


A recent analysis on Health Rising of 11 recent ME/CFS studies pointed to two main themes – one of which involved the blood vessels. Recently, a nicely sized (n=94) long-COVID study from Mass General Hospital (Harvard), titled “Endovascular profiles linked to neutrophil activation in children and young adults with long COVID“, dug deep into that question.
How important is blood vessel damage in long COVID? The short answer: possibly very important but not in every patient.
It’s also a rare study that included children and young adults (< 25 yrs) and determined whether the coronavirus spike protein could be harming the blood vessels.
That last focus by itself is potentially a very big deal. In their recently published review article, “Virus-induced endothelial senescence as a cause and driving factor for ME/CFS and long COVID: mediated by a dysfunctional immune system“, Nunes and Pretorius proposed that an acute viral infection (not limited to the coronavirus) could be harming blood vessels found everywhere from the blood-brain barrier, to the blood vessels in the brain, to the gut and the skeletal muscles in ME/CFS and long COVID. (Talk about a systemic problem!)
 Health Rising’s Quickie Summer Donation Drive is On!
Health Rising’s Quickie Summer Donation Drive is On!The GIST
-

Almost all the neutrophils in the long-COVID group have formed NETs to capture pathogens, toxins, and other threats.
A recent analysis on Health Rising of 11 recent ME/CFS studies pointed to two main themes – one of which involved the blood vessels. Recently, a Harvard study focused on young adults and children with long COVID dug deep into that question.
- We rely on our blood vessels to deliver energy (oxygen) and nutrients to the tissues, to build new muscles, to cleanse the tissues, including the brain, of toxins, and to direct the immune system to areas of infection.
- The study found that large microclots, in particular, were more common in the long-COVID patients. These microclots could be gumming up the small blood vessels that deliver blood directly to the tissues.
- It suggested that a broad-scale endothelial remodeling had taken place, resulting in damaged, pro-inflammatory, vasoconstriction-oriented blood vessels. This “remodeling” may have taken place during the cytokine storm that occurred during the initial infection.
- The lack of adhesive markers, though, which would have indicated that the blood vessels were calling the immune system to attack the virus, suggested that the virus was not present in the blood vessel walls.
- Instead of being caused by an active virus, it appeared like the damage was “locked in” by different factors that were reinforcing each other.
- This study expanded the endothelial situation in long COVID by assessing the production of a fascinating process called NETosis (neutrophil extracellular traps (NETs).
- In NETosis, immune cells called neutrophils sacrifice themselves to form nets that trap pathogens, toxins, and free radicals. They only go to this length when the danger is so high that the best option is to sacrifice themselves in order to build these sticky traps. One downside of the NETs is that they promote the formation of more clots.
- Culturing the long-COVID patients’ blood in the lab resulted in an explosion of these “NETs”. Few NETs, on the other hand, appeared in the healthy controls’ blood (see blog for images).
- In the lab, the authors showed that the spike protein plus neutrophils resulted not just in a damaged but in a leaky endothelium. This is important because a leaky endothelial layer in the blood vessels could impact blood flows and harm the blood-brain barrier.
- The blood vessel findings highlighted a major factor in long COVID, but they explained only about half of its causes. They were also quite heterogeneous; i.e., the long-COVID group of patients exhibited a variety of blood vessel findings.
- This is no surprise for diseases like long COVID and ME/CFS, which typically contain a wide range of patients with differing biologies.
- In what may be its most significant finding, the study identified a subset of long-COVID patients with particularly severe blood vessel problems. If these findings are validated, this patient group would be ripe for clinical trials aimed at improving blood/blood vessel health.
- A good next step might be to use an exercise test to stress the blood vessels and then measure markers of endothelial dysfunction, microclots, and NETs. etc., that this study found, as well as blood flows.
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit
The Mighty (or Not So Mighty) Blood Vessels
We rely on our blood vessels to deliver energy (oxygen) and nutrients to the tissues; to build new muscles; to cleanse the tissues, including the brain, of toxins; and to direct the immune system to areas of infection.
As we work our way through this series, we’ll see that several components of the blood vessels may be affected in long COVID and ME/CFS.
This study focused on the endothelial layer lining the blood vessels, as well as clotting and other factors.
Blood vessels are composed of a thin line of endothelial cells perched on a basement membrane, which is surrounded by smooth muscle (pumping action) and finally an outer connective tissue layer.
The endothelial cells are the great workers of the blood vessels. They’re responsible for opening (nitric oxide) or closing the blood vessels (endothelin-1) to increase or reduce blood flows.
In the blood-brain barrier, they form the tight junctions that limit unwanted substances from reaching the brain. Like leaky gut, a leaky brain barrier could be causing toxic/damaging substances to end up in the wrong place. They also play a key role in something called “neurovascular” coupling, which ensures that more active areas of the brain get the blood/oxygen they need. It’s pretty clear that neurovascular coupling is impaired in these diseases.
The Study
The researchers also wanted to get as complete a picture as possible of the immune situation in the blood vessels. By doing so, they demonstrated the fundamental role the blood vessels play in the immune system. When confronted with signs that a virus is present, that damage has occurred, that cells are under stress, or that low oxygen levels are present, the endothelial cells lining the blood vessels secrete adhesive factors that direct the immune factors to that spot.
