


Geoff’s Narration
The GIST
“It’s (ME/CFS) a jigsaw puzzle, right? And we have a couple of the pieces that I think are going to be really important to framing out the rest of the picture.” Steve Gardner, CEO and co-founder of PrecisionLife

Steve Gardner’s PrecisionLife is running towards, not away, from ME/CFS and long COVID.
I spilled the beans early in my talk with PrecisionLife CEO and co-founder Steve Gardner. I don’t usually pick favorites, but I told him that PrecisionLife is my favorite ongoing effort!
Why? Because it’s actually chosen ME/CFS and long COVID to highlight its superpowers, and is funding all its ME/CFS and long-COVID studies itself.

Instead of running from these diseases, PrecisionLife is running towards them.
Doing Genetics On Steroids
As an earlier blog and talk with Steve (who is a dead ringer for the holograph doctor (plus more hair) on Star Trek Voyager :)) demonstrated, PrecisionLife could be described as doing genetics on steroids. Instead of determining if the frequency of this gene variant or that gene variant is increased, PrecisionLife is determining what sets of gene variants/mutations (gene signatures) are increased (or decreased) in these diseases. Then it assesses the biological pathways they’re involved in.
By doing that, PrecisionLife ends up with something that more mirrors what’s actually happening in the body than your standard genetic study.
THE GIST

The genetic evidence suggests that targeting the right patients is going to be crucial for producing successful clinical trials.
- I usually don’t pick favorites, but PrecisionLife is my favorite ongoing effort. Why? Because instead of running from these diseases, PrecisionLife is running towards them. It hopes to use its work with ME/CFS and long COVID to showcase what it can do.
- PrecisionLife could be described as doing genetics on steroids. First, they determine which combinations of gene variants/mutations are associated with an increased risk of getting ME/CFS or long COVID. Then they determine the biological pathways they affect.
- Next, they look for the mechanisms driving those pathways and drugs that can tweak them. They identify patient subsets most likely to benefit from those drugs and work to secure funding for clinical trials.
- I talked with PrecisionLife CEO and cofounder Steve Gardner earlier about PrecisionLife’s exciting earlier study. This new study – which included 8x as many ME/CFS patients from the DecodeME biobank – was something else indeed.
- The growth of the findings was not linear – it was more exponential. They didn’t find 8x more genes associated with ME/CFS – they found 140x more genes (!).
- You might think the more the better, but it would have been easier for all of us if fewer genes had been uncovered. The large number of genes involved in ME/CFS means it’s a highly “polygenic” disease, in which thousands of genes, in different combinations, work together to increase the risk of developing it.
- Steve said that untangling this mess and deciphering the signals driving the subsets in ME/CFS is like trying to understand what 250 people speaking English, Spanish, Italian, or French are saying in a room.
- In fact, it’s not a surprise. Everything we’ve known about ME/CFS suggests it’s a highly complex, heterogeneous condition. It’s also not alone in its high polygenicity – many other diseases share that.
- Untangling what’s going on in complex, chronic diseases is PrecisionLife’s bread and butter. That is what it was made for, and as we’ll see, it appears to be making good progress in ME/CFS.
- Precisionlife identified 259 candidate core genes that their data shows play major roles in disrupting the biological pathways involved in ME/CFS. The biological pathways in which those genes are most engaged made sense with what we know about ME/CFS. They included neurological dysregulation, inflammation, cellular stress responses, and calcium signaling.
- ME/CFS’s high degree of polygenicity indicates that stratifying ME/CFS patients for clinical trials is essential. Steve Gardner straight out said that “the chances are that most people (with ME/CFS) will not benefit from a clinical trial”. That’s ANY clinical trial. It doesn’t matter what the treatment is. The ME/CFS is simply too genetically heterogeneous.
- One of those biological pathways that appears to play a big role in an ME/CFS subset involves TLR3, which is the target of the drug Ampligen. That suggests that PrecisionLife may be able to identify individuals most likely to benefit from it.
- The PrecisionLife paper identified a drug I’d never heard of called Apremilast that may b be helpful in an ME/CFS subset. Apremilast is particularly interesting because it affects both the innate immune system and neurons and impacts both inflammation and cognition.
- Steve warned, though, not to try Apremilast. Unless you just happen to be in the Apremilast subset – and there’s no way to tell if you are – the odds are that not only will you not benefit, but you’ll be hit with some nasty side-effects. No one, he emphasized, should try this drug.
