


“We’re saying that ME/CFS is a program priority now…Give us a chance to prove we’re serious – because we are.” Francis Collins
No one could have expected this. The NIH was supposed to reinvigorate ME/CFS research, not watch a vital aspect of it go down the tubes. According to Freedom of Information Act requests (FOIA’s), fewer ME/CFS researchers applied for the fewest individual grants in 2017 (n=8) and 2018 (n=8) in memory.

The NIH has failed to re-invigorate or even stop the decline in the most important source of funding – individual research grant applications
The individual research grant application problem dwarfs everything. Three small NIH-funded research centers cannot and aren’t meant to carry the load for a disease. The Intramural Study is promising, but is going to take years to complete – and it will need interested researchers to follow up on its findings.
“It is very important to know that the vast majority of NIH funding goes to investigator-initiated grants that be submitted at any time.” Vicky Whittemore
The NIH has a serious problem on its hands. Four years after it said it was committed to reinvigorating this disease, the individual grant applications that basically run the show over there not only aren’t increasing – they’re actually sinking fast. Since most of the NIH’s budget goes to individual-initiated grant applications, that’s a big deal. No disease program can be successful at the NIH without a steady stream of researchers submitting applications.
Grant Applications for ME/CFS
- 2011 – 20
- 2012 – 30
- 2013 – 16
- 2014 – 18
- 2015 – 26
- 2016 – 13
- 2017 – 8
- 2018 – 8
It should be noted that the NIH has always complained about the lack of grant applications. They complained about the few applications they were receiving back in 2011 when ME/CFS researchers submitted 20 of them, and in 2015 when 26 researchers applied.

Have the Research Centers Hurt the Individual Grant Application Rates?
The Research Center applications in 2017 were certainly expected to tie up some of our best researchers and therefore produce a decline in individual research applications that year. We can’t, however, blame the Research Centers for the decline we’ve seen since then.
At the very most the three winning Research Centers tied up nine potential individual applications. Adding 9 more applications from 2017-2018 – a very unlikely scenario – still leaves us with a still substantial decline in application rates.
It’s quite unrealistic to assume that the nine projects developed for the Research Centers grant applications would have been turned into individual grant applications. My guess is that in the normal course of events only 3 or 4 would have been submitted leaving the situation virtually unchanged, and indicating that the bad old days really are looking like the good old days now.
A Stark Reality
“We recognize and empathize with the suffering experienced by people with ME/CFS and their frustration that so little is known and so little research has been done to find answers. We aim to change that. The NIH is committed to unraveling the underlying biologic cause(s) of ME/CFS as swiftly as possible.” Collins and Koroshetz
The one good thing that may come out of this mess is how utterly stark the problem is. Now that the bottom has officially fallen out, it’ll be interesting to see how the NIH responds.
Almost four years after Dr. Collins’s promise that the NIH was finally going to get serious about ME/CFS, it’s clear that what they’ve done isn’t working – which is really no surprise. The NIH, after all, immediately broke Collins’s promise: it has never come close to being serious about this disease.
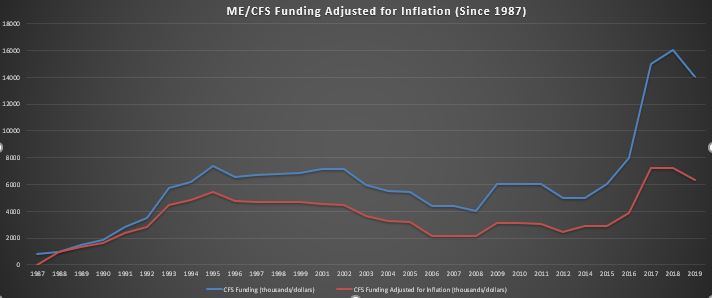
The recent boost in NIH funding for ME/CFS wasn’t much of boost, historically speaking, at all. The NIH was spending almost as much money on ME/CFS in the early nineties (red-line -spending adjusted for inflation) as it is today.
The NIH did create three small research centers and fund one intramural study, but in doing so committed about the same amount of money into ME/CFS that it had in the past. It assured us that a Working Group, which had never been effective before, was somehow going to change its spots and turn into an ME/CFS research generating machine. Without dealing with the individual research grant problem it suggested – without ever telling us how – that that problem was going to resolve itself.
“Serious” Effort Needed
The NIH has failed so miserably thus far at invigorating this field that it must – if is serious at all about ME/CFS – rethink its approach. The beauty of the collapse in grant applications is that it’s so total. There’s no grey area, no promising signs – it’s a complete and utter failure.