The swelling you experience when you have an injury is caused by the endothelial cells secreting substances that allow immune factors to flood the area and produce inflammation. The clots endothelial cells promote produce more inflammation. Other factors they express encourage platelet activation – another source of inflammation.
Immune factors that affect the blood vessels in various ways were assessed.
The blood vessels, then, are a very big deal in the immune system. First, the authors examined immune factors, called cytokines, produced in three ways: by endothelial cells, by immune cells in the tissues surrounding blood vessels, and by leukocytes, which typically enter the blood vessel walls themselves when inflammation is present.
The study also took a deep dive into immune cells called neutrophils (which are often involved in clotting). It checked out microclots as well.
Finally, it determined whether the coronavirus spike protein (the part of the virus that enters cells) might be responsible for the endothelial issues observed. To do this, they cultured human endothelial cells to form a blood vessel layer, and then incubated them with neutrophils that had been exposed to the spike protein (and its immune complex).
Results
Microclots – Check!
For the first time, a study assessed microclot formation in young people with long COVID and found them – in spades. The high probability factors (p = 0.0003; p= 0.0073, p = 0.0051) associated with the various measurements indicated that large microclots, in particular, were commonly found in the long-COVID patients but rarely found in the healthy controls.
Broadscale Endothelial Remodeling
A correlation matrix of the various endothelial factors assessed found that they were “coordinated”; i.e. the abnormal readings reinforced each other, which is what we want to see. (We want to see changes across an entire process.)
They indicated that a broad-scale endothelial remodeling had taken place. The unique “endovascular profile” the study uncovered suggested that microclots and activated platelets are tweaking the endothelial cells and vice versa in long COVID; i.e., a vicious circle was present that was locking in the blood vessel problems.
A cytokine storm early in the infection may have damaged the endothelium.
As so often happens in these diseases, some unusual findings popped up. The elevated adhesion markers that would have indicated immune cell infiltration of the endothelial walls were not detected. That was a bit surprising, as immune cell infiltration is often seen in conjunction with the microclot/platelet findings.
If I’m reading this right, it appears that the coronavirus infiltrated the endothelium during the acute infection. That infiltration caused the immune cells to chase after it, producing a cytokine storm; i.e. an inflammatory state in the endothelium.
The inflammatory state in the endothelium, however, is gone. There were no signs that immune cells are being directed to enter the endothelium. At least in the endothelial layer, the virus had apparently been vanquished.
That may seem like a good thing, but we may actually have a worse result: an endothelium may have survived a perhaps massive injury but has been left in a long‑lived, dysfunctional state.
The endothelial cells controlling the blood vessels are not dying, but they’re also not healthy. Instead of cleanly and calmly opening and closing the blood vessels and sending the blood to where it’s supposed to go, the damaged endothelium is having trouble vasodilating (opening) the blood vessels, is prone to close them down (vasoconstriction), has likely stiffened the blood vessels, has damaged mitochondria, and is pumping out pro-inflammatory cytokines and reactive oxygen species (free radicals), and supporting the production of clots.
A better result might have been if the damaged endothelial cells had simply died and been replaced. Instead, we may have bunch of irritable, twitchy and impaired endothelial cells and stiff, inelastic, poorly functioning small blood vessels lining the brain, muscle, and autonomic tissues.
A SASP Disease?
This state is not unknown – it’s called the senescence‑associated secretory phenotype (SASP). In fact, some viruses push cells into senescence because they’re pretty poor at resisting viruses in that state.
Senescent, pro-inflammatory, vasoconstricted blood vessels may be present in some long- COVID patients.
Since the SASP state has been well characterized, an important question is whether test results indicate its presence in ME/CFS and/or long COVID. The authors listed 7 factors indicative of a SASP state that have been found in these diseases.
The authors didn’t stint on the possible problems a senescent, damaged endothelium could be causing in ME/CFS and long COVID. They could be impairing both arterial and microvascular blood flows in the central nervous system, gut, muscles, etc. Even the immune system is not, er, immune from the potential blood flow problems.
The upshot is a cardiovascular system that can’t move the blood to where it needs to go during exercise, cognitive exertion, standing, etc. While the same type of study has not been done in ME/CFS, proteomics and endothelial studies suggest that a similar SASP process may be occurring.
Because a variety of viruses, including the coronavirus and herpesviruses, can infect endothelial cells, the SASP could be induced by many viruses. If an infection didn’t start your disease off, don’t worry! An inflammatory state caused by something else can start this process off. One wonders, once again, if, at their core, these are all, one way or another, blood-flow diseases.
Trapped in NETS
This study expanded the endothelial situation in long COVID by assessing the production of a fascinating process called NETosis (neutrophil extracellular traps (NETs).
In NETosis, immune cells called neutrophils sacrifice themselves to form nets that trap pathogens, toxins, and free radicals. They only go to this length when the danger is so high that the best option is to sacrifice themselves in order to build these sticky traps.
