


Geoff’s Narration
The GIST
The 2026 PolyBio Spring Symposium – Pt I
One way to gauge the health of a field is by the number of conferences/symposia it supports. From the looks of things, the long–COVID and ME/CFS fields are moving up:
-
-
- The International ME/CFS conference – May 7-8
- Invest in ME 15th International Biomedical Research into ME Colloquium – May 27-29
- PolyBio Spring Symposium – May 29-30
- 14th Annual Dysautonomia International Conference – July 9-12
- ISLC-PAIS Conference – Aug 26-29
- 4th Canadian Symposium on Long COVID – Oct. 15–16, 2026
- 4th Long COVID International Conference in Nice, France – Nov. 12–13, 2026.
-
Usually, with conferences/symposiums, I hunt and peck and focus on a few presentations. The 6th PolyBio symposium, however, was so interesting and brought up so many issues that I ended up covering more than usual. It’ll be covered in two rather long blogs.
At this point, we have to ask: where, really, would we be without PolyBio? Founded by a person with ME/CFS (Amy Proal) and a researcher with a longstanding interest in ME/CFS (Michael VanElzakker), PolyBio has funded over 50 high-quality, innovative research projects over the past 6 years.

PolyBio received a grand total of $24,211 contributions in the year (2020) it was incorporated. Two years later, it received almost $18 million in contributions. Over time, it’s received about $50 million in private funding, including massive support from the Balvi Filantropic Fund established by Ethereum co-founder Vitalik Buterin.
Why has PolyBio grown so quickly from such humble beginnings? It’s provided a blend of rigor, creativity and urgency that’s found an audience. Focused entirely on pathophysiology, it’s an antidote to a rather stodgy, do-it-by-the-book RECOVER project. (On a plus note, note that RECOVER has funded over 60 outside investigator research studies. While they account for only about 3% of RECOVER’s budget, they will surely deliver significant results. A future blog will dig into RECOVER’s long-COVID (and ME/CFS – yes, there is at least one:)) grants.
THE GIST
-

PolyBio’s Long COVID Cure Initiative has the potential to be transformative for the field.
One very, very long blog turned into two just long blogs (the next one is coming up) as PolyBio’s 6th Symposium provided insight after insight into long COVID and a promising effort on ME/CFS.
- Amy Proal, co-founder of PolyBio, which has funded over 50 studies, noted that the arrows are increasingly pointing toward the tissues as being ground zero for long COVID.
- First, though, let’s take a look at what looks to be a transformative long-COVID project: PolyBio’s Long COVID Cure Initiative (LCCI).
- Funded by a cool $10 million donation from the Park-Pagliuci Foundation, the LCCI seeks to bring order to a chaotic treatment environment that promises long waits for effective treatment.
- The foundation of the LCCI is the $8 million VIPER project, which takes an organized, methodical approach to identifying biomarkers and patient subsets to which treatments can be targeted. The LCCI will also provide support for commercializing biomarkers, establish a treatment network, and educate doctors.
- PolyBio believes the LCCI will cut as many as 15 years off the search for long-COVID treatments.
- Several symposium presentations suggested that to really get at these diseases, we’re going to need to go deeper and deeper into the tissues.
- First came two gut studies. One study found that a gut-lining-sealing drug called larazotide prevented coronavirus proteins and other factors from entering the bloodstream and triggering an inflammatory response. Another used Bruce Patterson maraviroc-pravastatin drug combo to prevent monocytes from attacking the blood vessels in the gut. Both resulted in symptom improvements.
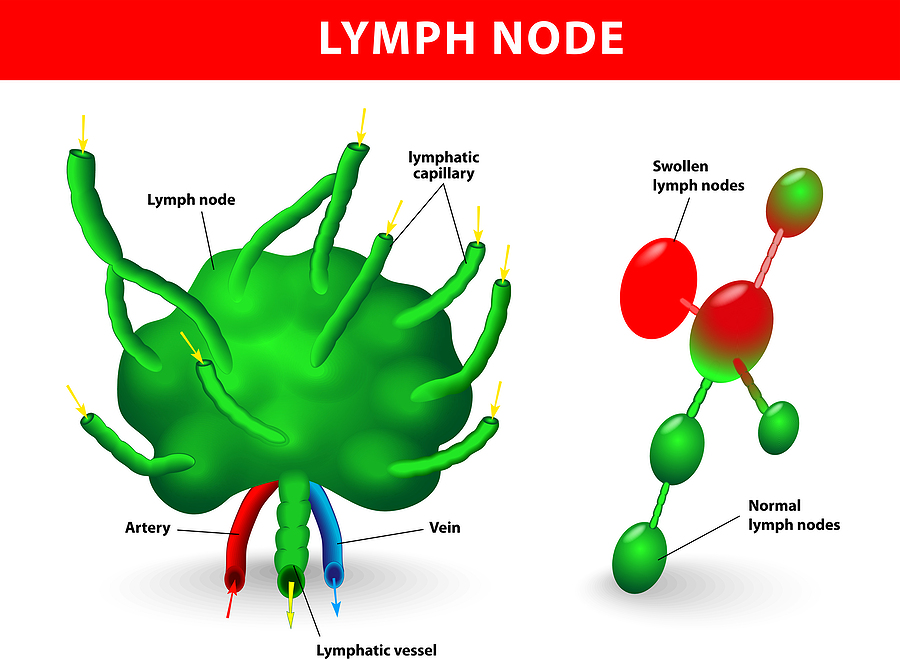
- Another study that examined B-cells in the lymph nodes and compared them with those in the blood found that the lymph node B-cells were damaged. This was important because it’s in the lymph nodes that B-cells encounter pathogens and devise responses to them. The study suggested that the coronavirus or another virus such as EBV (which actually hangs out in the B-cells) had penetrated the lymph nodes and was inhibiting the immune response needed to eliminate them. Once again, the problem appeared to reside in a tissue.
- Next came plaques in the arteries. A study found evidence that coronavirus RNA was present in some long-COVID patients’ plaques, and that the macrophages, the body’s main defense against them, were having trouble clearing the dead and dying cells from the plaques – producing more inflammation.
- The eyes are not just windows to the soul; they’re also windows to the central nervous system. A comprehensive retinal long-COVID study found evidence of neuroinflammation and an accumulation of amyloid proteins that have been associated with dementia.
- The dementia question is a complex one. Thus far, increased levels of misfolded or amyloid proteins have been found in the blood of long-COVID/ME/CFS patients, the eyes of long-COVID patients, and the cerebral spinal fluid of ME/CFS patients, and one study found that older, hospitalized patients had an increased risk of dementia. Much more study is needed.
