


Geoff’s Narration
The GIST
Collagen is a major ingredient of the extracellular matrix
A recent study identified a subset of long COVID patients with markers of endothelial damage and vascular dysfunction. The blood vessel issue may, however, be tied to a larger issue – problems with the connective tissues or, more accurately, with the extracellular matrix (ECM), which makes up the connective tissues.
The extracellular matrix (ECM) – made up of collagen and other factors – provides the scaffolding and structural support for our tissues; i.e., it helps to keep the blood vessels, nerves, ligaments, bones, etc. in the right place.
 Health Rising’s Quickie Summer Donation Drive is On!
Health Rising’s Quickie Summer Donation Drive is On!Mast cells don’t just affect the ECM; they partner with it. The ECM stimulates mast cells, which in turn secrete substances that remodel it, stimulating further mast cell production. Depending on how mast cells react, they can either degrade or bulk up the ECM (fibrosis).
Note that either a degradation or buildup of the ECM can cause problems, and some of the problems are similar. If the ECM is so degraded that it can’t keep the tissues in place, we would expect to see misalignments, subluxations, nerves getting impacted, problems with blood flows, etc.
The same is true if the ECM turns fibrotic and starts laying down too much collagen, etc. We would expect to see things like compressed small blood vessels, poor blood flows, and tissues that have been moved out of place.
While the blood vessels are not technically termed connective tissues, each of the three layers that make up the blood vessels contain either extracellular matrix or straight out “connective tissues”, and that includes the “basement membranes”.
One has to wonder if Drs. Ruhoy and Kaufman have been way ahead of the curve regarding the connective tissues.
THE GIST
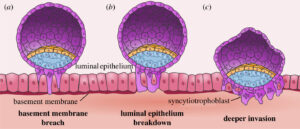
The basement membranes are found across the body. In this image of the epithelial lining of the uterus, they (the red line) anchor the epithelial cells.
- We’ve been looking at blood vessel issues recently. They may, however, be tied to a larger issue – problems with the connective tissues or, more accurately, with the extracellular matrix (ECM), which makes up the connective tissues.
- The extracellular matrix (ECM) provides scaffolding and structural support for our tissues; i.e., it helps keep blood vessels, nerves, ligaments, bones, etc., in the right place.
- Mast cells – which have become a big deal in ME/CFS – are intimately connected to the extracellular matrix. Depending on how mast cells react, they can either degrade or bulk it up.
- Either way, the extracellular matrix may not be able to keep the tissues in the right place, causing misalignments, subluxations, nerves getting impacted, problems with blood flows, etc.
- The problems with the endothelial cells lining the blood vessels that we’ve seen so far could negatively affect the basement membranes and blood flows. These are thin, specialized sheets of collagen, etc. (e.g., our ongoing theme -extracellular matrix – connective tissues) found under skin (epithelial) and blood vessel (endothelial) cells.
- These basement membranes anchor the endothelial and epithelial cells. Recent German studies found thickened basement membranes surrounding the capillaries in ME/CFS patients. These thickened basement membranes make it more difficult for capillaries to reach the muscle cells.
- Both the basement membrane problems could result from inflammation in the blood vessels. When this happens, the endothelial cells lining the blood vessels produce an immune factor called TGF-B (remember the mast cells), which can cause thickening or remodeling of the basement membranes, stiffen the blood vessels, and support the formation of microclots.
- Thicker basement membranes in brain blood vessels could also prevent glymphatic fluid from clearing toxins, leading to brain fog and other problems.
- Korean researchers have built a mouse model of ME/CFS, which they believe shows that increased TGF-B in the brain is causing “central fatigue”; i.e., brain-induced fatigue. In their model, TGF-B levels were increased in areas of the brain that have been impacted in ME/CFS.
- TGF-B has been a bit of a mystery in ME/CFS for quite some time. One of the more consistently elevated cytokines, TGF-β, can be pro-inflammatory or anti-inflammatory depending on the context it is found in. ‘
- The Amatica group, though, may have cracked the TGF-B code. Amatica found increased levels of TGF-B and two other factors – each of which could be associated with low blood flows.
- These factors could also impact the kidney cells – which a recent Open Medicine Foundation study suggested could be damaged in ME/CFS.