The NIH has to grapple with the fact that its preferred way of working with ME/CFS – the Trans-NIH Working Work – is an abysmal failure. When over half the Institutes in a Working Group can’t contribute even a minimum amount for the group’s one big initiative, something is seriously wrong. (Not having the buck stop anywhere is a sure recipe for indolence and inattention, and it has been just that. )
(Check out the graph above. A precipitous decline in ME/CFS funding began 2001 when NIAID kicked out ME/CFS, and the Trans-NIH Working Group took over responsibility for ME/CFS. It hit it’s nadir in 2007/2008, jumped up for a few years when the RFA money came in, then declined again.)
Strategic Plan
It’s now abundantly clear that one funded grant opportunity (RFA) and a conference every ten years is not enough to put this field on a sustainable trajectory. If the NIH wants to succeed, it has to create a strategic plan that, step by step, methodically builds this field over time. That includes funding RFA’s, providing regular reports that assess performance metrics and benchmarks, providing a home for ME/CFS, etc.
The NINDS panel that Vicky Whittemore and Walter Koroshetz put together to assess the way forward may provide that. It is due in the fall.
If the NIH doesn’t produce a coherent, long-term strategic plain, we will surely be back doing this again and again and again.
In the meantime, we should recognize that the NIH is designed to respond to researcher interest – not disease burden or need. It actually appears structurally designed (probably inadvertently) to make it difficult for controversial diseases – particularly with diseases like ME/CFS, which lack a clear pathophysiology – to get a leg up.
This isn’t easy for them either. (Ron Davis said it wasn’t going to be easy.) There’s much we don’t know about the NIH but the idea that someone there is going to suddenly plunk $50 million down on the table for ME/CFS is apparently harder than we know. It took Vicky Whittemore over a year to get three small research centers (and one data center) funded – and that was with Francis Collins’s public support.
Two-Pronged Attack To Produce Major Change
We have the ability, though, to force the NIH to give up its almost complete reliance on researcher interest and fund ME/CFS research based on the need that is present. One way to do that is by telling our story to the people whose job is to look after the American people – our Congressmen and women. They have the power to force the NIH to change its ways.

The NINDS report plus support from Congress will give us an opportunity to push the NIH to finally get serious about ME/CFS
The NIH also has internal mechanisms that can help and we have supporters there. The Institute of Medicine (IOM) and Pathways to Prevention (P2P) reports gave Francis Collins the foundation to publicly state this disease has been neglected and needs substantially more funding. That gave us a substantial boost, which then appears to have foundered on the structural constraints that were still present; namely our reliance on the Working Group.
The NINDS panel report due in the fall should give us substantial ammunition to push for major changes. Coupling that report with strong Congressional support could give us the wedge we need to finally produce major and lasting structural changes in the NIH’s approach to ME/CFS.
Our next opportunity to enroll Congress in supporting our efforts to produce meaningful change at the NIH will come in a couple of weeks on Advocacy Day – easily the biggest one yet.
- Coming up next – a chat with the SMCI’s Advocacy Director – Emily Taylor.
Your Support Keeps Health Rising on the Web



Researchers are not foolish. Perhaps they got tired of hitting a brick wall at NIH and turned to the independently (under)-funded but more committed alternatives. The collegial meetings and cooperation worldwide from other organizations shows more researchers are working in the field. They just don’t trust that $ will come from NIH. Unfortunately, I don’t think NIH will recognize they are a big part of the problem with continuing paltry funds for research on this devastating disorder.
That’s a common belief and it makes sense, but the stats do not bear it out. Based on my hopefully correct analysis grant acceptance rates for ME/CFS appear to be at least normal and perhaps higher than normal.
Another mistaken but understandable idea is that the preponderance of pain researchers on earlier review panels keep grant applications low. They surely did turn off some applicants but when the pain reviewers were replaced by ME/cFS reviewers grant applications remained low.
Plus ME/cFS researchers responded very well to the two funded RFA grant opportunities that took place over the past 15 years (the neuroimmune RFA and the Research Center’s RFA). So they will respond – but only when guaranteed money is present.
It is puzzling because I agree – the field seems stronger than ever before – while the situation at the NIH is getting worse.
what is clear is that this field cannot move forward quickly without researchers applying for the kind of big multi-year, multi-million grants the NIH provides. There’s just no substitute for them.
Even with the NIH’s paltry funding it’s still easily – very easily – the biggest funder of ME/CFS research in the world.