- A small pilot Harvard study of long-COVID patients with craniocervical instability found impaired cerebrospinal fluid flow and altered CSF pulse-flows. The alterations were not particularly dramatic, but could be causing toxic metabolites to accumulate in the brain and lead to brain fog, fatigue, etc.
- Finally, a PET/MRI study found particularly high levels of inflammation at the point where the vagus nerve enters the brainstem.
- Since this region regulates sensory and gut-brain signaling, the autonomic nervous system, “sickness behavior” (whoa!), pain, and more, the potential for mischief in these diseases is high. Everything from fatigue, nausea, dysautonomia, sensory sensitivity, pain, sleep disruption, and “sickness behavior” could result.
- All in all, these presentations suggested that investigators need to explore the tissues more deeply, and, in particular, determine if pathogens persist in them and are driving these diseases.
Donation Drive Update

Health Rising is committed to keeping up the “big ideas” in these fields. If that supports you please support us
Thanks to everyone who’s brought Health Rising to about 2/3rds of its goal!
Keeping on top of major opportunities and themes in long COVID, ME/CFS, and fibromyalgia is a major goal, and in this part of the Symposium, two immediately stood out. One – a potentially transformative project – the Long COVID Cure Initiative has begun. Two. These diseases may have been “invisible” to the naked eye, but once you peer into the tissues themselves, lots of oroblems are showing up – in lots of places.
If keeping up with major findings supports you please support Health Rising. Thanks!
Health Rising is not a 501 c (3) non-profit
The Long COVID Cure Initiative (LCCI)
A transformative project begins.
PolyBio took its biggest step yet with the Long COVID Cure Initiative, launched in March of this year, courtesy of a $10 million donation from Todd Park and Steve Pagliuca, each of whom has family members affected by long COVID. The significance of this effort dwarfs any study finding.
If you want to make a difference, you look around, see what’s missing, and fill it. That’s what PolyBio did with The Long COVID Cure Initiative (LCCI).
The LCCI is designed to turn the long-COVID cure space from a bucking bronco that is going nowhere fast into a smooth, steady quarter horse that produces results efficiently and quickly. It’s not magic, and no, PolyBio hasn’t found a cure. It’s actually very simple; it’s what a good decent business would do as a matter of course. The problem is that the long-COVID field comprises hundreds of businesses, each operating in its own way.
Accelerating the timeline for treatments.
The LCC builds an infrastructure to accurately assess the effectiveness of a treatment. I hate to keep picking on the NIH’s RECOVER project, but I would have thought their first order of business would have been creating something like the LCCI. PolyBio believes the Long COVID Cure Initiative will cut 15 years off what would have otherwise been an interminable, chaotic search for effective treatments; i.e., it’s designed to play a transformative role in the long-COVID field.
It’s no surprise it’s missing. This is, after all, a new field. At some point, it was going to pull itself up by its bootstraps and get organized. For all the long-COVID field has produced – and it’s produced a lot – the treatment space is chaos exemplified. Six years later, there is still no standard diagnostic criteria, no telling who’s in what study, and no standardized procedures. The result is a field that can produce possible biomarkers but has a lot of trouble validating them. (Cue ME/CFS for the past 40 years.)
So PolyBio, steeped in the urgency that long COVID, with its lack of validated and effective treatments, has produced, stepped in. It partnered with a crack UCSF team that’s been honing its techniques in HIV for years. One of the leaders, Stephen Deeks, said the UCSF team (LIINC) is looking at the same pathways in long COVID that brought so much success with HIV.
The LCCI’s four-point plan.
-

Once the VIPER project hits its target, we WILL have a biomarker.
The Foundation – the VIPER (Validating and Investigating Promising Existing biomarkers) Project – it all starts with diagnostics; without diagnostic tests that identify the biological drivers behind the subsets we all know are there, we may be pretty much lost when it comes to clinical trials. (On that thought, it’ll be interesting to see if the big long-COVID clinical trials produce this. Hopefully, they are big enough to pluck out subsets.)
- The $8 million VIPER program – is the beating heart of the Long COVID Care Initiative. Built on the UCSF HIV biomarker program, it will test all possible biomarkers in an organized way. Its first project is a large, 150-person study in which everyone will undergo a gut biopsy, and many will also undergo an endoscopy. Just six months ago, the LCCI was a very good, very underfunded idea. Now, thanks to Park and Pagliuci, it’s the real deal
- Commercializing Diagnostics – The second step shows just how comprehensive PolyBio’s plan is. Apparently, many potential biomarkers die on the vine because commercializing them and getting them into labs requires a completely different skill set. PolyBio is bringing that skill set in to ensure that when good biomarker(s) are found, they can quickly make it through the regulatory process, withstand intellectual property challenges, and secure strategic partners who can fund the production of a commercial diagnostic test.
- Mobilize Smarter Clinical Trials – Once you have a biomarker, you have to use it to test drugs/treatments in “smart” clinical trials focused on the appropriate patient set. To facilitate that happening as quickly as possible, PolyBio is creating “a national, diagnostics-guided, clinical trials network purpose-built for Long COVID” (!). PolyBio will also, and this is potentially very important given the many generic drugs out there that drug companies no longer have an interest in, fund clinical trials of generic drugs. Generic drugs are probably the quickest and easiest way to get affordable treatments into long-COVID patients’ hands, but they are hardly ever tested.
- Train Doctors – Even with that, there are still hordes of busy, often overworked doctors, who will not be able to catch up with the long-COVID field. To that end, PolyBio and Mt. Sinai will embed clinical trial findings into core CME courses to ensure that doctors can quickly recognize and access promising treatments for their patients.
- Check out the entire plan here.
Looking at this initiative, I don’t think it’s any surprise that PolyBio was able to find two individuals to provide massive support for it.
Yet Another Big, Bold Project
So, we have another big, bold initiative popping up! We can put the LCCI next to the $10 million or so SequenceME, the OMF’s $2-3 million partially funded Bioquest Project, and several million-dollar, 1,000-person Amatica ME/CFS and long-COVID gene expression project, PrecisionLife’s mechanistic work, and Germany’s truly magnificent commitment to spend $500 million on post-infectious diseases over the next ten years.
An Aside – The Funders

Todd Park gave back.
We can thank PolyBio for providing the vision and Todd Park and Steve Pagliuca for funding it. It’s worth looking at the individuals whose support may make a difference for millions, if not hundreds of millions of people with long COVID. What a legacy to leave, and would that there were more of them.