- The main treatment possibility would seem to be TGF-B inhibitors. These are strong drugs that could produce negative side effects if given to the wrong patient. If the TGF-B findings are validated and found to be associated with blood vessel or other issues in ME/CFS, they provide the possibility, though, of a small, closely watched trial
- Another approach would simply be to find ways to reduce the inflammation in the blood vessels. In that vein, endothelial cell protectors, anticoagulants, and mitochondrial enhancers such as rapamycin might help.
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit
Down to the Basement (Membranes)
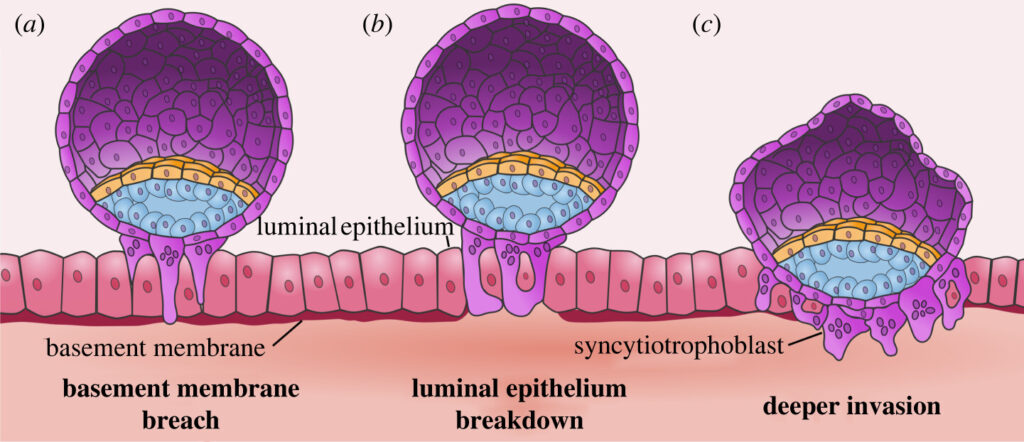
In this image of the epithelial lining of the uterus, the basement membranes (the red line) anchor the epithelial cells. (This image shows how the basement membrane breaks down so that a fertilized egg can burrow into the uterine lining.)
Suddenly, the basement membranes have become a thing. The thing is, they are all over the place. If you’re looking for a way to explain the multisystemic aspect of ME/CFS and long COVID, the basement membranes are one way. They’re found in the blood vessels, muscle tissues, skin, peripheral nerves, and kidneys…
The term “basement membrane” is quite descriptive. These thin, specialized sheets of collagen, etc. (e.g., our ongoing theme -connective tissues) are found under skin (epithelial) and blood vessel (endothelial) cells. (They also surround muscle cells, fat cells, etc.)
The possibly senescent endothelial cells in long COVID and ME/CFS come with a price. Nunes and Pretorius noted that “senescent endothelial cells exhibit phenotypic changes and increased adhesive properties to the basement membrane”
Found just below the endothelial cells, the basement membranes attach to those cells and anchor them in position. They basically keep them from floating away.
Because senescent endothelial cells tend to become more firmly attached to the basement membranes, they can become more rigid and less able to “go with the flow” of blood, so to speak, in the blood vessels. A too-firm attachment to the basement membranes, then, is another way blood flow may be interrupted in long COVID and ME/CFS.
That may be just the beginning. Two German research groups have found increased capillary basement membrane thickening in the muscles of ME/CFS patients. Because the capillaries have to make their way through thickened basement membranes to get to the muscle cells, these thickened basement membranes could be impairing blood flows as well.
A Thought Experiment
So now suddenly we have two potential basement membrane problems involving the blood vessels: the endothelial cells may be too firmly attached to them, and increased basement membrane thickening in the capillaries may be impeding blood flows. Could these two basement membrane issues be connected?
It’s possible. As the last blog noted, the inflammatory state endothelial cells are exposed to during an infection could push them into senescence and cause them to exhibit a senescence-associated secretory phenotype (SASP).
In that state, they may produce high levels of a cytokine called TGF-B (remember the mast cells), which can produce a thickening or remodeling of the basement membranes, and, to boot, stiffen the blood vessels, and support the formation of microclots.