- PrecisionLife has identified over 40 drugs they believe may be helpful in specific ME/CFS subsets. They’re not releasing this list to the public precisely because they fear people will try the drugs and be hurt by them. They are sharing their data with 8 or so research groups across the world in an attempt to get funding for pilot clinical trials.
- While ME/CFS and long COVID look identical on the surface, PrecisionLife’s genetic analyses suggest that they share about 40% of the same genetic risks. That suggests that while some drugs will probably work in both diseases, other drugs will be disease-specific.
- Recently, PrecisionLife turned its approach on its head. Instead of focusing on people who had ME/CFS, they focused on people they believed were at an increased risk of coming down with ME/CFS but never did. These are people with high levels of the genetic risk factors for ME/CFS, and who were old enough to have been exposed to multiple pathogens over time, yet have remained healthy.
- They’ve been able to identify genes and treatments their data suggests are associated with “disease resilience”. In their disease-mechanism work, PrecisionLife seeks to identify pathological, disease-producing gene mutations and attempts to turn them off with drugs. In the “disease resilience” work, they’re looking for genes they can turn on that will achieve the same purpose – returning the system to health.
- They were able, using their disease-resilience work, to identify an enzyme in ALS that they could turn on, thereby reducing the production of toxic chemicals. That drug is now being used in Japan.
- Please note that Steve is not saying PrecisionLife will solve ME/CFS or long COVID. There is more to these diseases than the genes we are born with. It will take a village to solve these diseases, and he believes PrecisionLife’s work will play “an important part” in doing that.
- The more genetic data PrecisionLife has access to, the better it will do, and we just got some really good news in that area.
- The ambitious Sequence ME and Long COVID project just got a big funding boost (4.2 million pounds/about $6.5 million) from the UK government. This huge effort aims to study the whole genome (3.2 billion base pairs) of 18,000 ME/CFS and long-COVID patients.
- The whole-genome project is to DecodeME’s initial GWAS study what a 1,000-power microscope is to a 10-power microscope. GWAS studies are like surveying a city by mapping its major intersections. WGS studies, on the other hand, map every street, alley, and building in full detail.
- The funding will allow DecodeME and its partners to fully sequence 6,000 ME/CFS patients.
- Producing DecodeME was no easy task, but with its own studies, the help its database has provided to PrecisionLife and surely other research groups, and now with this new funding, DecodeME shows how the impact of large-scale projects that address fundamental aspects of disease can just grow and grow.
- Health Rising will be following PrecisionLife’s work closely. We can expect several papers to be published over the next six months.
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit
Next, they use those biological pathways to identify the mechanisms (enzymes, proteins, specific cell types) that drive them. Then comes a search for repurposed drugs that could impact those mechanisms.
Finally, they identify specific groups of ME/CFS/long-COVID patients who are likely to respond to these drugs, with the goal of enrolling these “super-responders” in “smarter” clinical trials.
The New Study
The first PrecisionLife ME/CFS study was a pilot project. Now they’ve moved into the big time: their new study, “Identification of novel reproducible combinatorial genetic risk factors for myalgic encephalomyelitis in the DecodeME patient cohort and commonalities with long COVID“, used genetic data from a cleaner, more rigorously identified set of patients (DecodeME vs UK Biobank), and it was 8 times larger.
While their first study found 199 SNPs (gene variants/mutations) across 84 gene signatures, which mapped to 14 genes, this study identified 7,555 SNPs and 22,411 disease signatures, which mapped to a whopping 2,311 genes. As Steven said, “That is a lot of signal”.

Steve said deciphering ME/CFS was like trying to understand what 250 people speaking English, French, Spanish and Italian in a room were saying.
In our talk, Steven stated that the 22,411 signatures explain a lot about ME/CFS. These signatures consist of three or more gene variants/mutations, otherwise known as single-nucleotide polymorphisms (SNPS), that appear to predispose people to coming down with ME/CFS.
There are pluses and minuses to that finding. You might think, “Whoa, look at all these genes. This is great!” Actually, it would be easier if only a few disease-altering genes had popped out, giving researchers a clear line of sight. Instead, it appears that thousands of small genetic variants/mutations work together to increase the risk of developing ME/CFS.
That’s not a surprise, though. In fact, it suggests that PrecisionLife is on the right track. The multisystemic and heterogeneous nature of these diseases has long suggested that both ME/CFS and long COVID are likely highly “polygenic” diseases, i.e., diseases in which many small genetic mutations combine to increase the risk of developing them.