Todd Park (net worth @$1.4 billion) graduated magna cum laude and Phi Beta Kappa from Harvard College. An entrepreneur, he co-founded Athenahealth, Castlight Health, and Devoted Health. He also helped launch Healthpoint Services, which is focused on delivering affordable clean water, medications, diagnostics, and telehealth to rural villages in India.
Park also serves on the boards of New America and The Public Health Company, both of which focus on public‑interest policy. Park, then, is well aware of the needs and has the know-how to build transformative infrastructures in the medical field. In short, he’s perfect for this initiative.

Steven Pagliuci gave back. (Image Wikimedia Commons Davos Forum 2016)
Steve Pagliuca (net worth @$4 billion) on the other hand, is a private equity investor, co-chairman of Bain Capital, and former co-owner of the Boston Celtics. He has a long history as a philanthropist via his involvement with the Celtics Shamrock Foundation (youth development), the Massachusetts Society for the Prevention of Cruelty to Children (MSPCC), and the Harvard Life Lab which supports medical entrepreneurship, and has strong ties to Duke University and Harvard.
With his deep biotech experience (via Bain Capital’s life‑science investments), and his own infrastructure‑building expertise, he, like Park, is a perfect match for this project. Both know a good thing when they see it – and PolyBio produced a very good thing.
Another Aside – A Good Gilded Age?
We are currently living in a new Gilded Age. In fact, recent reports indicate that a smaller tier of Americans own a greater share of America’s wealth (the top 1% own about 1/3rd of the U.S.’s wealth; the top 10% own about 70% of America’s wealth) than ever before. The concentration of wealth in the US far surpasses that of the “Gilded Age”.
The fact that much of this wealth is untaxed has, yes, disadvantages for the rest of us who have to foot the bills, but also contains immense opportunities. The upper tier has money to spend – sometimes lots of money – and how better to spend it than supporting medical research?
Historically, some wealthy individuals in the US, many of them ruthless competitors, have ended up making a significant difference. After rapaciously consolidating the oil industry (and ruining many of his competitors), John D. Rockefeller Jr. essentially spent the rest of his life and fortune building a remarkable college and university system across the US. At a time when racism was rampant in the US, and many blacks in the southern states still could not vote, Rockefeller provided large, systematic, and long-term support for southern Black colleges – most of which still exist.
Rockefeller also founded the first biomedical research institute in the United States (1901), which has since produced 26 Nobel Prize winners and 26 Lasker Award winners. Its focus on peer‑reviewed, project‑based, university‑centered grants became the blueprint for the NIH’s system.
Andrew Carnegie violently smashed protests and crushed unions, and imposed 12 hour workdays as he cornered steel mining, refining, and transportation. After he retired, though, Carnegie gave away 90% of his wealth and built 2,500 libraries and universities across the U.S. Carnegie’s early life was filled with poverty and hardship, and though he was the epitome of a hard-driving, callous businessman, by the end of his life, he was described as being “deeply contented and fulfilled”. European visitors were astounded to see the libraries in even medium-sized towns in the US, which surpassed those found in Europe.
The SpaceX, Anthropic, and OpenAI IPOs are projected to produce somewhere around 16,000 new millionaires, at least 20 billionaires, and 1 trillionaire. Let’s hope some of them give back as Park and Pagliuci have. These fields are ripe for progress. All they need is the funding.
Onto the Symposium
Into the Tissues We Go
Several symposium presentations suggested that to really get at these diseases, we’re going to need to go deeper and deeper into the tissues. This question has been discussed for decades in ME/CFS, but the field has never had the means to do so. Thanks in large part to PolyBio, long-COVID researchers are going to the tissues, and the findings are raising eyebrows. First, though, some microclot findings.
Into the Gut We Go
Take I: Gut Sealing Study
Stopping the leak by tightening up the gut lining junctions had positive effects.
Peter Moschovis of Harvard presented early results from an attempt to seal the gut lining in 107 patients using a drug called larazotide in a Phase 2a randomized, double-blinded trial. Larazotide is a synthetic peptide that prevents tight junctions in the gut from opening, thereby preventing the spilling of gut contents into the blood. The idea is that leaky gut linings are allowing the spike protein or the coronavirus to spill into the bloodstream.
An earlier study in children with multisystem inflammatory syndrome (caused by the coronavirus) found that larazotide helped clear the spike protein from the blood, reduce inflammation, and improve gut symptoms. An interim analysis suggested that the drug may improve sleep, fatigue, daily-life impact, GI symptoms, and cardiovascular symptoms. With data collection wrapping up, hopefully we’ll get the full results in the not-too-distant future.
Note that the problem is not necessarily that the spike protein is found in the gut lining, but that it’s escaping into the bloodstream, where it may be causing inflammation, autonomic instability, and even blood vessel damage. (Note that the Epstein-Barr Virus can also be found in the gut lining.)
Thankfully, larazotide appears to be well tolerated, only affects the gut, and produces mostly mild gut side-effects. Given these findings, one wonders why, given the finding that exercise exacerbates leaky gut in ME/CFS, increases symptoms, and produces post-exertional malaise, a drug like larazotide, which seals the gut lining, hasn’t been trialed in ME/CFS.
Gut Healing Take II
Speaking of the gut, Dominque Salmon reported that not only did a small pilot trial of maraviroc plus pravastatin reduce severe GI symptoms (stomach cramps, diarrhea, and bloating) by at least 30% in 13 of 19 long-COVID patients but that it also shrank their microclots. When the treatment was paused, their symptoms returned, and when it was resumed, symptom reduction recurred. Spike protein levels declined in 5 of the 7 patients who had the spike protein. Whole blood serotonin levels also increased.
Dr. Bruce Patterson pioneered the maraviroc-pravastatin approach in long COVID about five years ago, but he was focused on the blood vessels.. Patterson was targeting monocytes that he believed were attaching to the endothelial lining of the blood vessels. Patterson’s early theses: that classical monocytes are activated, that the endothelial lining is under attack, that platelet activation is happening, and that microclots are present, have all been validated by subsequent research groups. Patterson used these drugs to prevent monocytes from attacking blood vessels and to stabilize endothelial cells.
This group targeted the gut, but because the blood vessels are so abundant, the basic idea is the same. The idea is that monocytes in the gut produce inflammatory factors that increase gas levels and sensitize the nerves, causing cramping, bloating, and reduced gut motility. The maraviroc/pravastatin combo may prevent monocytes from attaching to blood vessels, reducing inflammation, increasing blood flow, improving oxygen levels, and supporting blood vessel health.
Salmon’s was a small study, but a multicenter randomized trial is in the planning /fundraising stages. HealthBio – another company formed by Patterson – began a 252-person maraviroc/atorvastatin long-COVID trial in September of last year. Its completion date was April 2026.