I’m new to cfs research (reading, not conducting). Can you point me toward any studies that provide more descriptive statistics – regarding comorbidities, disease impact, etc.? I can’t comprehend the lack of interest in researching this.
I did find some of your resources, but since the most recent descriptives are from 1996, that illustrates the issue precisely.
I’m so glad you asked!
An interesting study just increased prevalence rates significantly
https://www.ncbi.nlm.nih.gov/pubmed/30671425 which
“Extrapolating from this frequency of diagnosis and based on the estimated 2017 population of the United States, a rough estimate for the number of patients who may be diagnosed with ME or CFS in the U.S. is 1.7 million to 3.38 million.”
With the disease producing very high costs
“Average annual costs for individuals with a diagnosis of ME or CFS were compared with those for lupus (all categories) and multiple sclerosis (MS), and found to be 50% higher for ME and CFS than for lupus or MS, and three to four times higher than for the general insured population.”
A 2011 CDC study estimated that the yearly economic costs of the disease in the state of Georgia were $1.2 billion dollars
https://www.ncbi.nlm.nih.gov/pubmed/21251294
Lenny Jason’s 2008 study estimated the economic impact in the U.S. at around 20 billion a year
https://www.ncbi.nlm.nih.gov/pubmed/18397528
Hi, thanks so much for for your interest. Here are some more links for you :
https://www.frontiersin.org/articles/10.3389/fped.2019.00012/full
https://www.ncbi.nlm.nih.gov/pubmed/25274261
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3229491/?report=classic
http://www.nationalacademies.org/hmd/Reports/2015/ME-CFS.aspx
https://www.frontiersin.org/articles/10.3389/fped.2017.00121/full
https://oatext.com/Estimating-the-disease-burden-of-MECFS-in-the-United-States-and-its-relation-to-research-funding.php
Maybe I don’t understand because of my ME brain fog but it sounds like the blame should be put on the researchers because they are not submitting enough proposals for funding. Please clarify.
I would just say that it’s clear that the current situation is not working. There are a lot of really ill people in the U.S. (and elsewhere) and researchers are simply not being enticed enough to get over whatever roadblocks are keeping them from entering this field.
The roadblocks are real – controversial disease, symptom based diagnosis, few research centers, peer pressure, career concerns …
Researchers have shown up for funded grant opportunities and my guess is that Anita is right – that there is more interest than ever in this disease and a funded grant opportunity would be a huge success.
How can patients help? I mean besides donating to CFS/ME orgs?
By engaging in the advocacy actions coming up in early April and those afterwards. Hopefully we are building to make a big splash in April and again this fall.
Cort, your list of applications by year is missing some information. You have no numbers listed for 2014. It’s also not clear if the reporting is by calendar or fiscal year.
In addition, your number for 2017 omits the applications submitted in response to the RFA. Fifteen applications were reviewed at that meeting, in addition to the 8 applications you noted for that year.
I think I mentioned to you before that the numbers NIH has provided me in response to FOIA requests do not always match the numbers they have provided to you. Some discrepancies might be explained by the different ways we worded our requests, but not all of them. I do not understand why NIH cannot even give us consistent numbers!
I added the 2014 figures that I have.
I asked for the number of applications reviewed by each review panel each year. Some of the applications for the early panels must have come from the end of the prior year.
I wanted to focus on the individual research applications and therefore did not include with research center grant applications.
I believe the Research Center grant applications went in in early 2017 (?) and the Centers were announced in Fall. Because each center application contained three projects, though, the Center application process resulted in as I remember potentially 20 or so individual grant applications.
I expected the numbers of individual grant applications to dramatically increase after the Research Center awards, but it hasn’t happened. Since those researchers have had a year and a half to submit individual grant applications my guess is that the unfunded Research Centers are not going to be a boon for ME/CFS, after all
Instead the applications – even after the Research Center process was complete – has gone down. The first 2019 review panel received 5 applications – up from the year before but similar to prior years and nothing like what is needed to move this field forward quickly)
While we are unfortunately getting somewhat different figures I assume the trend is the same.
The number of applications stamped received and the number that actually make it to the Review group may be different.
The total lack of researcher integrity is amply demonstrated by the fact that no CFS researchers ever actually looked into the incident that the Holmes 1988 CFS syndrome was based on.
I realize saying this pisses people off.
Tough SH*T.
This is provable and I don’t have to mince words.
I am relying on the fact that the history of CFS is documented and
some day, some new researcher who doesn’t know the ME/CFS community wants the original evidence base suppressed will just go ahead and look.