That could create a vicious circle: senescent endothelial cells emit TGF-B, which thickens the basement membranes and impairs blood vessel functioning, thus pushing them further into senescence, which causes them to produce more TGF-B, and on and on.
As bad as a vicious circle sounds, it’s exactly what we want to uncover. We want to find self-reinforcing, locked-in states that produce a chronic illness.
Toxic Brains as Well?
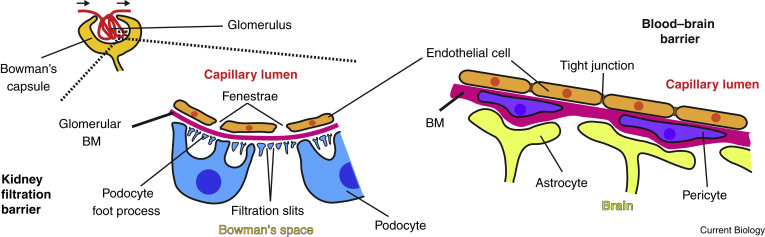
Basement membranes in the kidney and brain (the red line below the endothelial cells). (Image from Current Biology, March 20th, 2017, Jayadev, R and Sherwood, Wikimedia Commons)
Tate proposed, in 2022, that neurovascular pathways or a dysfunctional blood-brain barrier (BBB) (which could be created by endothelial problems) resulted in chronic neuroinflammation and led to a sustained illness in ME/CFS.
That’s bad enough, but the small blood vessels in the brain are surrounded by fluid-filled channels (perivascular spaces) through which glymphatic fluid cleanses our brains of toxins. Thicker basement membranes in the blood vessels could be squeezing and stiffening, reducing the perivascular spaces’ ability to clear toxins and leading to brain fog and a host of other problems.
Korean researchers have been exploring a TGF-β / brain connection in ME/CFS since 2020. They’ve created a fascinating mouse model of ME/CFS, which suggests that elevated TGF-β levels in the brain are producing “central fatigue”; i.e., brain-induced fatigue. The ME/CFS mouse model had increased levels of TGF-β in serum and in brain areas (prefrontal cortex, hippocampus, hypothalamus, and raphe nuclei in the brainstem), all of which are affected in ME/CFS.
Plus, injecting TGF-β into the brains of mice resulted in decreased activity, decreased dopamine levels, and increased markers of muscle fatigue (lactate dehydrogenase (LDH) and creatine kinase (CK)). (Interesting that an alteration in the brain produces markers of fatigue in the muscles (!). Reduced levels of dopamine, of course, have been associated with fatigue before, and several studies have highlighted the basal ganglia – the primary producers of dopamine in the brain – in ME/CFS. They wrote that their results
“suggest that TGF-β1 plays a critical role in the development of central fatigue and is, therefore, a potential therapeutic target of the disease.”
Time will tell, but future studies could determine whether increased levels of TGF-β are associated with markers of basement membrane thickening, endothelial senescence, and reduced oxygen uptake in tissues and the brain.
We’re not done with TGF-β, yet, though.
Amatica Uncovers a Blood Vessel Subset in ME/CFS?
Researchers have been wondering what the heck to do with TGF-β and ME/CFS for quite a while.
Several studies have found elevated TGF-β levels in ME/CFS, but given TGF-β’s ability to be pro- or anti-inflammatory depending on context, its role in ME/CFS has remained a mystery.

Has Amatica uncovered a TGF-B subset in ME/CFS? (image from National Cancer Institute, ID 2707)
Last year, Amatica may have solved the mystery. While no papers have been published, Amatica reported finding increased levels of TGF-β2 and two other factors (HIF1a, and PINK1) in 20-30% of ME/CFS patients.
This finding would seem to point an arrow straight at the blood vessels. Not only can TGF-β2 promote basement membrane thickening (by increasing the production of collagens, fibronectin, laminin, and proteoglycans), but it also inhibits the degradation of the membranes.
Increased HIFI levels, on the other hand, indicate that a low-oxygen (hypoxic) environment is present (as one would expect in a blood flow-challenged disease). HIFI also supports basement membrane thickening. Finally, PINK1 indicates that mitochondrial stress is present – exactly what one would expect if sufficient amounts of blood/oxygen are not getting through.