High polygenicity is not unusual. The combinatorial process PrecisionLife uses is different, but GWAS studies (genome-wide association studies) indicate that many other diseases (depression, autism, type II diabetes, multiple sclerosis, Alzheimer’s disease, rheumatoid arthritis, asthma, etc. have high polygenicity as well. Six major mechanisms appear to produce Alzheimer’s, for example.
(PrecisionLife was awarded the Innovation Showcase prize for its work on Alzheimer’s at the recent Collaborating for Novel Solutions (CNS) Summit. Check out Steve’s presentation here.)
PrecisionLife’s data indicates what we suspected: ME/CFS is a highly polygenic disease that results, at least in part, from the contributions of thousands of gene variants/mutations.
It does mean, though, that ME/CFS and long COVID are, surprise, surprise, very complex. At first, I wondered if we were too complex, and, indeed, deciphering what the genetics is saying is no small task. Steven said it was comparable to trying to understand 250 English, French, German, and Italian speakers speaking all at once.
While doing so is not a trivial matter, it’s also a solvable problem. The authors of the paper reported that “This is not an insurmountable complexity problem for the study of the disease”.
Steven explained why it makes sense that PrecisionLife is seeing such complexity in these diseases. Some people may have a more viral ME/CFS, others a more autoimmune ME/CFS, and others have a more inflammatory disease.
Within these themes will lie subsets. Inflammation in the brain is going to cause more brain fog; in the gut, it’s going to cause diarrhea and leaky gut; in the lungs, it’s going to cause breathing problems. It’s all inflammation, but each tissue produces a different signal.
Within all those genes lie subsets, and in those subsets, the signal can be pretty clear, hence the author’s assertion:
“It is possible to stratify patients with complex highly polygenic diseases into subtypes characterized by shared disease etiology.”
Understanding what’s happening in complex, chronic diseases like ME/CFS is, of course, what PrecisionLife is all about. They are its reason for being. Steven Gardner did not seem deterred at all.
As we’ll see, PrecisionLife appears to be well on its way to identifying mechanisms, subsets, and possible drugs for ME/CFS.
The Candidate Core Genes
PrecisionLife identified 259 candidate core genes that they believe play major roles in disrupting the biological pathways involved in ME/CFS. They believe that the other roughly 2,000 genes that have popped out are affecting, if I got it right, the expression of the 259 candidate core genes.
Another sign that PrecisionLife is on the right track is that the biological pathways affected by the candidate core genes are well known. The four that stood out in this study were neurological dysregulation, inflammation, cellular stress responses, and calcium signaling. (When they did a hypothesis-driven analysis, energy metabolism jumped out big time.)
Several metabolism-affecting genes (PKM, IGF1R, TBC1D5, and ABCA1) that may influence mitochondrial energy production and glucose metabolism are in the candidate core gene category.
An Ampligen Interlude
Immune-associated core candidate genes included two TLR3-affecting genes. The TLR3 genes stood out because TLR3 can: a) drive inflammation; and b) it’s the pathway that Ampligen, e.g., rintatolimod, works on.
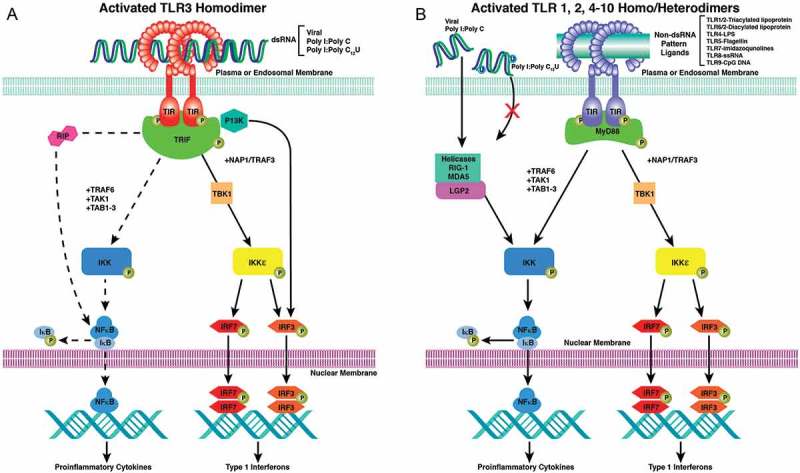
Some candidate core genes highlighted the pathway which Ampligen affects. (Image from “Efficacy of rintatolimod in the treatment of chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME)” Mitchell, 2016)
Ampligen is the only drug to have reached the FDA review stage. The original and only large clinical trial that demonstrated clinical efficacy dates back to 1988. For whatever reason, Hemispherx Biopharma ended the original trial early. That came back to haunt the company (and the ME/CFS community). Lacking a second large trial and citing the early termination of the first trial, the FDA panel, twenty-five years later, when the drug finally came up for review, in a fairly close vote (8-5), rejected Ampligen for ME/CFS.