We know exactly how this process occurs. First, neutrophils produce a large burst of reactive oxygen species (ROS), which triggers the production of enzymes that degrade the chromosomes. Eventually, the chromatin responsible for packing our DNA tightly away begins to unfold…and the neutrophils basically explode, producing large, sticky nets.
The researchers used various means to show that these NETs were likely damaging the endothelium
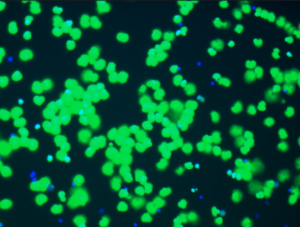
Check out some images from the videos in the paper. The neutrophils are blue dots. After five seconds, they remain stable in the healthy controls, but self-activate and produce nets (green splotches) in the long-COVID patients. First, they swell, then they burst open and release their DNA, which ends up producing the “NETs”. (High levels of cell-free DNA were associated with the NETs.)
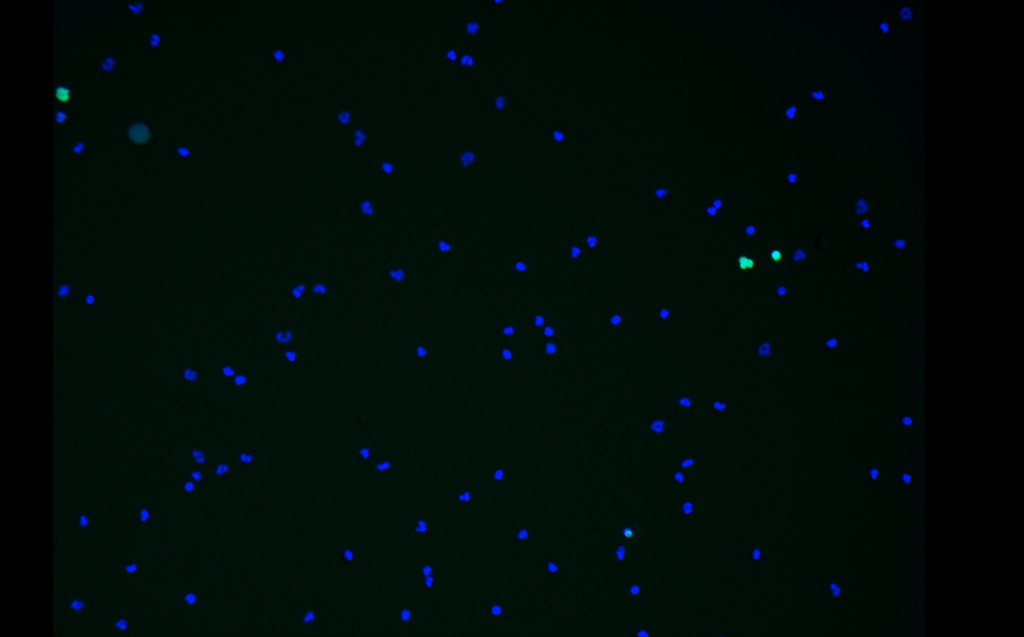
Stable neutrophils in the healthy controls. (Four small NETs (green dots) produced).
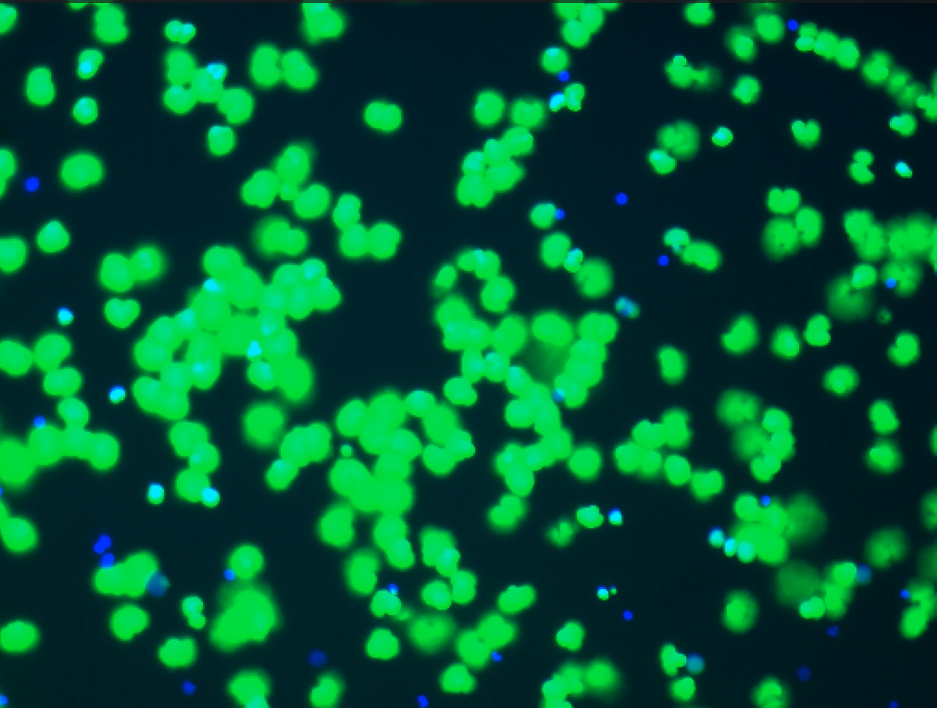
Almost all neutrophils in the long-COVID patients formed NETs to capture pathogens, toxins, and other targets.