The increased 2TGF-β findings, then, could reflect a process that is reducing blood flows to the tissues. Moving outward, it’s also possible that this triad of factors could be impacting the kidney cells (podocytes), which a recent Open Medicine Foundation-funded study suggests, which could be a risk in ME/CFS. This is because this combination of factors could impact the cellular membranes in podocytes, in particular.
This hypothesis could be tested by stratifying ME/CFS/LC patients using Amatica’s markers (TGF-β2/HIF1a/PINK1) and determining whether capillary flows have been altered and whether markers of endothelial dysfunction or extracellular matrix disruption are present.
Again, we see a constellation of possibly interweaving themes.
Treatment Possibilities
Say a TGF-β2/HIF1a/PINK1 subset with reduced microvascular blood flows and endothelial damage is present – what then? The treatment would depend on whether fibrosis (those enlarged basement membranes) or
TGF-β-inhibitors – there are a bunch of them – might be a possible candidate at some point. They’re pretty heavy-duty drugs used mostly for short periods in cancer and fibrotic diseases, and have never been tried in a disease like ME/CFS or long COVID. TGF-β plays a complex role in the body, and administering the drug to the wrong patients could cause serious problems, including an increase in autoimmunity.
A small, short TGF-β inhibitor ME/CFS/long COVID trial might be able to be done, though, in patients with clear evidence of TGF-β elevation and no evidence of autoimmunity. The trial could determine if TGF-β inhibitors improved microvascular flows, mitochondrial activity, and fatigue.
Another approach is to target the things that increase TGF‑β levels, such as oxidative stress, microvascular injury, and viral persistence. ACEi/ARBs and statins to protect the endothelial cells, anticoagulants to break down clots, and rapamycin to support the mitochondria.
A small Korean pilot study using Myelophil (MYP), a formulation of two herbs, Astragali radix and Salviae radix, (500 mg per capsule) twice daily for 4 weeks, did show significant improvements in fatigue, brain fog, etc., and may have modestly reduced TGF-B levels in some patients. However, because no placebo controls were included, a larger study is needed to provide results we can trust.
Conclusion
Something is clearly going on with the blood. Isn’t it time for a nice, big grant package to explore that?
Something is going on with the blood. The invasive cardiopulmonary exercise testing done by Systrom and others clearly shows that normal amounts of oxygen are not being extracted by the muscles. Since oxygen extraction is largely a function of oxygen delivery to the muscles via the small blood vessels, these vessels are prime candidates.
Indeed, a just-published long COVID study employing a 2-day exercise test (!) and near-infrared spectroscopy to assess oxygen delivery to the calf muscles found that the oxygen is not getting through. The big question is how it’s getting stopped and what effect it’s having.
The ME/CFS Research Foundation Conference (July 4-5)
The good news is that this subject is getting more and more interest. The upcoming free two-day German conference from the ME/CFS Research Foundation features three presentations on the blood vessels/blood flows in ME/CFS. As usual, the Germans are leading the way.
- Perfusion Across Scales in ME/CFS: From Capillary Density to Cerebral Blood Flow
- Biomarkers and Mechanisms Associated with Endothelial Dysfunction and Hypoperfusion in Post-infectious ME/CFS
- Signals in the Flow: Vascular Biomarkers and Neurovascular Dysfunction in ME/CFS
Besides these, this two-day conference is chock-full of intriguing presentations on autoimmunity, tryptophan, ATP. My two favorites: are “Whole Body PET Imaging” from Michelle James at Stanford, and “Lipidome and Metabolome Metabolism” from the Open Medicine Foundation’s Chris Armstrong. (Anything lipids excites me now…who knew?). Sign up for the free conference here.
Isn’t it time for a nice, big RO1 grant package from the NIH focusing on the blood vessels and blood flows?
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit


Wow Cort, great work. The connection between endothelial dysfunction, microcirculation, and now ECM/tissue remodeling really resonates with me as an applicable theory for the delayed PEM I experience.
Hi Cort, a fantastic blog. Circulation problems and oxygen uptake is the core problem. Then I think that the fight-or-flight response and the autonomic overdrive response are the body’s attempt to keep circulation and oxygen uptake going on. So then there is nothing wrong with the brainstem itself. Although this system works both ways -:)
Been saying this forever!!! So glad its getting recognised.