Into the Lymph Tissues We Go
In long COVID, B cells in the lymph nodes appear to be producing faulty antibody responses against SARS-CoV-2 — a defect that is invisible in routine blood tests but may explain why the virus is not fully cleared.
In “Adaptive Immune Responses to Long COVID Lymphoid Tissue“, Michela Locci went straight to the lymph nodes to examine how the B-cells found there are doing. She used an ultrasound‑guided fine needle aspirates (FNA) – developed apparently by her – to draw them out.
B-cells were taken directly from the lymph nodes and examined.
Why examine B-cells in lymph tissue instead of blood? Because the lymph nodes (and spleen and MALT) are essentially B‑cell factories and training grounds. These sites are where the B‑cells encounter a pathogen, activate themselves, and produce enormous numbers of clones to hunt the pathogen down.
Locci found a strange thing: the B-cells in the lymph nodes of long-COVID patients reacted very differently to the SARS-CoV-2 virus than the B-cells from the recovered patients.
Locci believes the aberrant germinal-center and altered B-cell activity she found is impacting the: a) B-cells’ ability to clear the virus; b) allow for herpesvirus reactivation; and c) promote the survival of autoreactive (autoimmune B-cell clones) that are feeding autoimmunity. This is probably happening in ME/CFS as well.
It’s a pretty darn impressive finding, and it took – a central theme of this conference – digging deep into the tissues. The B-cells found in the blood – which researchers usually study – turn out to be something of an anomaly. Only 2-5% of B-cells are present in the blood at one time, and they’re usually in a naïve or immature state. The rest are present in the lymph nodes, spleen, etc., but it’s apparently only in the lymph nodes that they proliferate, mutate, and become memory or plasma (killing) cells. It’s only the lymph nodes, then, that action is occurring, and that’s why Locci went to them.
PolyBio was jazzed enough by this finding that it and the Wallace Research Fund are now incorporating the ME/CFS field’s absolute favorite virus – the Epstein-Barr virus – into the study, which, by the way, infects and loves to rest in B-cells. (EBV lies low in the very cell designed to kill it.) Three presentations in this conference indicated that EBV reactivation is occurring.
Into the Arteries We Go
“Since 2020, we have been publishing work showing that even mild or asymptomatic COVID infections can have serious cardiovascular consequences, even in previously fit and healthy individuals,” David Putrino, 2025
We’re going to hear more about serious cardiovascular issues in the future – and it’s not pleasant. Infections in the gut are one thing, but the heart and blood vessels and cardiovascular system – that’s striking closer to home. Several studies have found that a coronavirus infection increases the risk of cardiovascular events.
Giannerelli’s assessment of plaque samples from 140 participants found that having a coronavirus infection played a bigger role in plaque gene expression dysregulation than smoking, hypertension, and dyslipidemia (ouch!). It appears that the arterial plaques found in people with long COVID are locked into an inflammatory state.
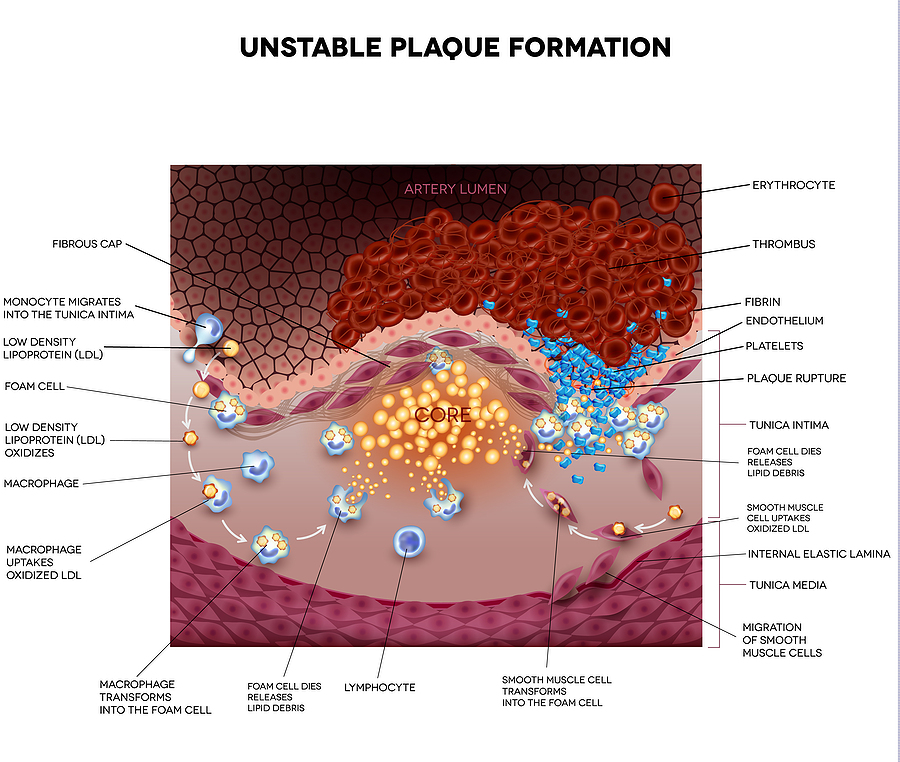
Next in the tissue series came arterial plaques.
Once again, a clearance problem showed up. Macrophages appear unable to clear the dead and dying cells associated with these plaques, likely leading to increased inflammation, impaired tissue repair, mitochondrial dysfunction, and yet another vicious circle. Unfortunately, macrophages are the body’s key defense against atherosclerosis.
Time will tell what the full paper shows, but it should be noted that this finding likely applies primarily to people who already had evidence of atherosclerosis before their coronavirus infection. It fits, though, with the ton of cardiovascular, blood vessel, and autonomic nervous system findings that have shown up in these diseases.
Even two years after the initial infection, Giannerelli found coronavirus RNA was still present in some of the plaques, indicating that the immune system had been unable to get at them and clear them.
The good news about this finding is that atherosclerosis, if it is present, and the cardiovascular system have, of course, gotten a ton of study over the years. Agents that tamp down inflammation, restore macrophages’ ability to remove dead cells, and improve lipid levels in these cells are all potential treatments, should these findings be validated.