Note, again, that they’re doing this without being triggered by the spike protein. They’re in such an unstable, active state that they kind of explode!
These extracellular explosions of DNA form (with fibrinogen, platelets and proteins) then form the structural backbones of the microclots found in long COVID, can damage the endothelial cells, particularly impair blood flows in the microvasculature (smallest blood vessels), and produce a low energy state, etc. They are also major drivers of the innate immune system drivers.
Nobody has looked for “NETs” in ME/CFS yet. The data to date suggests they’re probably there, but even if they’re not, note that they are not necessary to produce the blood vessel problems found thus far. They could simply be amplifying problems that are already there.
Assessing the impact NETs may be having on ME/CFS would seem like the next logical step and should not be too difficult: simply assess NET markers, microclot levels, and endothelial function, particularly at the microvascular (small blood vessel) level.
Spiking Endothelial Dysfunction?
The spike protein (red projections) of the coronavirus produced endothelial damage – when paired with neutrophils.
In the lab, the authors showed that the spike protein plus neutrophils resulted not just in a damaged but in a leaky endothelium.
While the paper showed that the spike protein produced microclots, spike-negative patients also exhibited microclots, indicating that some factor other than the coronavirus spike protein may be producing them.
An upregulation of serum amyloid P, which activates the complement system, which activates mast cells, and could be attacking the connective tissues in long-COVID patients, without the spike protein, provided another way to produce endothelial damage in people who no longer carry the spike protein in their blood.
A Subset Pops Out
(I asked Perplexity Pro, ChatGPT Pro, Gemini Pro, and Claude to assess the results section, which described the author’s attempt to differentiate long-COVID patients from healthy controls using the endothelial findings.
The answers followed a familiar pattern. ChatGPT Pro, Perplexity Pro, and Claude provided long answers that pointed out the pros and cons of the results. Claude pointed out that because the authors didn’t report things like AUC, sensitivity, specificity, and accuracy, we can’t tell if the results are clinically useful, and the authors noted this: “The clinical consequence of increased microclots and altered endothelial phenotypes is not yet known.” Gemini Pro provided a shorter answer, which emphasized the positives and missed most of the negatives.)

The most important finding may have been a subset of long-COVID patients with markers of increased endothelial dysfunction, clotting, and NETs.
The short take is that, despite the intriguing endothelial findings, the biomarkers the authors used to separate long-COVID patients from healthy controls explained only about 50% of the variance; i.e., they explained only about half of what causes long COVID.
That’s a moderate finding, which suggests that while the study captured an important feature of long-COVID biology, there’s clearly more to the disease. The upshot is that you couldn’t use these biomarkers to differentiate people with long COVID from healthy people.
Nor do we yet know how clinically important these findings are. The authors warned that more study is needed before anticoagulant therapy is used in long COVID.
This is not surprising, however. Long COVID (and ME/CFS) are highly heterogeneous diseases, and, not surprisingly, the endothelial findings in the long-COVID group were similarly heterogeneous. They were more prominent in some people and not prominent in others. This is what we would expect to see in any study that doesn’t stratify patients by biology.
The authors were able to identify a subset of long-COVID patients with elevated levels of endothelial markers (microclots, cfDNA/NETosis, P-selectin, PF4, VEGF-C, and HB-EGF) – and this is probably the paper’s key finding.
A major goal of all ME/CFS and long-COVID studies at this point must be to identify subsets, and that’s what this study appears to have done.
This group of patients can be assessed further and, if the findings hold up, should be ripe for clinical trials.
Possible (Mostly) Future Treatments
A wide variety of treatments are available should these findings be validated. Since some involve strong drugs, further studies would need to be done, and the authors specifically warned against using this study as a reason to initiate a treatment.
Since authors demonstrated in several ways how NETs may be involved, they probably present the most likely short-term treatment opportunity. Several treatments could inhibit the production of NETs (DNase enzymes, platelet–neutrophil interaction blockers (P-selectin inhibitors, PSGL‑1–targeting agents)) or eliminate NETs (colchicine, some statins, or PAD4 inhibitors).
Anticoagulants are probably the most contentious therapy, given the possibility of side effects, but they might be helpful with microclots in some cases.
One study found that L‑arginine plus vitamin C improved blood flows and fatigue in long COVID. Hyperbaric oxygen therapy (if done enough times) can be helpful for some people and may improve blood flows.
Next Stop – An Exercise Stressor?
Using exercise to stress the blood vessels and assess biomarkers and microvascular functioning would seem to be a logical next step.
Because exercise is essentially a stress test for the blood vessels (as well as the metabolism, autonomic nervous system, and immune system), the next step might be to assess the effects of exertion on endothelial health, particularly in the subset identified. Instead of using healthy controls, it would also be best to use recovered COVID-19 patients as the control group.