It wanted another large trial, which Hemispherx Biopharma said it couldn’t begin to fund.
Over time, Hemispherx Biopharma – now AIM Immunotech – has tried the drug on ovarian, breast, colorectal, and pancreatic cancer; Ebola; and long COVID. With its funding levels apparently low – its annual filings included a “going concern” notice – the company badly needs a win and is now focused entirely on pancreatic cancer.
Let’s hope AIM gets its win and can plow some resources back into ME/CFS/long COVID. Note that PrecisionLife may be able to identify “super-responders”; i.e., ME/CFS patients who are more likely to respond positively to the drug – something AIM Immunotech has wanted to find for years.
ME/CFS and Long COVID – More like Kissing Cousins than Sister Diseases?
Maureen Hanson has been suggesting that ME/CFS and long COVID may not be so alike as we think, and, indeed, we’ve seen a few cracks in the ME/CFS/long-COVID unity parade recently. Differences in the amount of clotting, blood vessels, and T-cells, for instance, have been found.
Precisionlife’s analyses suggest the illnesses may be more like kissing cousins than sister diseases. PrecisionLife did note that the “identified overlap between ME and long COVID is perhaps an underestimate”, but even if it is something of an underestimate, the fact that about 60% of the genes that put people at risk for these diseases are different suggests that quite a few differences exist.
Because there’s also substantial genetic overlap (@ 40%), some drugs should be able to treat subsets in both diseases.
Treatments
Another sign that PrecisionLife is right about the high polygenicity of ME/CFS is the poor performance of clinical trials. Gardner straight out said that “the chances are that most people (with ME/CFS) will not benefit from a clinical trial”. That’s ANY clinical trial. It doesn’t matter what the treatment is.
The genetic evidence suggests that targeting the right patients is going to be crucial for producing successful clinical trials.
The genetic data tell him that patients must be stratified for clinical trials to work; i.e., patients likely to benefit from the treatment must be identified first. (It’s no wonder that pharmaceutical companies have kept their distance from ME/CFS.)
That can’t come as a shock to anyone who, after seeing Jane or Joe do better on a particular drug, supplement, or other treatment, failed to get a positive result. That’s probably happened to each of us dozens of times.
Steve was not willing to name names, but noted that drug trials that make biological sense have been proposed for ME/CFS patients, where the dropout rate, even in healthy people, is above 50%. That is, the side effects are so bad that about 50% of healthy people can’t handle them. Without stratifying the patients in an ME/CFS trial of that kind, you’re really rolling the dice in an already very susceptible patient group.
PrecisionLife’s goal is to identify core genes driving the illness and then reduce their expression. From the paper:
“Yet even though it (ME/CFS) is highly polygenic, it would be relatively simple to effectively treat the disease using therapies that reduce expression of the core gene to levels below the disease threshold.”
The paper highlighted a drug called Apremilast, which I’d never heard of. I had the feeling that PrecisionLife would rather not have included this drug in the paper, but it was apparently needed as a kind of demonstration.
PrecisionLife, like other groups I’ve talked to, is concerned that people with ME/CFS will try strong drugs and end up being hurt by them. Steven’s earlier assertion regarding clinical trials applies: unless you just happen to be in the specific subset likely to benefit from a drug, the odds of that drug working are very low, and the odds of side effects are high. Since none of us know which genetic subset(s) we belong to, the odds of success for all of us are low. He said, “Please do not go out and try this drug!”
That said, Apremilast is particularly interesting because it affects both the innate immune system and neurons. It hits a pathway that’s involved in intracellular signaling, and impacts inflammation, immune activation, and ultimately, cognition. This pathway has been, as Steven put it, “well drugged”, and well enough studied, that PrecisionLife is pretty confident that it can pluck out ME/CFS subsets who are likely to respond.
Clinical Trials
PrecisionLife itself does not have the resources to run a clinical trial, but Steven said that PrecisionLife has produced trial designs and is currently in talks with about 8 groups around the world to get them underway. They’re focusing on cheap, easy-to-obtain, generic drugs with long safety records.