Whilst nattokinase etc is going to help.
We need crispr abd stem cells to reoair/ change the structure of the collagen
I’m curious whether there’s a distinction between this phenomenon and hEDS or whether most people with hEDS have this subset of ME or, conversely, most people with this subset of ME have hEDS. Either way, the research and treatment possibilities are exciting!
I have no idea but those are great questions! :)….Hopefully, researchers will track down the ECM/connective tissue subsets. This could show up in so many places from the spine to the gut to the blood/brain barrier to the muscles… It’s really intriguing :). Time will tell…
I thought Cort described connective tissue thickening while hEDS is more of a loose connective tissue issue. But maybe I did understood it wrong?
What did you mean Cort?
The blog did focus more on extracellular matrix thickening but degradation is possible as well. Either one can cause the tissues to be misplaced. Hypermobile EDS is more characterized by connective tissue degradation but, interestingly, some of the fascia appears to be thickened as well. It’s not stiffened though. It’s “soft and disorganized”.
The omf concluded that heds is present in whitney dafoe on a deep dive of his metablomics and concluded eds was a precipitating factor in the development of cfs i believe
Thanks, Cort. I would like to point out that TGF-β (Transforming Growth Factor-β1) is a regulatory cytokine highly concentrated in platelet α-granules and plays an important role in immune-mediated thrombocytopenia (ITP) by maintaining immune tolerance. Low TGF-β levels are associated with lower platelet counts and chronic ITP, whereas increasing TGF-β may help restore immune homeostasis, raise platelet counts, and suppress the autoimmune response.
In this study, I see a possible connection. Participants receiving mezagitamab and placebo had similar overall rates of side effects, with only slightly higher rates of serious adverse events in the mezagitamab group, while baseline platelet counts were comparable between groups. Importantly, by week 16, the 600-mg mezagitamab dose produced a substantially stronger platelet response, with 91% of participants responding compared with 23% in the placebo group. This raises the possibility that improved platelet recovery could also influence immune regulation through increased platelet-derived TGF-β activity.
A Phase 2 Randomized Trial of Mezagitamab in Primary Immune Thrombocytopenia
https://www.nejm.org/doi/10.1056/NEJMoa2513120
I agree that it is likely not as simple as saying there is too much TGF-β in ME/CFS, even in a subgroup of patients. When taking a quick look at Wikipedia I see:
“TGF-β induces apoptosis, a form of programmed cell death, in human lymphocytes and hepatocytes. The importance of this function is clear in TGF-β deficient mice which experience hyperproliferation and unregulated autoimmunity.”
To me that says that increased TGF-β has high chances to be very much a needed tool in many ME/CFS cases. Each time our immune system gets triggered, immune cells are activated. Part of that activation is the start of producing large amounts of new immune cells to amplify the immune response.
If those new cells are left unchecked, they raise the strength of the immune response for many hours to days. That’s great when there is an actual need to do so, but only when it is definately needed to be able to fight pathogens. When it’s not needed, it’ll just produce inflammation and put the immune in a very trigger happy state.
When looking at the brain, with every exhaustion due to exertion there IMO is a good chance microglia are activated and start to divide and grow in numbers. Daily signals to increase their numbers without any sufficient counterbalance is not something we wish nor desire. And TGF-β has *potential* to counterbalance that.
See https://www.mdpi.com/2227-9059/12/11/2468 saying “GF-β signaling is pivotal in maintaining microglia in a homeostatic state under normal conditions. This cytokine not only preserves microglial identity but also modulates its responsiveness to environmental changes, balancing their roles in neuroprotection and immune activation. In pathological conditions, TGF-β can regulate microglial reactivity, potentially exacerbating or mitigating CNS damage depending on the context.”
=> So it is IMO not about saying more or less is needed. It plays a fundamental and needed role in CNS immune regulation, but above all likely points to *other* / additional signals very frequently initiating microglial activation. Those signals IMO likely coincide with what initiates / triggers PEM (things like over-exertion). So long as one does not succeed in controling PEM rather well, fidling with TGF-β may be rather tricky.
Platelets also play a role in pathogen ‘capture’ e.g. they can immobilize some pathogens and render them less harmfull.