In addition to the markers assessed in this paper, a study that directly measures blood flow, brain and/or muscle oxygenation, and autonomic nervous system function before and after exercise would provide a clearer picture of the role blood vessels play in these diseases.
In conclusion, this study found that microclots, endothelial injury, NET formation, and vascular remodeling occur in young people with long COVID, and that a subset of patients are particularly affected. It should open the door to larger and more expansive studies that assess the possible biomarkers found, and their effect on symptoms, blood flows, etc., particularly in the long-COVID patients with increased levels of endothelial biomarkers uncovered in this study.
This study opened up a bunch of other possibilities that may be in play in Part II of this series:
- Down to the Basement (Membranes) We Go
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit


This is a great conference line up coming up this week. The Germans, in particular, are very active!
https://events.mecfs-research.org/en/events/conference_2026/agenda#1
No kidding – a whole section on the vascular system (a German speciality) and how about that Michelle James presentation on whole body PET :). Is it open to the public? I don’t see any opportunities to register.
You can do online registration, I did it yesterday.
I think this is the most exciting conference line up I have seen for many years.
Michelle’s sounds intriguing, and I am especially interested in the presentations on neuroinflammation and neuroimaging, as I think the brain and it’s interplay with the immune system is by far the most likely core issue with these illnesses.
It’s great to see some new and fresh names in the field.
Yes, lots of new names particularly, out of Europe! Some people are very excited about James as well. I found it and registered – thanks!
The vascular remodelling is what i feared. I mean that sounds like lasting damage no?
It does sound rather daunting but if inflammation can be reversed maybe the blood vessels can calm down and heal. If they’re loaded with too much fiber – the subject of the next blog – maybe it can be broken down…
I believe it can be broken down for sure.
But vascular remodelling, that’s surely going to be hard.
But let’s be hopeful that smthg comes up eh?
Good research papers and good write up Cort. Netosis and microclots and there impact *in capillaries* have been for some time on my radar and I speculated here on them before. Nice to see some actual data popping up!
Netosis and ‘stuff being clogged in these NETs’ is likely to provide a potent way to reduce blood flow and oxygenation *in capillaries*. I stress ‘in capillaries’ because they’ll have their greatest impact in capillaries who are already very narrow and less in the bigger blood vessels. It’s also important to stress ‘in capillaries’ because I believe it keeps this hypothesis standing in both the high bloodflow subgroup (microclotting mostly limited to capillaries) found in ME/CFS and the low bloodflow (microclotting becoming less micro and flowing over to bigger blood vessels) subgroup in ME/CFS.
With poor oxygenation, any sort of exertion will cause extra stress on cells and mitochondria. Even a bit will be too much. Mitochondrial DNA and oxydized mitochondrial DNA is likely to be released when (even a little exertion) is too much. Paper confirming increased mitochondrial release (found as increased mitochondrial DNA found in exosomes in blood) in ME/CFS: https://onlinelibrary.wiley.com/doi/10.1111/ejn.15828 with title “Exosome-associated mitochondrial DNA from patients with myalgic encephalomyelitis/chronic fatigue syndrome stimulates human microglia to release IL-1β” saying “Here, we show that mitochondrial DNA (mtDNA) associated with serum exosomes, is increased in ME/CFS patients only after exercise.”
=> released mtDNA stimulates microglia (the immune cells in the brain) and is only increased *after* exercise / exertion. So likely part of (time delayed) PEM cascade.
In addition, released mtDNA itself is increasing endothelial damage. See paper https://www.sciencedirect.com/science/article/pii/S153718912100118X with title “Mitochondrial DNA and TLR9 activation contribute to SARS-CoV-2-induced endothelial cell damage”
=> So a possitive (despite the word, that is bad just like having a possitive Covid or cancer test) feedback loop is reinforcing the issue… …after (over)exertion.
The last paper says “promoted mitochondrial dysfunction, i.e. it increased mitochondria-derived superoxide anion, mitochondrial membrane potential, and mtDNA release, leading to activation of TLR9 and NF-kB, and release of cytokines. SARS-CoV-2 also decreased nitric oxide synthase (eNOS) expression”. This is one of many sources that says released mitochondrial DNA can activate TLR9 receptors.
TLR9 activation itself can, among many other inflammatory things, promote NET formation / netosis. That further reinforces the feedback loop / vicious circle. See paper https://pmc.ncbi.nlm.nih.gov/articles/PMC9222025/ saying “Following ischemia–reperfusion injury (IRI) in the murine liver, a dose-dependent increase in NET-specific markers in response to histones was observed. This effect was dependent on TLR4 and TLR9 on neutrophils.”
In this paper they are mainly concerned with (NET formation due to) TLR9 activation by histones and cfDNA (cell free DNA) released from cellular damage due to ischemia / reperfusion but here I limit to discuss the effect of released mitochondrial DNA on the TLR9 receptor.
=> After exertion, mtDNA is increased in ME/CFS patients. That increases TLR9 activation also on neutrophils, leading to increased NET formation / netosis. That reduces blood flow and oxygenation, making the next exertion even more difficult. That further lowers the threshold for exertion in ME/CFS before mitochondrial DNA is released in the blood.
