


The Folic Acid Story
Did the FDA’s attempt to reduce birth defects have unintended consequences?
In the 1990’s, the US and UK mandated the enrichment of all grain products with folic acid in hopes of reducing the occurrence of neural tube defects. In the decades since neural tube defects have indeed declined yet little long term research has been done to determine the effects excess folate might have on non-pregnant adults.
The tolerable upper limit (TUL) for folate is set at 1,000 mcg/day for adults, but with the overconsumption of fortified grain products many may exceed this threshold. Recent studies are now taking a closer look at potential health risks of folic acid fortification for adults.
Folate is not only a concern for adults, but may have particular relevance for some people with Chronic Fatigue Syndrome (ME/CFS).
What Role Might Folate play in ME/CFS?
Folate is a vital component of the single carbon pool that participates in basic cellular processes such as amino acid metabolism, synthesis of nucleotides (DNA, RNA, ATP), and methylation (including epigenetic methylation of DNA). Low levels of folate are implicated in increased risk of cardiovascular disease, stroke, dementia, depression, cancers, and birth defects. Similarly, high levels are also associated with carcinogenesis (1).

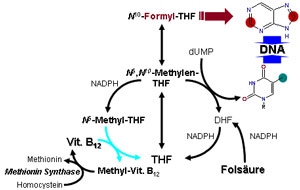
Folate metabolism is a complex, multi-step process that occurs in every cell in the body. It requires three key enzymes: dihydrofolate reductase (DHF), methylenetetrahydrofolate reductase (MTHFR), and methionine synthase (MTR). When you consume the synthetic form of folate – folic acid – in enriched foods or supplements, it must be converted to different forms utilizing these enzymes. If this conversion is inadequate, functional folic acid deficiencies can emerge that may dampen methylation, amino acid metabolism, etc.
Despite the fact that this biochemistry has been known for decades, few studies have examined the exact mechanisms by which folic acid is taken up or metabolized in the body after consumption. Those studies which have examined folic acid metabolism have relied only on mouse models which have substantially different concentrations of the above enzymes than humans (2).
Gut-Check Time for Folic Acid Supplementation
A recent study in patients with stable liver disease indicated, however, that synthetic folic acid from traditional supplements was inefficiently absorbed in the intestinal tract compared to the active 5-methyl-hydrofolate (5-MTHF) form (which was taken up twice as readily). The researchers concluded that food regulatory bodies should rethink their position on folic acid enrichment. Interestingly, the FDA and European Food Standard Agency have already approved products containing 5-MTHF derivatives to replace folic acid (3).
A Key Metabolic Factor – More Biochemistry
B-12, an essential co-factor in folic acid metabolism, is often low in ME/CFS
The folate cycle feeds into other key biochemical cycles as well. The end product of folate metabolism, 5-MTHF, is an essential precursor for neurotransmitter metabolism and the synthesis of dopamine, serotonin, and norepinephrine. It is also necessary for the production of SAMe, which participates in over 200 enzymatic reactions in the body.
After 5-MTHF is produced, it is then recycled back into the cycle through the enzyme methionine synthase (MTR). This reaction requires adequate B12 as a cofactor. With B12 deficiency in near epidemic proportions in the elderly, vegetarians, chronic antacid users, SIBO, and people with ME/CFS or FM, it’s possible that folic acid can become trapped as 5-MTHF in what is called the “folate trap.” This “folate trap” prevents the recycling of 5-MTHF back to THF and slows methylation and many other downstream reactions.
Finally, there is a growing understanding of the link between hypothyroidism and proper folate cycle function. Many ME/CFS and FM patients have subclinical hypothyroidism that may be related to inadequate production of 5-MTHF. This methylated form of folate is essential for the conversion of tyrosine to thyroid hormone (1).
Who With ME/CFS or Fibromyalgia Should Be Concerned With This Study?
 It’s possible but not certain that people with ME/CFS and FM may already be behind the eight ball, so to speak, regarding folate metabolism. Dr. Amy Yasko and the late Rich VonKoynenberg proposed that genetic mutations (single nucleotide polymorphisms or SNPs) in enzymes involved in the folate methylation pathway may be common in the ME/CFS and/or FM populations.