Steve cautioned that “it will never be perfect”, that “genetics doesn’t work that way”, but PrecisionLife’s process should help them find more responders to a drug.
PrecisionLife has identified 40 drug candidates it believes will work in specific ME/CFS subsets, but is sharing them only with groups that could run clinical trials.
The partial overlap between ME/CFS and long COVID suggests that some drugs will work in both diseases, while others will only work in a particular ME/CFS or long-COVID subset. At this point, PrecisionLife is most interested in drugs they believe will work in both diseases.
Reverse Engineering ME/CFS and Long COVID

A new approach – finding resilience mechanisms Instead of disease mechanisms – may provide new therapeutic options for ME/CFS.
Recently, PrecisionLife turned its approach on its head. Instead of focusing on people who had ME/CFS, they focused on people they believed were at an increased risk of coming down with ME/CFS but never did. These are people with high levels of the genetic risk factors for ME/CFS, and who were old enough to have been exposed to multiple pathogens over time, yet have remained healthy.
Instead of looking for mechanisms that drive the disease, they looked for “resilience mechanisms” that protect people from developing ME/CFS. Their ultimate goal is to identify and enhance these protective biological pathways in people with ME/CFS.
Thus far, they’ve found “many protective signatures” in ME/CFS that mapped to nine protein-coding genes. Protein-coding genes are arguably the most important genes in our genome because they directly determine the effectiveness of the proteins that orchestrate virtually all the processes in our cells. Only 2% of our genome is made up of protein-coding genes.
Once again, the findings suggested that PrecisionLife was on the right track. The protein-coding genes they found affected processes such as the stress response, autoimmunity, and insulin resistance, which generally align with what we know about ME/CFS.
PrecisionLife has been able to take its resilience search all the way to a drug approval in a neurodegenerative disease called amyotrophic lateral sclerosis (ALS). They found that people with genes that impaired B12 activity were at an increased risk for ALS. Their ALS resilience study, on the other hand, suggested that people with increased activity of a specific enzyme were protected against ALS.
It turned out that that enzyme, in concert with vitamin B12, turns a substance that is toxic to neurons into a safe amino acid. At that, the path became clear – find a drug that stimulates that enzyme so that toxic factors don’t build up. A drug was found and is now helping to slow the progression of ALS in Japan.
PrecisionLife already has a list of drugs they believe will stimulate the resilience processes that are protective in ME/CFS. We should see a paper on this approach come out shortly.
Next Steps
Steve is not saying PrecisionLife will solve ME/CFS or long COVID on its own. Indeed, one would never think that a study of the genes we are born with would provide all the answers. Epigenetic processes, after all, change how our genes are expressed over time. Our general health, the type of environment we live in, the pathogens we encounter, and when we encounter them, are all part of the picture.
Steve said it will take a village to solve these diseases, and he believes PrecisionLife’s work will play “an important part” in doing that.
What PrecisionLife really needs is more good data. The more good data they have, the more precise their models will be. That’s why they’re currently supporting the massive Sequence ME and Long COVID study, which was featured recently in Health Rising.
This ambitious project aims to study the entire genome (3.2 billion base pairs) of 18,000 ME/CFS and long-COVID patients. The whole genome project would be to DecodeME’s initial GWAS study like a 1,000-power microscope is to a 10-power microscope.
Even that is an underestimation. While GWAS samples have ~1–2 million common genetic variants/mutations, WGS captures all 3.2 billion base pairs in our genome. It will pick up rare and structural variants that GWAS can’t.

DecodeME and the ME/CFS community get a big win with funding from the UK government.
GWAS studies are like surveying a city by mapping its major intersections. WGS studies, on the other hand, map every street, alley, and building in full detail.
Getting the WGS sampling done would be a huge win for ME/CFS, and just yesterday, ActionForME reported some good news. The UK government has stepped up big time, contributing 4.75 million pounds ($6.5 million) to the project. The funding will allow DecodeME and partners to fully sequence 6,000 ME/CFS participants. It will take about a year to do the sequencing.
The UK government rightfully touted its horn, stating:
“British scientists are leading the world in genomic research, and this investment puts them at the cutting edge of a challenge that affects hundreds of thousands of people in this country. This first-of-its-kind programme cements the UK’s position at the forefront of global genomic research…”
Next will come getting funding to sequence an equal number of long-COVID patients and healthy controls. Getting the seed money to start the project was critical as it would seem strange for funders to stop funding the project in midstream. Let’s hope the next round of funding goes well. You can register for a webinar about the project here.