My take:
=> after many types of infection, resting longer for quite a time is needed even if the pathogen is erradicated. That idea seems ‘to be out of fashion’. More then a few doctors held too long the believe that once the pathogen is erradicated you can no longer experience symptoms and are good to go full speed again. This shows there is lingering damage that can take quite some time to resolve *after* the last bit of pathogen is erradicated.
=> the difference between ‘normal’ gradual recovering after infectious disease and getting long Covid / ME/CFS *might* mainly be found in what types and percentage of cells in the body are ‘over their best date / senescent’. In the early phase, it may be mainly the endothelial cells at the site of infection that are senescent. Note that Covid targets all endothelial cells around the body, increasing the spread of the problem in the early phase compared to pathogens that target a single organ. With it, Covid is one of the pathogens that yields a greater chance of getting into the long phase by starting with a far larger percentage of senescent endothelial blood vessels early on.
=> In the later phases, more and more cell types are not getting replaced at the normal rate *IF / WHEN* the body goes into inhibitting mode as a way to try and resolve the problem. The more cells that are senescent, the more cells that will release mitochondrial DNA upon exertion and amplify the problem. As some cell types have normal replacement rates of multiple days (like many endothelial cells) while others have replacement types of weeks or months or years or never, it’s easy to see that endothelial cell types go senescent first and others to join senescence over months or years.
=> So in this view, *part* of ME/CFS (or long Covid) is a process that is not exceptional but normal: everybody recovering from a strong infection is going trough it. The difference is wether you succeed first in preventing a localized vascular endothelial problem to expand all over the body and later to other cell types with longer lifetimes too. The bad news: the more the problem expands over time, the harder to try and reverse it just like we see with chances of getting out of ME/CFS over time.
The very short summary:
*NETs in capillaries reduce blood flow and oxygenation.
*exercising too much with reduced blood and oxygen flow will release damaging stuff (like mitochondrial DNA) from exerting cells.
* that in turns creates brain inflammation by triggering the brain’s microglia.
* that also triggers more creation of NETs in capillaries, increasing the clogging in them after each over-exertion.
* so it is perfectly normal to have lingering symptoms after many types of infection even if there is no more pathogen. the above provides a mechanism.
* the main difference between recovering quickly and getting into ME/CFS may be that the recovering people succeed in preventing a locallized / smaller problem to expand all over the body while the latter do not. Exerting while ill or shortly after it might increase that risk.
* the more the problem is spread all over the body (typically after longer duration), the harder it becomes to recover.
Great summary!
Thank you for the short summary.
Look at all these potential connections!
The interesting thing is that https://pmc.ncbi.nlm.nih.gov/articles/PMC8924116/ finds strong netosis in active / acute Covid19.
It says “Abundant NETosis and NET generation have been observed in the neutrophils of many COVID-19 patients, leading to unfavorable coagulopathy and immunothrombosis. Moreover, excessive NETosis and NET generation are now more widely recognized as mediators of additional pathophysiological abnormalities following SARS-CoV-2 infection.”
=> So we sort of have a *continuum* in many patients.
Abundant netosis observed during active infection (this citation). Abundant netosis observed during long Covid phase (the paper you linked in the blog). And increasing indications of excessive netosis following (sounds shortly to longer after) Covid infection (this citation).
See the lack of gap, the lack of need of a change in underlying mechanism for trouble from initial Covid infection all the way to long Covid? I find that very interesting!
It looks a lot that (part of) the initial tool to solve the infection (NET formation) just remains there causing trouble for some time after the infection for both recovering and non-recovering patients and ‘just’ remains there for those that do not recover.
Part of the initial tool needed for getting rid of the infection seems to become part of what gets stuck. Now that idea is interesting as this mechanism does NOT ONLY involve the minority that does get into long-Covid (or ME/CFS or chronic lyme…) but ALSO those dying from the infection itself or those that have half their lungs permanently filled with fibrosis.
The ones that died had the tool not up to the task of saving them without getting them killed, and in Covid most died from the own immune system overacting rather then from the virus itself.
The ones that got into long-Covid got the tool activated and most of them very likely succeeded to erradicate the virus. Unfortunately the tool was activated in a way that part of it can’t deactivate so the patient remains ill only in a different way.
=> So studying IN DEPTH now the own immune system resolves this infection and how the immune system tries to restore to neutral after infection and when it gets stuck forrever overlap. Studying one learns more about the other.
Since the immune systems of people with ME/CFS and likely long-Covid seem to be ‘experts’ at being prudent and preventing permanent damage, it offers researchers that see this a lot of opportunity to learn how to heal better from strong infections with less dying and extensive permanent (lung) fibrosis. Now THAT is a reason to invest heavily in studying long-Covid and ME/CFS.
If the spikes damage the endothelial cells, that is bad news. And to think that the mRNA vaccine actually stimulates the cells in your body—not just in the arm muscle—to produce these spikes. It is known that even two years after vaccination, these spikes can still be found in the body in places where they were not supposed to be.
That is an extra risk with every vaccination you take. The virus itself, of course, is also a risk. The phenomenon of sudden death among young people and athletes, which is still seen, could also be related to this. Anyway, blood flow problems could explain everything. This has been known for a very long time in ME/POTS. I do not know if studies that have been done on ME or long-COVID patients with blood thinners and its effect.