It’s possible but not certain that people with ME/CFS and FM may already be behind the eight ball, so to speak, regarding folate metabolism. Dr. Amy Yasko and the late Rich VonKoynenberg proposed that genetic mutations (single nucleotide polymorphisms or SNPs) in enzymes involved in the folate methylation pathway may be common in the ME/CFS and/or FM populations.
Of the three enzymes involved in folate metabolism, methylenetetrahydrofolate reductase (MTHFR) plays the largest role in the conversion and utilization of folates. A genetic defect in this key enzyme could dramatically affect the ability to convert, recycle, and utilize folates.
Genetic Aspects
An Open Medicine Institute study is examining the effects of MTHFR mutations on folate metabolism in ME/CFS
Two common genetic variations, C677T and A1298C, have been identified in the MTHFR gene that codes for the MTHFR enzyme. The C677T type has been associated with increased incidence of cardiovascular disease and other health risks (4). This MTHFR SNP has been found to be prevalent in certain populations of people. Heterozygous MTHFR C677T, meaning one copy of the gene is mutated while the other is normal, is found in 42% of Hispanics, 35% of Caucasians, and 14% of African Americans. Homozygotes, where both copies of the gene are mutated, are less common in the general population with 10% preponderance (5).
I am aware of only one study that has examined this in CFS, where no association was found (7). Further research and stricter study design are certainly warranted. Another study measuring levels of homocysteine in the cerebrospinal fluid of CFS/FM patients found elevations suggestive of problems recycling folate back to methionine. However, it was unclear whether these findings were due to genetic SNPs in enzymes, folate deficiencies, or B12 deficiencies (8).
The Open Medicine Institute is currently engaged in a study to determine the extent of MTHFR mutations and the role they may play in aberrant folate metabolism in ME/CFS.
What Problems Might High Levels of Unmetabolized Folic Acid (UMFA) Pose?
If enzymatic road blocks from genetic mutations or inadequate enzyme cofactors inhibit synthetic folic acid metabolism, high concentrations of folic acid can spill over into the portal circulation.
A natural killer connection, of all things, may be possible
Elevated levels of unmetabolized folic acid (UMFA) have been implicated in increased overall mortality (9). Epidemiological studies have found a striking association between the incidence of colon cancers and folic acid food enrichment. In the US, rates of colorectal cancer began to increase in 1996 and reached a maximum in 1998. Rates have continued to exceed those present during folic acid pre-enrichment days by as much as 15,000 extra cases per year (2). Worth mentioning is that these observational studies are inadequate to determine causation due to the inability to control for all possible confounders. Nonetheless, hindsight tells us that careful study of genetic and biochemical factors should have been more thoroughly investigated before implementing a potentially harmful change in food policy.
Some studies also speculate that excess folic acid may be related to decreased natural killer cell cytotoxicity (10). This could be due to the fact that excess naturally occurring folate (DHF) blocks normal function of the MTHFR enzyme providing another potential block in methylation and other downstream biochemical cycles. More study is urgently needed to determine if synthetic folates hinder immune functioning.
What Are Your Recommendations for People Who Are Concerned?
CFS/FM patients and perhaps everyone should check their methylation status utilizing genetic testing such as 23andMe (see www.23andme.com for $99). Conventional laboratories like Quest or LabCorp also now have MTHFR studies that may be ordered by a healthcare provider. Specialty labs like SpectraCell or HealthDiagnostics specialize in more in-depth methylation studies.
(The FDA now allows 23andme to only provide raw data. Several free online tools can, however, do that job. Yasko has an excellent tool plus there’s http://geneticgenie.org/and http://www.promethease.com)
Dietary and Supplementation Suggestions
If MTHFR SNPs are found, consider avoiding all forms of synthetic folate and folic acid—including those found in grain products. (Regardless, avoiding grains due to the high incidence of gluten sensitivity in CFS and FM patients is sometimes recommended.)