Into the Eyes We Go
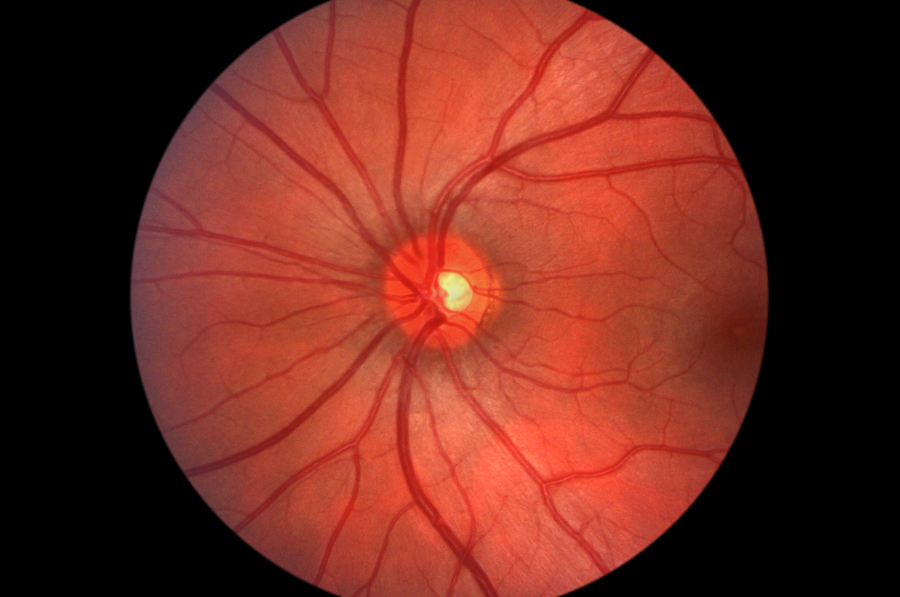
Miller used three techniques to examine the retina. He found evidence of neuroinflammation and misfolded proteins.
Sean Miller’s retinal findings fit nicely with VanElzakker’s brainstem findings (see below). Because the eye is part of the central nervous system and is easily accessible via non-invasive means, it provides a useful way to assess what’s going on in the central nervous system.
Miller’s Yale study was small (n=15) but comprehensive, using three methods (autopsies, live-patient retinal imaging plus ERG, and organoid models) to assess central nervous system activity in the retinas. Increased microglial activity (neuroinflammation), astrogliosis (increased astrocyte levels), and increased activity in neurodegenerative, antimicrobial, and protein-aggregation pathways were observed.
The brain fog and other symptoms have told us that something pretty dramatic is happening in the brain, but the big question this study raised was whether long COVID is associated with an increased risk of Alzheimer’s or other dementias.
Studies have shown that acute exposure to the spike protein can result in accumulations of the amyloid proteins associated with Alzheimer’s. One idea is that the body is actually producing these misfolded proteins to protect itself from a coronavirus, or perhaps other, infection.
In this case, the Yale group was able to reverse the amyloid buildup in the retina using an NRP1 inhibitor (which is not currently available). Pretorius has also found amyloid products in the microclots in the blood, and Baraniuk found them in a 2010 ME/CFS study. The problem is that these misfolded proteins are difficult for the body to break down.
While the convergence between Miller’s retinal amyloid, Pretorius’s fibrin amyloid microclots, and VanElzakker’s possible tau findings in the CNS (see below) presents a compelling narrative, the studies themselves are far too small to provide confidence that long-COVID patients may be at risk for dementia.
A systematic review that covered 940,000 post-COVID survivors and 6.7 million controls (!) did find that 12 months post-infection, long COVID patients showed an 84% increased risk of dementia. The very high heterogeneity, though, suggested that the patients studied, the control groups, and the effectiveness of the long-COVID diagnosis probably varied widely, casting doubt on the findings.
Increased new onset dementia in COVID-19 patients over 50 appeared to be driven primarily by respiratory and vascular (blood vessel) problems, not by the dementia associated with Alzheimer’s. In his substack, Eric Topol reported a 50% increased risk of dementia after three years, but only in COVID-19 patients who had been hospitalized. A UK Biobank study came to a similar conclusion. Older COVID-19 patients who had been hospitalized or had a history of high blood pressure had higher markers associated with β-amyloid pathology (and Alzheimer’s) as well as more subtle cognitive deficits after three years.
Into the Spine We Go
Finally, someone – Mario Murakami from Harvard, of all places – is taking on craniocervical instability not in ME/CFS but in long COVID. Murakami is a postdoc, specializing in neuroanatomy and brain imaging. One of his first projects at Harvard is assessing neuroinflammation in conditions like Long-COVID using PET-MR and magnetic resonance spectroscopy (MRS).
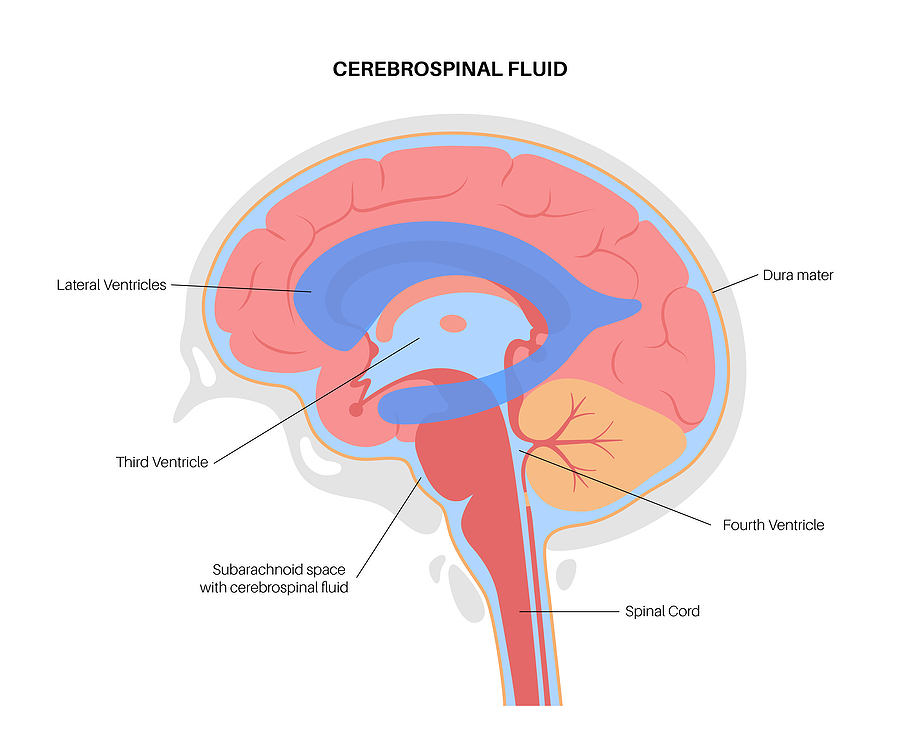
An altered cerebrospinal pulse was found, which could be inhibiting toxins from exiting the brain. The ventricular system drains toxins from the brain.