Producing DecodeME was no easy task, but with its own studies, the help its database has provided to PrecisionLife and surely other research groups, and now with this new funding, DecodeME shows how the impact of large-scale projects that address fundamental aspects of disease can just grow and grow.



Hi Cort,
would you happen to know whether Steve Gardner could use the “RS” data generated by 23andMe for his genetic decoding?
I don’t know. It’s an interesting idea. I have data from 23andME as well. From what I can tell both DecodeME and 23andME use GWAS testing. It might come down to whether it works logistically to get individuals’ GWAS data vs being able to download it from a large sample set.
Exactly. This is how I find related and possible combinations with Promethease.
I mean; I’m using RS IDs in Promethease to identify possible symptom-related illnesses or combinations of different markers that may include — or help exclude — certain already known conditions.
Hey Cort.
The Gist “read more” button doesn’t seem to be working.
Looking forward to hearing all about PrecisionLife and your enthusiasm for them.
Thanks, Brian! Working on it 🙂
A fantastic interview with Steve Gardner. Wonderful to feel the level of commitment he and his team have to our illness. Thanking the universe that we live in this “era” of science with the combo of WGS and big data analysis offering us hope on the horizon.
There really is a lot of exciting stuff going on 🙂
Thank you for this, Cort, as always. Is there any way you can get a list of the 259 candidate genes, and the B12-related ones? The paper you link to says the data is available for studies. Many of us have had genetic testing and would be glad to compare. I’m
Great question, Carollynn! The paper says the information is available in the extended tables. It also list several supplementary datasets. Usually, you find links to those at the bottom of the text – but I could not find them. This paer is still in preprint status. Hopefully, when it gets fully published we will have those.
I hope you’ll print or link to it when that list is published. Exciting stuff.
Great interview, Cort! I have been on aprémialas for over 10 years. It has completely controlled my psoriasis, which has been a blessing, but sadly my ME/CFS has continued to progress over those same years. There are definitely side effects but the drug manufacturer provides a controlled phase in of the drug to limit them. I hope the drug can work for some ME patients someday!
Thank you for sharing your experiences with Apremilast!
Hi Gayle:
Thank you for the information.
Aprémialas is in Germany known as Apremilast, sold under the brand name Otezla, an oral phosphodiesterase-4 (PDE4) inhibitor used to treat inflammatory diseases. It is approved for moderate to severe plaque psoriasis, psoriatic arthritis, and oral ulcers associated with Behçet’s syndrome.
The active ingredient works by blocking PDE4, thereby preventing the breakdown of cyclic adenosine monophosphate (cAMP), a signaling molecule derived from ATP, inside cells. Increased intracellular cAMP levels help regulate immune activity and reduce inflammation.
I have lived with psoriasis and psoriatic arthritis for 66 years, yet I remain hesitant to take Otezla. The medication carries an extensive list of warnings and precautions issued by the European Medicines Agency (EMA), making the decision far from straightforward.
Elevated levels of cAMP can influence several metabolic pathways. In the liver, cAMP promotes the breakdown of glycogen into glucose (glycogenolysis), which may contribute to increased blood glucose levels and, in some circumstances, hyperglycemia.
@Sieglinde:
“Elevated levels of cAMP can influence several metabolic pathways.”
Indeed. Another important pathway that works more with increased cAMP levels is water removal in the kidneys. https://www.ncbi.nlm.nih.gov/books/NBK373395/
saying “Cyclic AMP (cAMP)-driven mechanisms are central to the pathogenesis of polycystic kidney disease (PKD). Cyclic AMP stimulates both fluid secretion and cell proliferation, making abnormal cAMP-regulated pathways key targets for PKD therapy.”
Note that increased fluid secretion means more problems with low blood volume, a central problem in many cases of ME/CFS and POTS.
Note also that other proposed medications for ME/CFS (Ozempic type weight reducing medications) also act by increasing cAMP. Not the best source but it’ll do; no energy left for in depth search today: https://www.promegaconnections.com/ozempic-semaglutide-for-weight-loss-and-diabetes/
saying “When activated upon binding of GLP-1, the coupled G proteins stimulate adenylate cyclase, increasing production of cyclic AMP (cAMP) from ATP. Increased cAMP stimulates several downstream effects”. Different mechanism to increase cAMP, overlapping / part similar effects.
Note: Ozempic’s potential to reduce blood glucose levels is not in contradiction with “cAMP promotes the breakdown of glycogen into glucose (glycogenolysis), which may contribute to increased blood glucose levels and, in some circumstances”. If / when Ozempic manages to reduce food intake, there will be less glycogen to convert.