Some supplement changes may be in order
Foods high in naturally occurring folate (dihydrofolate, DHF)
- spinach, turnip greens, beans, sunflower seeds, Brewer’s yeast, liver
Foods often fortified with folic acid
- breakfast cereal, bread, flour, corn meal, pasta, rice
When choosing supplements, opt for a multi-vitamin or B-complex with active forms of folate such as folinic acid or 5-MTHF. To assess if supplementation is sufficient to bypass methylation defects, routine homocysteine, folate, and B12 can be measured.
Folate is most accurately measured as red blood cell folate. Serum B12 measurements are notoriously inaccurate, so methylmalonic acid (MMA) is the preferred test to perform. If MMA is depressed and homocysteine remains high, there may be an additional need for methyl donors to recycle folate through the cycle. Supplemental methyl-B12, trimethylglycine (TMG), or SAMe may help restore normal ranges (11).
______________________________

Dr. Courtney Craig used traditional and integrative therapies to recover from ME/CFS
Dr. Courtney Craig D.C. was first diagnosed with CFS as a teen in 1998, and recovered in 2010 utilizing both conventional and integrative medicine.
Trained as a doctor of chiropractic and nutritionist, she now provides nutrition consulting and blogs about what she’s learned.Check out her latest blog “Candida Got Your Tongue?
- Check out more of Dr. Craig’s Health Rising blogs here
Support Health Rising
_____________________________________________
1 Kelly GS. Folates: Supplemental Forms and Therapeutic Applications. Alt Med Rev 1998. 3(3): p. 208-220. http://www.ncbi.nlm.nih.gov/pubmed/9630738
2 Smith AD, Kim YI, Refsum H. Is folic acid good for everyone? Am J Clin Nutr March 2008 vol. 87 no. 3 517-533. http://www.ncbi.nlm.nih.gov/pubmed/18326588
3 Patanwala I, et al. Folic acid handling by the human gut: implications for food fortification and supplementation. Am J Clin Nutr. 2014 Jun 18;100(2):593-599. [Epub ahead of print]. http://www.ncbi.nlm.nih.gov/pubmed/24944062
4 Klerk M, et al. MTHFR 677C⟶T Polymorphism and Risk of Coronary Heart Disease: A Meta-analysis. JAMA 2002;288:2023-31. http://www.ncbi.nlm.nih.gov/pubmed/12387655
5 Hughes LB et al. Racial or ethnic differences in allele frequencies of single-nucleotide polymorphisms in the methylenetetrahydrofolate reductase gene and their influence on response to methotrexate in rheumatoid arthritis. Ann Rhuem Dis 2006; 65: 1213-1218. http://www.ncbi.nlm.nih.gov/pubmed/16439441
6 Botto Lorenzo, Yang Quanhe. 5,10-Methylenetetrahydrofolate Reductase Gene Variants and Congenital Anomalies: A HuGE Review. Am. J. Epidemiol. 2000; 151(9): 862-877. http://www.ncbi.nlm.nih.gov/pubmed/10791559
7 Regland,B, Andersson M, Abrahamsson L, Bagby J, Dyrehag LE, Gottfries CG. (1997) Increased concentrations of homocysteine in the cerebrospinal fluid in patients with fibromyalgia and chronic fatigue syndrome. Scand J Rheumatol. 26(4):301-7. http://www.ncbi.nlm.nih.gov/pubmed/9310111
8 Harmon DL, McMaster D, McCluskey DR, Shields D, Whitehead AS. (1997) A common genetic variant affecting folate metabolism is not over-represented in chronic fatigue syndrome. Ann Clin Biochem. 34 (Pt 4):427-9. http://www.ncbi.nlm.nih.gov/pubmed/9247678
9 Neuhouser ML, et al. Mathematical modeling predicts the effect of folate deficiency and excess on cancer-related biomarkers. Cancer Epidemiol Biomarkers Prev. 2011 Sep;20(9):1912-7. Epub 2011 Jul 13. http://www.ncbi.nlm.nih.gov/pubmed/21752986
10 Troen AM, et al. Unmetabolized folic acid in plasma is associated with reduced natural killer cell cytotoxicity among postmenopausal women. J Nutr. 2006 Jan;136(1):189-94. http://www.ncbi.nlm.nih.gov/pubmed/16365081
11 Olthof Margreet, Trinette van Vliet, Esther Boelsma, Petra Verhoef. Low Dose Betaine Supplementation Leads to Immediate and Long Term Lowering of Plasma Homocysteine in Healthy Men and Women. J. Nutr. 2003 Dec. 1; 133(12): 4135-4138. http://www.ncbi.nlm.nih.gov/pubmed/14652361



I had the test and there is a problem in one gene. What does this mean and what can I do? I am sufferer of Fibro for 32 years.