See https://www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2025.1616783/full, title “Platelets in infection: intrinsic roles and functional outcomes” saying:
“These intrinsic platelet attributes enable dynamic interactions with pathogens and immune cells, significantly contributing to pathogen capture, neutralization, and the orchestration of innate and adaptive immune responses.”
So more (at least not depleted amounts of) healthy platelets sort of signal the immune system that the blood ‘pathogen capturing’ mechanism is able to reduce the pathogenic load. That in turn offers room for less ‘immune expansion’ e.g. downregulating things like increased microglial activation and increases in microglial expansion.
From that point of view, “improved platelet recovery could also influence immune regulation through increased platelet-derived TGF-β activity” makes sense.
Hi Cort;
Since microglia are not “resting” cells, but highly active and specialized immune cells of the central nervous system (CNS), they continuously survey the brain parenchyma, regulate neuronal circuits, maintain tissue homeostasis, and detect injury or disease processes such as Alzheimer’s amyloid-β plaque formation. This has been well established for years, including studies published around 2020 https://pubmed.ncbi.nlm.nih.gov/31518022/
In addition, findings involving platelet-derived growth factor (PDGF) signaling in cultured brain slices showed that loss of NG2 glia abolished the homeostatic microglia signature without affecting disease-associated microglia profiles. These observations further support the idea that CNS immune regulation depends on active glial cross-talk and continuous surveillance mechanisms rather than passive or “resting” immune states.
That is why I question why the CNS is still often treated as relatively “immune-privileged” or neglected in some disease models, despite the fact that microglia constantly monitor brain tissue and respond dynamically to pathological changes — even in situations where there is no obvious apoptosis.
In addition:
What I’m missing and advocating for years is more detailed attention given to the processes of the glymphatic and lymphatic systems.
My question was and still is: What if apoptosis—programmed cell death—fails to function properly or if the lymphatic drainage (sanitation) system becomes impaired or blocked, while the body’s defense mechanisms are also compromised? In that case, potential threats such as bacteria and toxins may not be effectively transported to the lymph nodes to activate T and B cells. Instead, lymphatic fluid (chyle) may carry toxins and infected tissue components back into the bloodstream, potentially spreading harmful substances throughout the circulation.
The same principle may also apply to the glymphatic system—the brain’s waste-clearance network. If glymphatic drainage is impaired, toxins and inflammatory byproducts may be continuously recycled rather than efficiently removed. This ongoing recycling can repeatedly activate T and B cells, as well as cytokine signaling, potentially keeping the brain, tissues, muscles, organs, and the body as a whole in a prolonged state of inflammation and toxicity, which may ultimately contribute to cellular damage and cell death.
Mentioned back on January 25, 2024
Lymph nodes filter system for viruses, bacteria and fungus invasion
https://swaresearch.blogspot.com/2024/01/the-only-filter-system-we-have-is-lymph.html
and several times on PR.
Wow! This is exactly the resultat my musclebiopsie has shown. Next step for me is to look weather this TGF ß ist elevated. What else could one do if one know this was ones pathomechanism?!
Thanks Cort. When I first got mold illness in 2013 I thought “ooops, blood not flowing well, what do we do?”. After detox and doing VIP and tadalafil etc the blood flowed better. Out of the wheelchair and eventually back to mtn bike racing!
Unfortunately with my long covid the “old tricks” aren’t working as well. Started Arterosil HP recently in hopes of fixing the endothelium some. Maybe pentoxifiline could help too. Etc. Keep us up to date on the latest findings.
Hi CG,
Re ur words of:
wheelchair to mountain bike racing”.
That is amazing….how can I find out more about your protocol of detox and TADALAFIL and VIP?
Thanks
It was a complex and highly individualized approach that my mold/etc specialist Mary Ackerley, MD helped me with. We just basically left no stone unturned in my quest for health for many years. I recovered a lot and helped build the nonprofit ISEAI.org so that others wouldn’t have to go through what I did. And was good for years, then unfortunately got absolutely hammered by covid vaccines more recently and now am disabled again. Fighting in “round 2”. So reading this latest article by Cort is very helpful for all of us suffering from terrible blood flow and PEM etc. A few years ago at age 49 I could run a 6:35 mile. Now I can barely hobble to the restroom.