The the 100% negligence by those claiming they wanted to “Solve CFS” is going to be revealed. The utter lack of “science” by even “good doctors” will be apparent to all.
There is not a damn thing anyone can do to stop this.
The truth will come out.
What, in another 50 years when we are all dead? if it hasn’t come out in 30 years, what do you feel will change in the future? And just because the truth comes out doesn’t mean ANYTHING WILL CHANGE.
Someone posted in my Ehlers-Danlos forum the links to several articles about ME/CFS researchers being harassed (think PACE study). The articles were inclined to link disinclination to pursue CFS research because of this harassment.
Here is the link for one of those articles:
https://www.reuters.com/investigates/special-report/science-socialmedia/
I don’t know if events like these are having any impact on grant applications, but it’s something to consider.
I wish there was some way to find out. Articles like the Reuter’s article do us no good and are kind of ironic since I’ll bet non-CBT/GET researchers probably really LIKE the ME/CFS community. We’re knowledgeable, committed and engaged.
Something else I wanted to add, although not precisely relevant to this topic, is that researchers have developed a blood test with a high rate of accuracy to distinguish patients who have fibromyalgia from several other disorders. I only post this because fibromyalgia is rather like a cousin to ME/CFS. Perhaps this research could lead to discovering markers for CFS as well. Might it be a good idea to request a grant for this?
https://news.osu.edu/experimental-blood-test-accurately-spots-fibromyalgia/
It seems like the best thing to do at this point is to contact our Congressmen and Senators regarding the lack of funding from the NIH. The people have to be heard.
It is crucial to do that. Congress is the one group that a) is concerned when the NIH doesn’t treat a group of illnesses right and b) can do something about it.
We’ll have the opportunity to contact them soon.
I am astounded at reading this report. Has no one read Dr Judy Mikovits and Kent Heckenlively book called “Plague – One Scientist’s Intrepid Search for the Truth about Human Retroviruses and Chronic Fatige Syndrome (ME/CFS), Autism, and Other Diseases”?? She did a study that clearly delineated a retro virus called XMRV was infecting 4 – 8 % of healthy population and that 14 out of 17 children with autism showed evidence of this virus after vaccination. In 2011 her research showed vaccinations were contaminated with XMRV. When word got out she was jailed and ….. a long story – read her book. She is now posting on YouTube for the first time.
And I thought it was better in the Us then in Belgium.:-(
But even then, there is at least something and some good researchers. Here is nothing.Go and live with it (means lay in bed and die because mine is progressive)or GET and CBT.
It is so depressing all…
Ill since ’88, really breakthroug in ’93, many promisses from researchers that where broken, my life has past away in bed and I even do not hope anymore, can not hope anymore to live long enough to make it to the first treatment or test.
I agree with you konijin. Also, even if successful treatments are eventually discovered – probably not in my life-time though. After decades of low income & poverty conditions – the final insult would be – who will be able to afford them anyway. I guess we all just continue to live in hope.
Please do not give up hope. Dr. Klimas and Cortene clinical trials are underway in ME/CFS plus remember that the NIH is putting alot of money into developing – they hope- 15 new pain drugs over the next 5 years. Some of those will surely be applicable for ME/CFS.
Read ‘Medical Medium’ and ‘Life-Saving Foods’ by Anthony William.
Google ‘Cincinnati EBV’ (from another of Cort’s posts) tying EBV to 94+ chronic diseases via transcriptions (RNA).
This NY Times best-selling book is aimed at CFS people and gives us hope, and info on what to do until they come up with a cure in 20 or 30 years.
Over the past couple years, it has helped me get over the FM and Vagus nerve inflammation part of CFS, which has bumped me up a point or two on the 0-10 Energy Scale.
I can now bicycle twice a week on flat roads and sleep long enough to dream (>4 hrs/nt), while that was not the case for years; I was stuck somewhere between too awake to sleep and too tired to read.
I am still working on the severe (and often burning) brain inflammation part, and raising my VO2max (cellular oxygen uptake), which is in the toilet for CFS people (<44% normal per one study).
If 94+ diseases are caused by the dozens of 'undiscovered' mutated strains of HHV-4, (which almost every adult worldwide now carries at least one strain of), maybe the people researching the 93 others will stumble across a quicker cure for CFS.
Hopefully they expand upon the Cincinnati study. MS, Lupus, RA, and Diabetes were some of the other chronic diseases tied to HHV-4 (EBV) virus 'for sure'.