Shelia,
It really depends on which gene is mutated. Also certain mutations work by slowing down enzymatic processes while others speed them up. Knowing which enzyme is involved can help you and your clinician know what supplemental co-factors may be beneficial and in which forms.
I have taken the test and have reason to be concerned. I have spent some time trying to find a multi-vitamin that has folinic acid or 5-MTHF and have had no luck. Do you or anyone else know of any?
Thanks,
Life Extension might have one.
Dr. Craig mentions that “CFS/FM patients and perhaps everyone should check their methylation status utilizing genetic testing such as 23andMe”. However, won’t genetic testing just tell you the genetic predisposition to having difficulties within your methylation cycle? Based on posting from the late Dr. Rich Van Konynenburg, wouldn’t functional testing be more important or as important as genetic testing? I know he referenced the Methylation Pathways Panel test, available by a lab in the US, as one source of this test. From what I understand, the test will reveal several indicators of the various forms of folate in the body, among other variables, such as glutathione levels. I do appreciate the purpose of genetic testing, since that may shed light on what potential issues to watch out for. And, I’ve seen a posting on Ben Lynch’s mthfr.net website where both the merits of genetic testing and functional testing are discussed. But, I would think that the functional test, albeit an expensive test, is the best way to assess one’s methylation status, vs. one’s genetics predisposition to having methylation issues. I would certainly appreciate other’s feedback from those who have had either test.
I agree that genetic testing is a static way to assess and doesn’t measure the dynamic, functional aspect of a patient’s methylation. I recommend Health Diagnostics towards the end of the article above. They are based in NJ and offer a Methylation Pathway analysis that measures blood folates, GSH, and other markers of methylation functional status. It’s a good routine test to run to see if a methylation supplement protocol is working. This is the test Rich VonK recommended as well.
Check out the MTHFR.net site, which may be Dr. Ben Lynch’s (Naturopath), and see the store items. Choose carefully; some (like Methyvorin) have ingredients that are verboten if one has more than a MTHFR methylation issue. Yasko’s own HH Multivitamin with folate is designed for the most common multiple mutations; they advise starting out with only the amount from one capsule that will fit on the end of a flat toothpick. The stuff is potent and over- or under-methylation must be avoided when a person takes medicines or supplements for this purpose.. CFS_Yasko Yahoo groups, MB-12 site and the Borrelia/Autism Yahoo group have wonderful posts where people share their experiences and resource bases with all these complex methylation issues and tests, not just the MTHFR. So does Dr. Yasko if someone has taken her Nutrigenomic Liver Methylation Test, the one that started this entire trend in epigenetic/Nutrigenomic healing. From my many years of research, this information holds some very important keys for healing Neuroendocrine Immune Diseases, and these tools have been available only in the last few years. Quick fixes are not realistic, low-dose experimentation is definitely indicated, and the info can be complex, but it could be that the world immunology community may be making some gains in getting solidly vetted info to the public on the connections among NIDs/M.E., methylation, environmental health, and natural lifestyle and successful healing. A wonderful, concise article was presented here by Dr. Craig and Cort.
Thanks Jeanette.
Dr. Lynch’s website is a great resource for those who want to know more. He includes many references to the research throughout his posts for anyone who wants to dig deeper.
Isn’t sublingual B12 recommended for all ME/CFS patients?