Also wanted to mention my experience with TGFβ1 blood testing. This is a marker commonly looked at in mold-related illness and CIRS. Unfortunately the lab probably needs to be trained in very specific methods in order for the marker to be accurate, at least from what I learned. Dr Ackerley actually trained the labcorp near her and sent all her patients to that one location. Even then, the marker “bounced around” for me and didn’t really seem to correlate with how functional I had become over years of treatment. So although Medicare covered the marker for me I stopped relying on it. Just a word to the wise in case you all try to get it done. Dr Shoemaker has mentioned the specific ways this blood test needs to be run/handled. Maybe things have changed over the years and it is more reliable these days? I don’t know. I think the reference ranges may have changed. And back in the day it was advised only to run it at labcorp and not quest, I think, for some reason. Anyhow….
And I will visit ISEAI.org
Cg- thank u for your detailed and articulate reply. May I ask where u live. Thank u
CG, I was also a patient of Dr. Mary Ackerley for several years after 3 years of being very sick not knowing my husband and I were living in a mold house. After losing everything in our home and 2 cars (mold in the garage), we built a new home and I recovered with Ackerly testing and supplements. Then got Covid and sick again. I feel your pain.
I am sorry! It is quite rough to be taken out badly multiple times…
This is so far over my head that I can’t even ask a good question, but can this somehow be related to MASTOCYTOSIS?
From https://pmc.ncbi.nlm.nih.gov/articles/PMC8948255/
“Utilising this workflow, we identified and validated CXCL7, LBP, TGFβ1 and PDGF receptor-β as novel biomarkers for systemic mastocytosis. We demonstrate that CXCL7 correlates with neutrophil count offering a new insight into the increased prevalence of anaphylaxis in mastocytosis patients.”
Translation: in mastocytosis, TGFβ1 is also increased. Note this is a correlation, not necessairly a cause! Mastocytosis is characterised by too much (and abnormal functionning) mast cells and increased TGFβ1 is a mechanism to (try and) regulate these back to normal numbers.
The paper also says: “TGFβ Reticulin fibrosis is frequently associated with SM and studies have demonstrated a correlation between the circulating levels of TGFβ1 and the extent of bone marrow fibrosis36,37.”
So both too few and too much TGFβ is problematic. A optimal balance is desired.
To dejurgen,
I’ve seen your name for many years on this site in the comment section and I was always curious. May I ask your background/degree? You are always so knowledgeable about science ,etc.
… and I assume you are afflicted with our condition or have a family member that is? Thank u
I am an engineer with research experience (PhD). I have no medical education.
I got into ME/CFS science when I kept declining by the week and estimated I would reach ‘a point of no return’ in about half a year. I gave myself 5% chance to be able to halt and reverse the decline before I had no longer any ability to even attempt to fight back.
So I got in due to a mix of necessity, desparation and determination. I improved a lot since and escaped the hellhole, but I still have a very long way to go. ME/CFS + FM and many commorbidities.
I salute your determination. We live challenging lives, huh.
Thank you for sharing ur background/expertise.
Take care
Thank you.
Agree re formulating a question
This note was in response to Elizabeth
Conference was last week.
Maybe the odd American date system threw you off
It has become quite popular recently to imply “subsets”, they are to be found on every corner of the discussion. And here we go again in respect to Amatic´s findings. I do not think that it is valid to claim subsets on the basis of cross sectional data in a disease which is marked by two different disease states: PEM and non-PEM. What if TGF-β2 levels may be upregulated during PEM? Then the 20 or 30% of samples with elevated TGF-b2 levels may just be those in which the samples were drawn during PEM. I do not claim that this is the correct interpretation, but it is a plausible one as TGF-b2 acts as a signaling molecule that helps regulate metabolism, so different levels during PEM could at least be thinkable.
In short: we should think twice before we claim “subsets” – because their construction may just be based on a misinterpretation of data.
Just curious, are you inputting this to Nationale Dekade Steuerungskreis via Ärztlicher Beirat DGMECFS?
And, as I’ve said before, I believe in a 3rd state too that might interfere with results: Pushing state/adrenaline-fueled/overactivated state. The pushing part of ME/CFS push-crash cycles.
Could be relevant re. the old topic of “The measurement distorts the result”?, because many patients will be in a high-adrenaline state when visiting a clinic (due to travels and excitement).