Anthony says the toxin-eating EBV virus has different symptoms depending on what toxins (heavy metals, chemicals) it has been exposed to.
Since patented drugs are chemicals by definition, the pharmaceutical industry has zero interest in research that shows their semi-toxic products are actually lowering the immune system, feeding chronic diseases, and slowly destroying the toxin-filtering liver and kidneys.
…Just think of what would happen if a healthy person took your prescription meds.
So private research efforts do need to be supported, and protected from the politics of our for-profit medical system IF a non-patentable cure (thus non-toxic) is the only cure.
Watched the movie, “What About Me?”last night on Amazon and was reminded of the sordid history of our disease. One fiasco after another! When Judy Mikovitz found XMRV they got rid of her and all her work yet she was not the only one to find XMRV in ME/CFS. It was also found at the NIH and by researchers in Germany. As I recall those who found no presence of XMRV did not actually follow the same protocol that Judy used….? CDC said it wasn’t there and then all the evidence was evidently destroyed. I was also reminded about the secret file about ME/CFS locked up in the UK for 79 years! What’s up with that and why is it still unknown! In addition to XMRV I wonder what connection there is to ME/CFS with people given multiple vaccines…..has anyone correlated vaccination histories and ME/CFS worldwide? In addition we have the effect of all the various toxins in our enviroment….has anyone tested the blood of ME/CFS patients for these chemicals? It seems to me that interesting research is done and then blocked from continuing further and nothing comes of it, over and over again. The WHO designated ME as a neuro-immune disease in 1969 and still we are arguing about whether it is truly a physical disease. Why? I am very grateful to those who are still doing good research in this field but given the history of how anything connected to ME/CFS is dealt with, including the patients, I understand why anyone would be reluctant to take it on. According to “What About Me?” there are over 20 million people with ME/CFS worldwide and by now many more. What is being done to collate all the information that we would all be willing to share to try to get at what is really going on and what to do about it? If not now, when?
“In the meantime, we should recognize that the NIH is designed to respond to researcher interest – not disease burden or need. It actually appears structurally designed (probably inadvertently) to make it difficult for controversial diseases – particularly with diseases like ME/CFS, which lack a clear pathophysiology – to get a leg up.”
I’m really curious about best sources to learn about the NIH structure and how it relates to the broader politics of getting this or that funded; was there a good book/s that you read by historians that you’d recommend? Like, who are the academic historians of medical research who talk/write about those things?
If various mutated strains of HHV viruses combined with trace toxic heavy metal and chemical poisons in our systems (from foods, environmental exposure, vaccine adjuvants, patent drugs) ARE the underlying cause of almost all chronic diseases and cancers, making it likely 100% of our population will soon have a chronic disease or cancer (instead of just 50%), what does that mean for our society and current medical industry?
I have a feeling that we will find out over the next 30 years. It is going to be interesting.
It’s a catch-22
Scientists don’t join the field due to lack of exciting footholds and so whatever studies they have in mind are inherently speculative and less likely to be funded. So most scientists don’t bother with the substantial amount of effort required to submit applications as they don’t expect to be funded.
The solution is to focus on building research capacity.
This means:
Patient charities and crowd-funding to fund pilot studies.
NIH to fund more specialist research centres, which will in turn attract more scientists and funding.
I’m also wondering if there is any way we could fund some specialists to assist scientists entering the field to make applications so they don’t have to invest as much personal time?
Look at Jarred Younger, though. Getting NIH grants – as busy as can be – this field can work for researchers.
Maybe it’s a networking issue. How are these scientists finding out that ME/CFS is a wide open field unless they’re already wise to the situation? There are some very promising avenues of research, and CBT/GET is a no-go, but that’s not immediately obvious to someone on the outside.
As a scientist, I’d say that the number one impetus for jumping into a new field (in my experience) is meeting a scientist in that field. Usually face to face at a conference. This puts ME/CFS at a severe disadvantage simply because we’re starting with such low numbers of dedicated researchers.
News articles aren’t usually nuanced enough to express the opportunities that exist right now in ME/CFS research. [Unless there’s another connection, like Dr. Phair who made contact with Dr. Davis at Stanford.] Jarred Younger was already a member of the CFS research community, I think.
Maybe what we’re seeing is simply a lag while the news trickles out to the rest of the scientific community.
I should also point out that science operates based on paradigms; without a coherent paradigm for the disease, the risk for the scientist to waste several years on a dead end is very high. I’m guessing (hoping) that after the next few breakthroughs the field will become much more attractive to researchers.