His pilot brain-imaging study found that long-COVID patients with craniocervical instability(CCI) have impaired cerebrospinal fluid flow – something that could explain the brain fog and fatigue found. Impaired CSF-blood flow is probably no surprise to anyone who knows anything about CCI in ME/CFS, but it needs to be published in the scientific literature to be taken seriously. The fact that this study is coming from Harvard is a substantial bonus.
The very small pilot brain imaging study (n=8) found that CCI compression near the fourth ventricle and the cerebral aqueduct disrupted cerebrospinal fluid flow and glymphatic waste clearance.
Murakami chose these regions because they’re in a kind of hydraulic junction at the transition between CSF flowing up in the brain’s ventricular system and CSF flowing below the brain in the brainstem, cerebellum, and upper spinal cord.
Thankfully, Murakami did not find a dramatic blockage; instead, he found blunted pulse flows. (The CSF flows in pulses.) The craniocervical junction is so tight, though, that a bit of inflammation, muscle weakness, etc., could effect it.
While a blunted CSF pulse flow does not automatically cause problems, it could prevent toxic metabolites from exiting the brain, potentially leading to brain fog, fatigue, and autonomic dysfunction. Although Murakami did not state so, everything from orthostatic intolerance, nausea, sensory sensitivity, sleep disturbance, cognitive slowing, and “sickness behavior” could result.
This study was too small (n=8) to be representative of what happens in CCI. Now that he has his pilot data, though, Murakami hopes to expand the study to include more ME/CFS, long COVID, and chronic Lyme patients. Let’s hope he can get the CCI ball rolling.
Into the Brainstem We Go
That brings us to VanElzakker’s brainstem presentation. A neurologist with a longstanding interest in ME/CFS, Michael VanElzakker proposed the vagus nerve hypothesis of ME/CFS many years ago, suggesting that small infections near the vagus nerve might have major effects.
(You might or might not wonder why VanElzakker spells his name VanElzakker instead of Van Elzakker? I wondered that for many years, so I looked it up. It turns out that when many Dutch people emigrated, the clerks in the immigration offices – being the blunt instruments they were – simply merged Van and Elzakker (which refers to alder trees – nice!) into VanElzakker. So now we know! 🙂
Years ago, VanElzakker pointed out that most brain scans scan from the top down and are not good at assessing the brainstem.
VanElzakker aimed his MRI/PET scan towards the bottom of the brains of long-COVID patients, and found signals that suggest that inflammation was particularly high in the nucleus of the solitary tract, right where the vagus nerve enters the brainstem.
Since this region regulates sensory and gut-brain signaling, the autonomic nervous system, “sickness behavior” (whoa!), pain, and more, the potential for mischief in these diseases is high. Everything from fatigue, nausea, dysautonomia, sensory sensitivity, pain, sleep disruption, and “sickness behavior” could result.
Additionally, disruptions to blood vessels and the blood-brain barrier in the brainstem suggest that vascular problems in the body extend to the brain as well.
VanElzakker also found 4-fold higher p-tau217 levels in long-COVID patients than in healthy controls or ME/CFS patients. Elevated p-tau217 levels are associated with an increased risk of Alzheimer’s. Because they could also be caused by a number of other things (neuronal stress, blood-brain leakage, blood vessel injury), we can’t say that long-COVID patients are at a higher risk for Alzheimer’s, but it’s definitely something to keep an eye on.
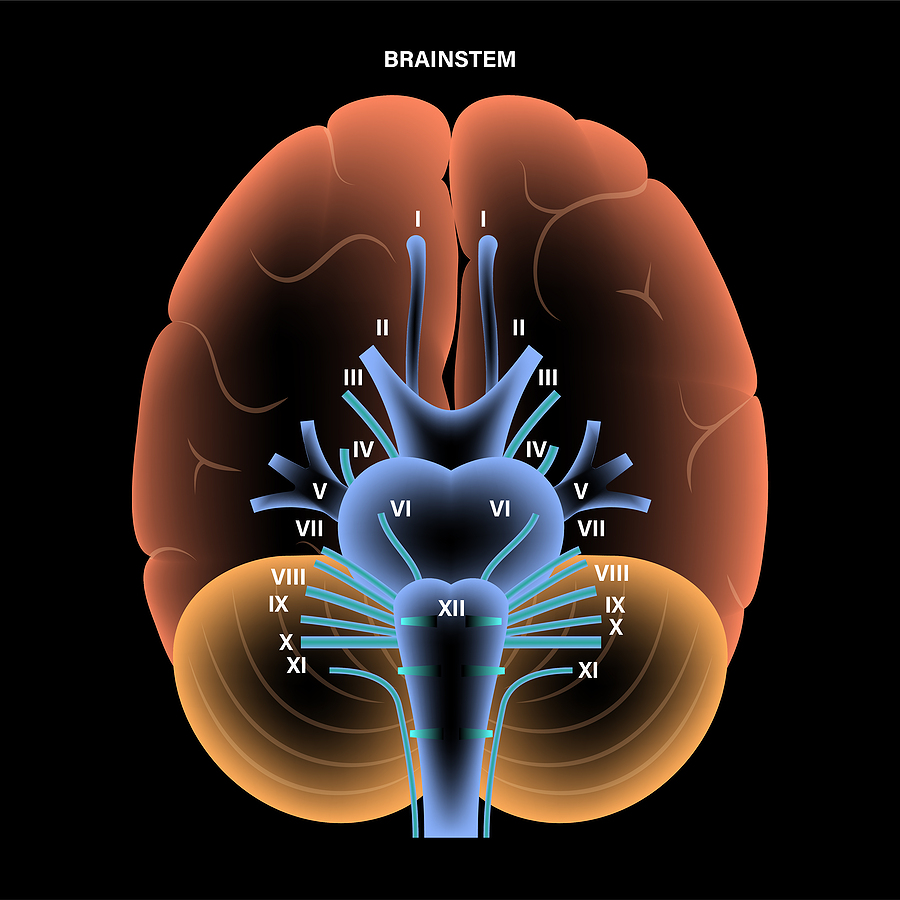
X at the bottom of the brainstem marks where the vagus nerve comes in. This is where inflammation was found.
This finding could point to a wide variety of treatment options, which include anti-inflammatories, vagus nerve stimulation, breathing practices, blood vessel therapies, and more.
There are some cautions. As most brain imaging studies are, this study was small (23 long-COVID and 14 COVID-recovered controls), and the TSPO signal used does pick up inflammation, but cannot tell us what cells it’s coming from (microglia, astrocytes, macrophages, the blood vessels).
