic%20staphylococcal%20infections.
E
Wow, that’s so interesting!!!
Is this well known in the scientific research community?
Although autogenous vaccines are currently used in vet medicine, the only place I have heard of its use in humans is the Markov clinic and I am not sure they are in operation now because of the war. This is not the kind of treatment that pharmaceutical companies would pursue for obvious reasons. There may be other clinics in Europe, but I am not sure how to find them.
I have been in glucosamine with no effect what so ever. The only drugs that have really helped are DHEA low dose naltrexone? Endepp for pain and sleep. Currently looking for another autoimmune drug as LDN now failing. It got me 80 per cent well!
Can low dose saxagliptin be used off label now Australia ?
Low dose Naltrexone after three good years now failing.
So interesting. I have elevated ACE level. Also low blood volume. Desmopresin helps a little. I wonder if this is somehow connected. My renin is not high of course.
How can I test for toxins?
Hi Cort,
If you want to know more about everything Dr. Moreau is doing in Montreal, see link below.
https://www.omfcanada.ngo/collaborative-research-center-montreal/
Very exciting to learn of this!
Regarding the kidney involvement, could that explain a couple of instances of blood in the urine?
The vgliptan id available in nz , is that worth trying and at what dose