Just experienced it again some weeks ago: was *exceptionally* functional on adrenaline for 2 weeks while managing a high stress situation, crashed super hard, not recovered yet. (Probably burnt out my stress system and cellular resources too during that time: In a completely different state now where my usual supplements and medications do not work.)
In my opinion, any ME/CFS pathomechanism/PEM theory must be able to explain how and why mental pushing or adrenaline (the “second wind” when having pushed past an exertion limit previously signalled by the body) can temporarily override ME/CFS muscular function limits but cause hard PEM later. I think Klaus Wirth’s theory would probably pass the test.
I am making comments as much as i can – if they are all heard, who knows, but this is all i can do (including on X).
The “third” stage arguments is very important, thank you. Yes, many patient show up for their research appointments with their systems revved up, not in a crash, not on their normal state but in a tenuous pre-crash state.
Thank you for the input!
Many patients can drive on a wave of adrenaline indeed. I can too, but it always comes at a cost.
Adrenaline has two sides. It mobilizes energy and blood flow to the brain and skeletal muscle, but at the cost of energy to the digestive tract. It also increases breathing capacity by being a bronchodilator.
The opposing side of adrenaline is that it is, not unlike cortisol, it weakens immune response strength. Both are stress hormones that increase energy production in vital organs and decrease immune strength. Less immune activation means less ROS and less chance to overactivate the microglia.
There IMO is another part to this: an increase in dopamine during that ‘high’ state. Dopamine weakens how the brain experiences fatigue. So on dopamine you can deplete yourself deeper before you feel depleted. When dopamine dips to below normal levels the reverse happens: you are more depleted / should feel more pain and exhaustion and with less dopamine your brain makes the experience twice as intense.
Dopamine also has another side: dopamine weakens / kills cells. It does so extra strong on immune cells. That IMO means that microglial cells expand less (in numbers) due to immune (and exhaustion) triggers and that they likely are less strong activated due to them too. After the ‘high’, cells are in a weaker state due to the ‘mildly killing capability’ against tissue / other cells then immune cells, due to the increased amounts of toxic waste products of dopamine and due to less dopamine moderating immune reactivity.
”Many patients can drive on a wave of adrenaline indeed. I can too, but it always comes at a cost.”
Absolutely true. Let’s keep it simple. Where does this adrenaline rush come from? Why this reaction? The body is apparently in a state of emergency. Is this stress response a compensation or the cause? This remains, for me, the 1 million dollar question….
I think there is an oxygen deficiency, hence such a strong reaction.
My best guess? The body downregulates (maximum and resting) ATP production potential body wise (for good reasons). That results in many situations where ATP production is inadequate (exertion in ME/CFS, standing up with reduced bloodflow to the brain in POTS…) to maintain basic functionality and safety (brain clarity when doing activity with risk of injury, falling and injury in POTS…).
Then emergency energy is needed quickly. And temporarily giving a boost in adrenaline is one of the quickest mechanisms to do so and do it while prioritizing only the most essential organs.
Was curious if this is related to fascia: 8 yrs ago, there was an interesting documentation on emerging fascia research. It can be watched with English subtitles here: https://www.youtube.com/watch?v=-f_Z6qxbhDo&list=PL692-lK7tWDUVxXzp-7ulTnyiHkoEvCV5&index=1 Here’s what Google KI says (in short, yes):
“The extracellular matrix (ECM) and fascia are not the same thing, but they are closely related. Fascia is the tissue itself, while the ECM is the structural network of proteins and fluid inside that tissue. Think of fascia as the “wrapper” (tissue) and the ECM as the filling and structural fibers (gluey substance) within that wrapper.
– Fascia: The comprehensive connective tissue system that wraps, separates, and supports muscles, organs, and nerves throughout the body. It is the overall “organ”.
– ECM (Extracellular Matrix): The non-cellular component of the fascia (and all tissues) that provides structural support, hydration, and nutrition to the cells. It is often described as a gooey, hydrated mesh of collagen and ground substance.
– Fascia includes the ECM plus cells (such as fibroblasts and myofibroblasts) that maintain the tissue.
– The ECM is the material outside the cells.
Analogy: If fascia is a fibrous net, the ECM is the gelatinous, nutrient-rich solution held within that net.