I am going to be doing the nutrition part of a clinical study on the methylation cycle. It will be an alkaline diet wtih alkaline supplement and either methyl folate of methyl B-12 depending on the gene mutation. I found this link on MTHFR very interesting and thouht it might provide more enlightment for your readers. I personally know at lest six people with chronic fatigue and fibro that have this gene mutation. http://www.methyl-life.com/a-doctor-explains.html
Kindest regards Patty
Fibro and CFS have left me confined to bed on an average of 4-5 days per week these days. I’m coming up on 5 years since my diagnosis. I just turned 40 years old and I have very little quality of life these days, so I cannot tell you how much I appreciate this site and each article that gives me hope of a cure or even a better quality of life. I now have another new test to take to my doctor. I don’t think I’m alone when I say that some days hope of a cure is the only thing that keeps me going. For that I can’t tell you enough, Cort and Dr. Craig, I thank you so much, and Dr. Craig, I very much look forward to reading more of your blog as well. I plan to make a donation to your site a part of my monthly budget, I’m thankful for now receiving disability, so hopefully every little donation helps. Love this site!!
I am homozygous for the MTHFR 1298C mutation. I have had CFS for 25 years, and had lung cancer last year even though I am a non-smoker. I am taking Deplin L-Methylfolate 15 mg. per day and 5 MTHF activated. What else should I be doing?
My husband is also homozygous for the MTHFR 1298C mutation, thus our two sons are also both homozygous. One takes Deplin and one doesn’t. Any advice for additional testing or treatment would be greatly appreciated, especially in light of my recent history of lung cancer.
Thanks,
Cathy Gee
Sounds complex, Cathy. I’ll point you to the expert panel Cort has put together. May be able to give you more insight:
http://www.cortjohnson.org/chronic-fatigue-syndrome-mecfs-doctor-resource-center/ask-mecfs-fibromyalgia-expert-panel/
Hi,
I have the heterozygous MTHFR A1298C mutation which does not seem to be related to folic acid metabolism, however I am low B-12 and hypothyroid. I have been taking 50mcg of synthroid since 2000 which seems to be working well but recently my homocysteine levels have been borderline and slightly elevated. My Doctor says there is another genetic mutation that interferes with the conversion of cyanocobalamin to methylcobalamin. I have not been tested for this and don’t recall what the gene is, however I think he knows what he is talking about so I am starting taking the methyl form of B-12 as soon as I get my hands on it.
He also recommends stopping all other B vitamin supplements. He thinks there is a risk of getting too much B-6 and that can be detrimental.
Your blog addressed the folic acid metabolism and identified B-12 as a necessary co-factor, apparently in recycling the 5-MTHF back to THF but if you addressed increasing B-12 as an approach I missed it.
Since this seems related to the approach I am embarking on I would appreciate any insight,
Thanks,
Greg
There are several good multi-vitamins out there with MTHFR and p5p etc. pure encapsulations has one as does ProThera/klaire.
Debbie
I have homozygosity for 677(+/+) which results in 60% – 70% reduction in MTHFR enzyme activity A1298C Genetype. I am currently taking Vit B6 sulphate, folinic acid and methycobalamine. Should I now drop the Vit B6 sulphate? Should I be taking anything else with these supps to aid in my methylation.
I have had ME/FM for 8 years and live in South Africa so have difficulty in obtaining the right labs. Any assistance would be helpful.
Tested positive for homozygous C77t (Quest labs) and have been taking Seeking Health: “Homocystex Plus” from Dr Ben Lynch daily for over a year now. Works very well for me. You need to start slowly and increase slowly. Have ME/CFS and hypothyroidism.
Be well!
Could you please clarify the “Gut Check” paragraph?
The study you referred to was done on only 6 people, how can we draw conclusions from that?
In that same paragraph you say the study compares folic acid to 5-MTHF, but the study compares folic acid to folinic acid.
So maybe I’m looking at the wrong study?
Any article that suggests Folinic Acid is more beneficial than Folic Acid because it bypasses the MTHFR step is WRONG.
The only form unaffected by MTHFR is methylfolate.
However, many (properly conducted) scientific studies have shown that supplementation with plain old Folic Acid does increase serum folates and, more importantly, decrease homocysteine levels in all variations of the MTHFR alleles.
Although homozygous MTHFR does mean REDUCED conversion it does not mean ZERO conversion.
Note that homocysteine levels can only be reduced (when considering the folate pathway) if the folate has been converted to methylfolate i.e. this demonstrates that THF to methylfolate conversion is happening in all genotypes.