Regenerative medicine is the only hope for a cure if youre severely effected surely? Anti purigenic therapies. Perhaps some kind of crispr repair down the line.
Until then its anti coagulant therapies and what else?
Pro resolving mediators both limit acute inflammation and promote resolution and return to homeostasis following infection or injury. There is growing evidence that chronic immune disorders are characterized by deficiencies in resolution and SPMs have significant potential as novel therapeutics to prevent and treat chronic inflammation and immune system disorders.
Specialized Pro-resolving Mediators as Modulators of Immune Responses
https://pmc.ncbi.nlm.nih.gov/articles/PMC9962762/
Yep ” explode” is what I felt was happening inside my body.
Massive explosions in the beggining, then I felt my body rest and get ready for the next fight,then rest,then fight….this went on for aprox.one year,until my immune system could no longer fight.
I had no idea a person could become this ill…NOW PTSD along with many other issues…35 yrs in
I am wondering if people who never recover from a pathogen is that their body doesn’t have the ability to resolve the inflammation.
“To ensure timely resolution of acute inflammation, neutrophils need to be disarmed and removed from the affected sites. Resolution of inflammation is an active process governed by specialized pro-resolving lipid mediators (lipoxins, resolvins, protectins, and maresins), proteins (eg, annexin A1), and gaseous mediators (eg, hydrogen sulfite and carbon monoxide), which predominantly act on phagocytes and other immune cells.”
https://pmc.ncbi.nlm.nih.gov/articles/PMC8867684/
My view is that it is a neuroinflammatory process that is the main culprit. That will be impacting all manner of things, including neurotransmitters. And downstream things.
jarred Younger mentioned last year that his recent work is really showing neuroinflammation. Not sure when he will publish that.
I am very interested in the trial of bezisterim for long covid. Apparently its mode of action is on neuroinflammation. The trial results for long covid are due out within the next few months.
*IF* there is a resting state in ME/CFS that is low enough on oxygen, then every attempt to exercise too long and too much risks to either:
A) create rather excessive lactate buildup if the vaculaire in the working organ fails to provide enough oxygen; that excessive lactate buildup then would come with it’s own set of problems
B) create conditions of a strong local increase in oxygenation, for example by sudden vassodilation due to immune cells locally dumping lots of strong vassodilating chemicals like histamine. That strong immune reaction needed for it in itself would cause side effects, but the main problem IMO is this: this (rather poor oxygenation before exertion and a strong bump in oxygenation during it) in itself would be akward close to ischemia / reperfusion damage.
In option B), some amount of the ‘full scale’ Ischemia / Reperfusion damage (often noted as I/R damage) is IMO likely everytime you go from long (need to) rest to too strong exertion. And part of I/R damage is caused (and resolved) by… …(new) neutrophils infiltrating the tissue. Once there, a lot of them will remain there a lot longer then expected as they’ll quickly find themselves in a low oxygen environment once you need to stop exertion. And hypoxia (shortage not lack of oxygen) causes neutrophils to have abnormal long lifespans. They sort of inhibit and extend lifespan in harsh environments too. And when exerting too soon the next time… …they IMO lay there waiting like burried land mines.
So cleaning up the old NETs is IMO only part of the work so long too often new ones are produced.
For sure cleaning up old NETs is only part of the work.
Hypoxia is involved in so many of the pathways that are affected in pwME/CFS, not sure about Long Covid as I’m not as familiar with it, but I would imagine it’s involved in long covid, too.
May I add that SARS-CoV-2 causes damage to the glycocalyx, which affects shear stress, and shear stress can also cause NETosis.
“Increasing evidence supports that NETosis is a regulated, signaling-driven process, and that mechanical forces—including shear stress, tensile force, and matrix stiffness—can act as noncanonical danger signals capable of inducing NETosis.”
So once the glycocalyx is damaged, that could be a continuing cause of increased NETosis. Blood flow, especially to capillaries, is affected by damaged glycocalyx, which of course also reduces oxygen delivery.
I have to admit that it’s late in the day and I lose comprehension ability when I’m tired. so I will need to reread Cort’s article and your comments, dejurgen. Interesting input.
I thought the idea of these senescent endothelial cells was so interesting! They are wounded, they’re spitting out inflammatory cytokines, they can’t open the blood vessels very well anymore – and they’re staying put!
This is another interesting thing about this.
Replicative Endothelial Cell Senescence May Lead to Endothelial Dysfunction by Increasing the BH2/BH4 Ratio Induced by Oxidative Stress, Reducing BH4 Availability, and Decreasing the Expression of eNOS
Reducing BH4 availability would also lower dopamine and norepinephrine.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11432946/
What are possible treatments if these findings are viable?
I just updated that section.
“A wide variety of treatments are available should these findings be validated. Since some involve strong drugs, further studies would need to be done, and the authors specifically warned against using this study as a reason to initiate a treatment.
