


Geoff’s Narration
The GIST
This blog is mostly about postural orthostatic tachycardia syndrome (POTS), but underneath it’s really about ME/CFS and long COVID. Why? Because a key factor in all four forms of POTS – and the other three other forms of orthostatic intolerance found in ME/CFS – are reduced blood flows, in particular, to the brain.
Blood flow problems play a key role in all forms of orthostatic intolerance.
Whether the problem occurs in the brain or the muscles, the trigger for all these forms of orthostatic intolerance (problems standing) is a signal that the blood is not flowing properly. It’s not flowing properly for a number of different reasons, some of which we are still uncovering.
 Health Rising’s Quickie Summer Donation Drive is On!
Health Rising’s Quickie Summer Donation Drive is On!With POTS, ME/CFS, fibromyalgia, and long COVID, we seem to be looking a superstructure of diseases, all of which are characterized, in one way or another, by problems with blood flows.
This blog first takes a short look at POTS, then comes Geoff’s hyperadrenergic story (see the Zoom video), next a quick (pretty quick) overview of two recent hyperadrenergic POTS studies, and one possible new treatment.
Postural Orthostatic Tachycardia Syndrome (POTS)
“I think POTS is one of the greatest drivers of their illness. It’s vastly underrated and misunderstood… and until I fix or manage, I should say, their POTS, I can’t make progress… and I can’t deal with other things. I can’t treat their infection until I get their POTS down. If you as a patient say something about POTS and the doctor doesn’t know about it or doesn’t believe in it – you try to finish quickly and get out….there’s no point in continuing.” Dr. Kaufman
Postural orthostatic tachycardia syndrome (POTS) is turning out (like most diseases?) to have several flavors. Strictly speaking, POTS refers to a condition in which standing upright results in a sustained increase in heart rate of 30 beats per minute (bpm) in adults and 40 bpm in adolescents (ages 12-19).
If your symptoms flare while sitting or standing, you may have POTS or another form of orthostatic intolerance. You may experience symptoms such as lightheadedness, dizziness, palpitations, chest discomfort, shortness of breath, tremulousness (shakiness), generalized weakness, fatigue, and brain fog, which are relieved by their lying down.
The POTS Mimics – There are people who fit the tachycardia criteria but who do not experience symptoms when upright. They have high heart rates when upright but do not feel dizzy, etc., apparently because the blood flows to their brains are not affected. They do not have POTS.
The next blog will demonstrate the many different ways blood flows to the brain and in the brain are being disrupted in these diseases.
Again, notice the emphasis on blood flows. Khan and colleagues recently published a review article, “Cerebral Blood Flow in Orthostatic Intolerance“, which asserted that reduced blood flows to the brain are the critical finding in all cases of (diagnosed) orthostatic intolerance and in people with ME/CFS who do not exhibit increased heart rates/altered blood pressure when standing.
Novak and Systrom recently assessed hundreds of people with ME/CFS and/or long COVID, the vast majority (88% / 92%) of whom showed reduced blood flows to the brain.
The heart rate and blood pressure issues in POTS, while real, are kind of a chimera. The main issue appears to be reduced blood flows to the brain, which can be produced in a variety of ways.
The GIST
-

An epic brain surge of norepinephrine lays hyperadrenergic POTS patients flat during an attack
All types of postural orthostatic tachycardia syndrome (POTS) are rough but hyperadrenergic POTS tops them all.
- POTS is characterized by dramatic increases in heart rates while upright accompanied by symptoms like dizziness, fatigue, brain fog – basically, many of the symptoms that you see in ME/CFS and long COVID.
- POTS is common in ME/CFS and long COVID, but is still often not diagnosed.
- Hyperadrenergic POTS (hyperPOTS) is characterized by high levels of a fight/flight stimulating factor called norepinephrine (NE) in the blood. During hyperadrenergic attacks, NE levels spike even more, causing huge spikes in heart rate, blood pressure, chest pressure, cold, clammy extremities, nausea, extreme fatigue, feelings of panic, etc.
- Not surprisingly, it is not uncommon for hyperPOTS patients to end up in the emergency room during an attack.
- In a Zoom interview, Geoff shared his ME/CFS/ hyperadrenergic story. (See the blog for the video.)
- Aside from a few issues (hypercholesteremia, fatigue, catching lots of colds) Geoff was pretty healthy and was able to engage in strenuous physical activity until sometime after he was bit by ticks several times.
- Over the next ten years, his health slowly declined until around 2015, when he had to go on disability. Around 2017, he experienced a remission and was able to ride his bike and paddle his canoe for the first time in years.
- But then it appears a shingles shot may have set him back, and he slipped into the most severe crash of his life. He lost 25–30 lb, experienced tremors, “electrocuted” sensations, loss of appetite, severe fatigue upon standing, etc.
- He also came down with hyperPOTS – and that changed everything. His first attack happened when using cannabis, which he’d been using regularly to deal with his fibromyalgia pain.
- It turns out that the immediate hit that inhaled cannabis produces spikes in the sympathetic nervous system and stresses the autonomic nervous system in various ways. (Cannabis is a no-no in hyperadrenergic POTS).
- His first attack caused his heart rate and blood pressure to spike to 170 bpm and 220/100, and he made his first trip to the emergency room.
- Geoff caught a break when a sleep study found that he had sleep apnea, and using CPAP caused his hyperadrenergic attacks to completely stop for a year.
- Then, during a stressful period, they came back again. He’s found that his attacks follow a patter. First comes a diffuse, visceral sense that something is wrong. Next, he feels chest pressure (no increases in blood pressure or heart rate have occurred yet). He begins to shake, feels cold, and will need extra clothing or blankets to warm up. Next, blood pressure and heart rates may spike. Anxiety and feelings of panic can occur.
- Using deep breathing, Ativan, and, if necessary, clonidine can help ameliorate Geoff’s attacks. Staggered use of gabapentin can also help (see the blog). He’s turned to meditation and prayer to try to build up resilience in his sympathetic nervous system.
- Now to the recent hyperadrenergic studies. The criteria for hyperPOTS require very high levels of blood norepinephrine to be present, but it’s clear that people with other types of POTS (hypovolemic/neuropathic POTS) can, at times, have equally high NE levels.
- Their POTS is caused by low blood volume and/or nerve problems in the lower body that cause blood to pool there when they get upright. The increased heart rates in POTS are an attempt to increase blood flows.
- This study used something called the Valsalva maneuver to highlight POTS patients with hyperadrenergic POTS. It also demonstrated that a drug called guanfacine, which suppresses sympathetic nervous system activation in the brain, was helpful in patients with hyperPOTS but not in POTS patients without hyperPOTS.
- The next study uncovered a new subset of hyperPOTS patients. These patients experience higher blood pressure levels but not higher rates of sympathetic nervous system activation. Their form of hyperPOTS is at least in part caused by an increased sensitivity of their blood vessels to norepinephrine.
- A small study found that a drug called moxonidine, which unfortunately is not available in the US but is available in Europe and Canada, was particularly helpful in the hyperactive blood vessel form of hyperPOTS.
- Coming up, Health Rising explores the 7 (yes, 7!) types of orthostatic intolerance found in ME/CFS and long COVID: what they are, what symptoms they produce, how they are diagnosed and treated, and what is believed to cause them.