@Helen:
cAMP is also an important messenger molecule in the histamine system. The histamine system is a well known player in mast cell related hypersensitivites (MCAS and other).
From https://pmc.ncbi.nlm.nih.gov/articles/PMC1916657/ saying:
“The characteristics of histamine-stimulated adenosine 3′:5′-cyclic monophosphate (cyclic AMP) accumulation in slices of rabbit cerebral cortex have been investigated. The selective H2-receptor antagonists, cimetidine, tiotidine, metiamide and ranitidine appeared to antagonize the stimulation of cyclic AMP accumulation elicited by histamine in a competitive manner consistent with an interaction with histamine H2-receptors.”
Translated in more plain language: histamine elicites / provokes cAMP to accumulate in cells with many H2 (histamine 2) receptors. Thus increasing cAMP via other medication has the potential to make these (mast cells and others) more trigger happy and that in turn risks to increase allergic reactions.
=================
Combined summary:
=================
* Recently severall medications that increase intracellular cAMP have been proposed as ME/CFS drugs. Increased cAMP indeed has a list of potential beneftis for us.
* BUT increasing cAMP also can make hypovolumia (low blood volume) and allergic (and intollerance) reactions more pronounced / worse.
=> part of the solution (more cAMP for more energy) seems to be also part of the problem (more cAMP for lower blood volumes and more allergic reactions).
So it seems to be a thin line of balance that is wrong, not cAMP being either too high or too low.
Worse, most of us have both symptoms of too few cAMP *and* symptoms of too high cAMP. Increasing or decreasing cAMP (especially when done 24/7) hence merely shifts one list of symptoms to another list of symptoms.
@Helen: thanks for pointing out your experience! When reading the side effects of Ampligen it sounded to me like an advertisement for dehydration (low blood volume) and unrecognized allergic / intollerance reactions. Benefit versus side effects: so often a thin and individual boundry 🙁 .
Correction: side effects of Ampligen and Ampremilast (overlapping working mechnanisms) together pictured me those two groups of problems (hypovolemia and increased allergic sensitivity). Made me look into it.
Thanks dejurgen
would you like to read my summary from 2024
Adenosine, Epinephrine, and Adrenaline: Mechanisms of Interaction and Therapeutic Uses
https://swaresearch.blogspot.com/2024/06/adenosine-epinephrine-and-adrenaline.html
Thanks for this. So interesting. I was on Ampligen 26/27 years ago and it took me from completely bed ridden to more mild/moderate. Unfortunately I became allergic to it so had to stop earlier than I should have.
Darn! I wonder if there was something in the formulation?
Apremilast is a sister drug of Ibudilast about which we have talked and heard on and off over the last years.
Ibudilast is an approved drug in Japan and can be orderen via int. online pharmacies. It seems to be used in Japan as a treatment option for ME/CFS – but its hard to get a handle on how well it works.
There is a small 10 person open trial on Ibudilast, some improved…: https://www.amed.go.jp/content/000083247.pdf (there is a summary in English when you scroll down).
A German team has also assessed functional CNS changes in patients taking Ibudilast, however, this is an abstract only and not published (also, they do not report how the patients were doing on the drug – just their brains – grrrr
So in fact we know next to nothing on this class of drugs.
Herbert, you are correct that no one should take Otezla without consideration. After 10 years on it I have solid blood sugar numbers and healthy liver. I’m very happy to have my Ps and PsA under control but would have been thrilled if it also resolved my ME/CFS.
Yes Cort I agree – my favourite ME researcher. I gave a spit sample for DecodeME. It’s brilliant that such innovative progress is being made from those original samples. Well done PrecisionLife.
I like this part…. ‘Steven explained why it makes sense that PrecisionLife is seeing such complexity in these diseases. Some people may have a more viral ME/CFS, others a more autoimmune ME/CFS, and others have a more inflammatory disease.
He went on to say. Within these themes will lie subsets. Inflammation in the brain is going to cause more brain fog; in the gut, it’s going to cause diarrhea and leaky gut; in the lungs, it’s going to cause breathing problems. It’s all inflammation, but each tissue produces a different signal.’
For years many researchers were convinced that all ME patients had a persistent virus. Even though a virus was involved, that theory never felt right for my own ME symptoms and history. I felt really disillusioned with ME research at times. It’s great that someone is now finding a way of subgrouping ME patients.