Since authors demonstrated in several ways how NETs may be involved, they probably present the most likely short-term treatment opportunity. Several treatments could inhibit the production of NETs (DNase enzymes, platelet–neutrophil interaction blockers (P-selectin inhibitors, PSGL‑1–targeting agents)) or eliminate NETs (colchicine, some statins, or PAD4 inhibitors).
Anticoagulants are probably the most contentious therapy, given the possibility of side effects, but they might be helpful with microclots in some cases.
One study found that L‑arginine plus vitamin C improved blood flows and fatigue in long COVID. Hyperbaric oxygen therapy (if done enough times) can be helpful for some people and may improve blood flows.”
Dr. Wick from Labor Wick has recently published a preprint of a study he did on clothing aggregates (doesn’t call them Microcloths anymore), they also tested blood thinners. I think their study group is too small and in the preprint important informations are missing for me to take it serious at this stage, but having taken blood thinners and thinking they help me. Maybe read it as a short side literature.
Also I’m also suggesting you sign up for the German conference, it’s free.
https://www.nature.com/articles/s41598-026-42952-8
Thanks for the link and I just registered for the conference 🙂
Excellent article – thank you, Cort!
P.S.
I love how all these AI platforms are using your blog to answer questions about MECFS almost all the time (showing your pages in the resource links). Hopefully this makes you feel extra awesome for all your hard work!
Interesting article. I’ve long believe blood vessels, particularly in the brain, are an important piece of the puzzle. I once had a tremendous effect from taking a combination of vasodilators (garlic and ginkgo) along with blood thinners like vitamin E and aspirin. That was twenty years ago, and unfortunately the effects were not sustainable.
Over the last few months I’ve been taking pulsed rounds of fibrin dissolving agents (serrapeptase, nattokinase, and lumbrokinase) with very promising results. This is a developing area of babesia treatment (which I’ve tested positive for by FISH). What some LLMD’s are suggesting is babesia is plugging up capilaries, particularly in the brain, so as to evade immune cells in the blood. My experience is compatible with this explanation. Proceeding slowly seems to be key, as being too aggressive can lead to crashing. I suspect sudden oxygenation and restoration of immunity to previously insufficiently perfused cells can lead to further cytokine release. I suspect pathogens like Lyme and whatever else have been enjoying a rather cozy existence on the other side of those clogged capillaries.
I think David Putrino will touch on the nattokinase trial in the conference.
What symptoms do you find are helped?
Clean up of senescent endothelial cells would/should be taken care of by efferocytosis. Is efferocytosis inefficiency seen in people with long covid or ME/CFS?
https://pmc.ncbi.nlm.nih.gov/articles/PMC8913510/
Efferocytosis is the effective clearance of apoptotic cells by professional and non-professional phagocytes. The process is mechanically different from other forms of phagocytosis and involves the localization, binding, internalization, and degradation of apoptotic cells. Defective efferocytosis has been demonstrated to associate with the pathogenesis of various inflammatory disorders.
Yes w/r/t SARS-CoV-2
https://pmc.ncbi.nlm.nih.gov/articles/PMC9262386/
COVID-19 is a disease of dysfunctional immune responses, but the mechanisms triggering immunopathogenesis are not established. The functional plasticity of macrophages allows this cell type to promote pathogen elimination and inflammation or suppress inflammation and promote tissue remodeling and injury repair. During an infection, the clearance of dead and dying cells, a process named efferocytosis, can modulate the interplay between these contrasting functions. Here, we show that engulfment of SARS-CoV-2-infected apoptotic cells exacerbates inflammatory cytokine production, inhibits the expression of efferocytic receptors, and impairs continual efferocytosis by macrophages.
For ne, I can walk upstairs most times instead of having to crawl or not attempt at all.
It also staves off many of the frightening cardiac symptoms I get.
I feel more oxygenated. For me its not a cure obviously abd I fear the classic m.e. return to illness state that seems to happen after a few months
I’ve seen recent improvements in my health that I don’t attribute to fibrinolytic enzymes. But who knows for sure how much of one’s symptoms are strictly attributable to a particular therapy rather than something else one is doing for their health. That said the effects I do attribute to the fibrinolytic enzymes are a markedly improved dream recall, as well as feeling worse for a day or so followed by feeling quite a bit better in the days that follow that. Such is life with detoxifying and beating back pathogens.
It’s apparent that the babesia feels the need to rally as I’m dissolving fibrin. I also tend to sensitize to foods for the day that I’m down. It’s something I’m having to take slowly. Serrapeptase is gentler than lumbrokinase so it’s the one I’m using for now at about .25 – .5 of a capsule once or twice a week.
Im taking nattokinase . Better blood flow.
Even a return to what occurs to healthy gentlemen in the morning on occasion!
I think the vascular system is a big part of the disease.
The problem is, if endothelium has been damaged, its literally aging faster and at a dysfunctional way that means ( permanent? ) damage has occurs.
I hope that’s not the case
Covid has never shown to exist.
I don’t know how this appeared on my laptop yesterday, but it is a world map to ME/CFS doctors and labs.
https://mecfsroadmap.altervista.org/mecfs-doctors.html#:~:text=The%20Gottfries%20Clinic%20uses%20vitamin,bacterial%20dysbiosis%20in%20the%20kidneys.