Hopefully, with this data in hand, we’ll get a larger PET-MRI/blood-biomarker study that tracks things like symptoms, autonomic nervous system activity, sensory processing (pain, touch, etc.), cerebral blood flow, cognition, and p-tau217 and amyloid/tau levels.
Conclusion
We’re getting lots of interesting findings from the blood, but it’s possible that direct examinations of the tissues are the way to go.
Donation Drive Update
Health Rising is committed to keeping up the “big ideas” in these fields. If that supports you, please support us.
Thanks to everyone who’s brought Health Rising to about 2/3rds of its goal!
Keeping on top of major opportunities and themes in long COVID, ME/CFS, and fibromyalgia is a major goal, and in this part of the Symposium, two immediately stood out. One – a potentially transformative project – the Long COVID Cure Initiative has begun. Two – these diseases may have been “invisible” to the naked eye, but once you peer into the tissues themselves, lots of problems are showing up, and in lots of places.
If keeping up with major findings supports you, please support Health Rising. Thanks!



Polybio are amazing! Very thankful for their efforts
Curious about this statement: ‘ The idea is that leaky gut linings are allowing the spike protein or the coronavirus to spill into the bloodstream.’
Even if we take for granted that the epithelial layer is compromised, isn’t it also possible that our own good bacteria are entering the bloodstream and becoming ‘antigens’? Why do they think it’s just spike proteins causing antibody reactions?
I think they would entirely agree with that – and that would include EBV as well. Since one of the places EBV makes its home is the B-cells (you gotta give it up to EBV – its a very clever virus!) anywhere the B-cells go, EBV can go – and B-cells are found in the gut lining. I asked Perplexity AI about this. This is what it said
“Yes. EBV-infected immune cells are commonly found within inflamed gastric and colonic mucosa, meaning EBV can be present in the gut lining—mainly in infiltrating lymphocytes rather than as a classic “gut epithelial” virus.
EBV primarily infects B cells, which can infiltrate the lamina propria and lymphoid structures in the gut such as Peyer’s patches”
EBV is able to affect the gut microbiome as well.
If it turns out COVID-19 can hide in the epithelium that could be a major breakthrough for long-Covid. By the way, I used Larazotide last summer and had some interesting results. PM me if you want to discuss.
My daughter is currently on Larazotide. She did 2 weeks once a day and now doing twice a day for another week before starting Ozonated glycerin with binders and then a tryptophan supplement. All part of a doctor’s beginning long covid protocol. It is quite new still and not seeing much of difference yet but am very curious. Did your interesting results last? Not sure how to private message on this platform otherwise I would have.
Thanks
Hi Randee, plenty I could tell you. Are you on Reddit? If so, you could leave a message with the word Larazotide in this thread and I’ll pm you from there:
https://www.reddit.com/r/LongCovidTrials/comments/1usrayw/helpful_list_of_expected_clinical_trial_results/
Hi Ay,
Just responded on Reddit as suggested with Larazotide. My username is : Big_Spell_3813.
95% of the population has had the EBV virus which means that EBV remains in the cells of most of the population. EBV may be a marker for ME/CFS, but it is not the cause. Let’s ponder what is causing immune dysfunction that allows EBV and other herpes viruses, bacteria and mycoplasma to reactivate.
While it’s true 95% of people harbor latent EBV, the vast majority control it perfectly. In ME/CFS, the mounting data suggests atypical, localized herpesvirus reactivation isn’t just an incidental byproduct—it is actively driving the ongoing pathology.
The research strategy right now is a deliberate two-step process: first, establish undeniable physical proof that these active tissue reservoirs exist. Once we have that proof, science can properly map out exactly what kind of upstream immune failure or initial hit unraveled the body’s viral defense systems to begin with.
Maybe it’s more like a correlation: leaky gut lining leads to more spike protein in the blood. That doesn’t mean that it needs to come from the gut lining.
If for example improving leaky gut lining improves the working of immune cells (like less exhaustion), they might be able to clean up more spike protein? Or remaining reactivating virus in other parts of the body gets cleaned up better?
This research is already improving our understanding as it is and more work can lead to even better answers.
Sounds to me like a call for long-course antivirals.
In getting to 90% recovery where I can work and exercise after 11 years of ME I will say that fixing my gut through the carnivore diet was key
As long as I still to a low carb fatty meat based diet I’m OK
I’ve heard many stories like this and had a similar experience myself. You just have to wonder what it is about carbohydrates that triggers the symptoms. And why Metformin, for example, works well as a prophylactic for Covid.
Yes but why
The aside about the spelling of Van Elzakker is definitional comic relief…and much appreciated!
:). That was fun!
Keep up the great work!
Thanks so much! 🙂
Ive been saying this for years. Its SO CLEAR. Its also worrying as its a systemic weakness
I’m not nearly as medically well versed as Cort & many of you here, but I’ve had ME/CFS since a whiplash injury 30 years ago. I also had two separate positive tests for EBV years apart & several years before the accident. I’ve been frustrated by the sole focus being on the viral component in ME/CFS research, when there are a percentage of people who, like me, had a physical trigger.
I recall decades ago that a Belgian study had found a much higher correlation of neck/spinal injury & ME/CFS than other types of physical injury/trauma. I’m glad some are looking at the tissue around the brain stem & upper spine. There may be secrets there for a subset of us.
Strangely, my sister had a whiplash injury & within a few months had developed tumors, multiplying up & down her spine, ultimately killing her. I know it sounds bizarre, but it seems like both of us had a cascade of events triggered by a neck injury.
I had the same Deanne, a car accident where I was hit twice – once from behind, and then again from the side – no broken bones, but M.E. came on within days, but took a while to be diagnosed – I’m still so sick 18 years later!
Thank you for sharing your experience. I was actually healing from long Covid until an oral surgeon whipped my head back and forth to remove a cracked molar. My neurologist believes that his action exacerbated a preexisting TBI from a coup contra coup whiplash injury I got in 2015 in a car accident where C2 and C3 were broken. I was again starting to slowly heal and regain some lost ground when I experienced an injury to L5 and got a pinched sciatic nerve. Long Covid changed so much in my body that I couldn’t tolerate any painkillers that acted via the CNS…which is basically all of them. The connection between the spinal cord, nervous system and brain stem/ cerebellum and long Covid are under appreciated. I thought I was alone…but reading your comments helped me realize that these physical injuries are also drivers of long Covid/ ME/ CFS.
Everytime I pick up an infection my lymph nodes always express themselves.
When i got covid 19 the exray of my lungs showed what they thought was blood clotts turned out to be hundreds of lymph nodes expressing themselves via ct scan.