Subgrouping is the next great challenge. The good news is that some groups are thinking they’ll be able to do this….Let’s hope!
Gut microbiome and Inflammation is being mentioned a lot in relation to ME now. Obviously we want cures, but until they arrive…
In case others are interested
https://www.youtube.com/watch?v=TT5ig1EiIfQ
https://www.youtube.com/watch?v=Z61921PImhc
https://www.youtube.com/watch?v=WndEgsxswiI
Prof Tim Spector was a London rheumatologist for 20 years. He’s now a Prof of Genetic Epidemiology and a leading gut microbiome researcher. These talks are from his ZOE YouTube site.
Can you gradually lower inflammation by eating certain foods? I don’t know, but it seems worth a try. I’m introducing things very gradually.
Thank you Cort for this very interesting article. Perhaps it’s in there and I just missed it, but did Steve give any sort of hint as to how soon effective treatments may be identified through his work?
No he didn’t. They need to get groups to fund clinical trials. So, first, that has to happen. The trials – 30 -50 people – could go pretty quickly, but first they need funding.
“The UK government has stepped up big time, contributing 4.75 million pounds ($6.5 million) to the project. The funding will allow DecodeME and partners to fully sequence 6,000 ME/CFS participants. It will take about a year to do the sequencing.”
And exactly what will this accomplish? Since we don’t know what ME/CFS is, how are they selecting 6000 patients?
I am so tired of hearing that only big bucks will solve this. Balderdash.
The organization I run was instrumental in getting a medication off the market that caused babies to be born with no limbs. We helped a community discover that the increase in cleft palate cases in their community was linked to solvents leaking into their water supply from an unlined landfill. Identified an increase in a rare cranial-facial birth defect in the children of Gulf Veterans (confirmed by a DOD study). One of our scientists was also responsible for getting Dursban off the indoor use market when she found similar birth defects in the children of mothers who were exposed to Dursban during pregnancy. Discovered that a large percentage of children with autism also have some type of structural defect. And much more. You can read all about it at http://www.birthdefects.org
Up to three years ago, all of this was done on a budget of around $100,000 a year.
All birth defects and diseases have a genetic component, but there is not much we can do about our genes. We can, however, look for the triggering agent that causes the gene(s) to express themselves in a birth defect or illness. This can be done for a lot less money and much faster.
A project like our National Birth Defect Registry could give you answers faster and for less costs.
Here’s DecodeME’s criteria. They are a formal ME/CFS diagnosis from a doctor, having to meet either the IACFS or IOM criteria (PEM required), and complete a detailed diagnostic screening questionnaire.
Absent a blood test that’s about as good as you’re going to get. (It’s actually much better than long COVID criteria).
I don’t see any other way to tease out subsets in a large, heterogeneous, symptom-based disease than with big studies.
On the other hand you present such a simpler case. You have clearly defined patients (cleft palate) and a potential environmental toxin which you were able to link to it.
Would that it was so simple in ME/CFS. People are from all over, are exposed to many different toxins, pathogens, and other stressors, at different periods in their lives, and in some cases, there are no identifiable triggering agents.
There is no comparable “birth defect” registry for ME/CFS but that’s what these studies are trying to produce. They’re trying to produce biologically based subsets which can then be targeted. We don’t have a cleft palate or sickle-cell anemia group or genetically based mitochondrial disorder group to target. If we did this would be so much easier. It’s just a big mess.
Given how genetically heterogeneous this disease is that requires a large sample set. Absent that you’re always dealing with small sample sizes which will always include a mix of different kinds of patients. That’s why Gardner asserted that the odds of clinical trials working out are very small.
The whole genome study will make understanding the genetic situation in ME/CFS soooo much clearer.
Ultimately, I believe we will find out that ME/CFS is many different things. I would bet we will end up with different disease names and the ME/CFS label will largely drop away.
Thank you so much for sharing this article!
I just had my genome sequenced through sequencing.com, and I was able to look up some of the gene variants from the related 2022 smaller study publication and get some matches! That’s very exciting, and also very validating that we are not making this up!
As for someone else’s question, I also was not able to find a complete list of all the gene variants that I was hoping to find in the newest article, but hopefully they will publish them.
I appreciate all of your hard work and dedication, I wouldn’t have known about this study because they call chronic fatigue “ME” in the UK. 🙂
ME is a distinct disease caused solely by continuous enterovirus infection of the nervous system. CFS is any of many other encephalitic-causing pathogens and toxins. ME has been known since 1908 and before that used to be called Superior Polio.