When I received my third and last covid vaccine my armpit swelled to the sized of a grapefruit. When i went,in the 90s to Calgary,Alberta to receive intervenous IV vitamins the nurse later added a tiny shot of molibdimum into my IV bag…the result was my entire upper chest and stomach area with hives the size of grapefruit that later subsided in about 1 hr.
The attending doc advised chelation which was way out of reach financial wise…good thing,…i later found out that the form of chelation he advised is now no longer advisable.
I also am a victim of not one but two rear end collisions …one of which sent my head clean through the rear window of my truck which in the 1990 model of GMC was the only year the bench seat did not include head rests which could have prevented my head from this injury….knocked out COLD for im not sure how long.
In getting to 90% recovery where I can work and exercise after 11 years of ME I will say that fixing my gut through the carnivore diet was key
As long as I still to a low carb fatty meat based diet I’m OK
There’s going to be a gut subset and you are it! Congrats and thanks for sharing that 🙂
Every once in awhile I comment. Re Van Elzakker reference to vaga nerve. I’ve had CFS since 1968 Hong Kong flu. A few years ago I saw diagram of Vagus nerve,function unknown at time. Eureka,the gut brain connection. I ordered an Alpha Stim,developed by guy who invented ECG. Upon first use I became super women,didn’t require any sleep. This miracle ended 4 years later when contracted RSV.
The gut – brain connection also now being recognized in Parkinsons.
I now loan to family/ friends to assist them with sleep pre exams,etc
I see there are similar products on market but I cannot attest to them.
Best of luck ,all.
Joan Gibson,Retired Psychologist
“EBV (which actually hangs out in the B-cells) had penetrated the lymph nodes and was inhibiting the immune response needed to eliminate them”.
THIS is such an important statement. From my decades of M.E. this the CAUSE of M.E. – EBV infecting the immune system.(B cells). Everything else is an effect.
I would like to see a time-line of the ages and number of cases of ME/CFS diagnoses since the first clusters were identified in the 1980’s. I believe that many conditions have been swept into the ME/CFS basket for lack of a better diagnosis. Is there a finite time period for new cases. I would also like to know how you study the effects of Long Covid when there are thousands of mutations.
A bit or research and I answered my own question.
List of myalgic encephalomyelitis and chronic fatigue syndrome outbreaks
https://me-pedia.org/wiki/List_of_myalgic_encephalomyelitis_and_chronic_fatigue_syndrome_outbreaks
This is of particular interest and suggests a single cause: “From 1984 until 1992 [at publication of this text] an endemic period occurred in which an usually large number of cluster and epidemics of ME/CFS have been recognized in North America.
Hi Betty,
Very interesting paper. Looks like I am at the end of the 1984 episode in Montreal Canada since I have been sick since 1990.
I have said this before and I will say it again- I became ill with me/cfs i march 1982 while living on the west shore of lake tahoe – just south of tahoe city. Two years before the incline village outbreak. And my doc was Dr Peterson.
Oops – IN march of 1982!
To me the lymphatic/ tissue connection makes sense in my experience of long covid. I have hundreds of large cracking lymphnodes all throughout my gut, chest and now reaching into my neck and skull. Botoxing my skull is the only way to relieve the nerve pain radiating throughout my face.
My diaphragm can hardly move because of these lymphatic palpable nodules. When I press on these areas (especially armpit collarbone) it sounds like bubblewrap. Relief is shortlived and rebounds if done too much. But a person gotta breathe!
Whenever I get a virus symptoms become near E.R lvl for weeks. Digestion and breathing got so restricted after 6 years that I developed gastroparesis. Airbubbles got trapped in my stomach that made me stop breathing at night. It got pretty severe at one point… i have severe spo2 drops (78%) And no doc takes me serious. Just those blank stares with the offer to see a psychologist…
I always wondered about the lymphnode part. I have never heard about someone with similar symptoms. Had an MRI done in Turkey-full body. Found nothing wrong with lymphatic system. They did find modic type 2 herniation C5-C7 and a 12-15cm long syrinx from T8 till L2. It would come as no surprise that the same psychosomatic treatment got offered. No one has once looked at my images or results! 28% intermediate monocytes? Why would that be of any concern! But I am bragging now
While we wait for THE ANSWER and for big pharma to formulate treatments we do have some home remedies at hand that can help to calm a leaky gut.
I personally have experienced profound healing impact from homemade kombucha (unsweetened). I took two tablespoons two/three times daily and after one month my crippling gut pain/IBS symptoms left me. I continue to take a small amount each week now.
There is plenty of research supporting the use of fermented foods for gut health.
Not THE answer or THE cure, but may offer many people relief of some symptoms….while we wait……….
When will we get MECFS tissue biopsy results? Or any (LC) tissue biopsy results? Seems like Polybio has been talking about that for 4 years now.
Thanks as always Cort! I just had my results from GI Mapstool test – and zonulin markers are abundant! After 8 years of MECFS and gut problems with it, I attribute my gut improvement to lots of fibre, glutamine (1g daily) and NOW foods Gastro Comfort – zinc carnosine, slippery elm and aloe vera. I can now eat pretty much anything (having had heavily restricted low-FODMAPs diet). I still have to be mindful of high histamine foods, still gluten free, but dairy seems to be ok, and even the odd coffee – woop! Sugar and alcohol, however, is an absolute no-no – however much my body begs!
Congratulations and thanks for sharing that 🙂
As much as I hate to believe it, this could be bio weapons let loose on the population
One deep dive into lyme. Many believe lyme was an engineered bio weapon from plumb island military base directly across the water from the first known cases of lyme (“juvenile arthritis”)in and close to, the town of Lyme, Connecticut.
While its difficult to distinguish between fact and fiction there are now reports of farmers finding boxes filled with tics in their farm fields
There were 7 workers from the Wuhan China lab that were the very first to be “infected” with covid 19 before any civilian people fell to covid 19
Call me a conspiracy theorist, but it wouldn’t be the first time a country
Harmed their population
Hi Rooney, A colleague told me about this book on Plumb Island: This first major non-fiction book focusing exclusively on Plum Island is “Lab 257: The Disturbing Story of the Government’s Secret Plum Island Germ Laboratory”. Published in 2004 by investigative attorney Michael C. Carroll, it exposes the history of the island’s animal disease center and the biological threats posed by the facility.
What is so curious and disturbing is that at the end of this work of non-fiction, the author states that this was a work of “fiction”. I guess, as an attorney, he was protecting himself.
My family is from the south and out in the woods hunting and fishing for 100 years. Of course, there were ticks, but no Lyme Disease. I suggest reading this book and making up your own mind.
Thank you for the summary, Cort.