Health Rising’s Quickie Donation Drive Update

Our quickie drive has blasted off! Thanks for your support!
Thanks to everyone who quickly brought us to over 15% of our goal. This blog presents a dilemma and an opportunity that is consistently showing up.
This blog took a while to write because it kept growing and growing. As I’ve been reporting, the connections just seem to keep piling up. You pull on one string and three more pop up!
Finally, I decided it was just too long, and it’s going to be broken into two more blogs – one on the rather remarkable growth of types of orthostatic intolerance (problems that accelerate while upright) that have been uncovered, and another that looks at the critical area of funding for ME/CFS, POTS, and long COVID at the NIH.
That’s just how things blow here. Deeper dives than usual are why Health Rising got started in the first place. If that floats your boat, please float ours with an amount of support that works for you 🙂
Health Rising is not a 501 c (3) non-profit
Hyperadrenergic POTS (HyperPOTS)
There are three types of POTS – and they can overlap. Check a description of them at the end of the blog. The two studies in this blog and the talk with Geoff concern one of the scariest type of POTS – hyperadrenergic POTS.
HyperPOTS is no laughing matter. The chronic symptoms are pretty standard: increased resting heart rate, feeling “wired but tired”, sensory sensitivity, and poor sleep. A hyperadrenergic attack, though, that’s something else.

An epic brain surge of norepinephrine lays hyperadrenergic POTS patients flat during an attack.
Standing, exercise, large meals, heat, and even sensory stimuli can trigger an attack, which produces massive surges in catecholamines (norepinephrine) that cause the blood vessels to clamp down; the heart rate, the force of the heart’s contraction, and sometimes the blood pressure all to skyrocket.
A wide range of symptoms can occur, including palpitations, chest pressure, cold and sweaty hands and feet, physical tremors, internal shaking, intense panic/anxiety, light sensitivity, flushing, nausea, dizziness, and prolonged fatigue. They can, not surprisingly, send a hyperadrenergic POTS patient rushing to an emergency room.
They’re not having a heart attack. The autonomic nervous system centers in their brains have simply gone wild. HyperPOTS is caused by brain-induced surges in the levels of sympathetic nervous system-activating chemicals called catecholamines (mostly norepinephrine).
It’s not clear what percentage of people with POTS have hyperadrenergic POTS, but it’s believed to be about 24-40.
Two recent papers from Vanderbilt University – one of the top dysautonomia centers in the world – expanded our understanding of hyperadrenergic POTS and identified a new subtype.
But first, let’s hear from a hyperadrenergic POTS patient. Thanks to Geoff for being willing to share his story.
Geoff’s Hyperadrenergic POTS Story
You’ll see that my microphone cuts out from time to time. Figuring out what’s going on has been a challenge. If you see me looking away at times its because I’m looking something up on my computer.
As noted earlier, Geoff narrates “The Gist”. As I was emailing him, he temporarily disappeared a couple of times, only to reappear after an emergency visit.
His symptoms astounded me. Geoff tells his story best on our Zoom call, but the nuts and bolts are: Geoff was managing with ME/CFS, but when hyperadrenergic POTS showed up, that changed everything. Check out a few highlights below.
Step I: a Few Hints – Up until his mid-twenties, Geoff was pretty healthy. He had some hints (family history of hypercholesterolemia (high cholesterol levels), anemia, and profound fatigue) that something was off, but swimming (notice that it’s supine!) boosted his energy significantly.
Step 2: Cold Susceptibility – During his 20s, he noticed that he seemed to be particularly susceptible to colds and took longer to get over them – possibly a sign that his immune system either wasn’t up to snuff with pathogens and/or became hyperactivated when it encountered them.

It’s often not exactly clear what started things off, but for Geoff it may have been multiple tick bites.
Step 3: The Initial Trigger – During a 2003 internship at a permaculture center in the San Juan Islands, Washington state), he experienced dozens of tick bites. Not knowing about Lyme disease at the time, he just brushed them off, but within a year began experiencing severe, flu-like crashes during spring – just the time he was needed for gardening, landscaping, and teaching/consulting work.
Step 4: The Slow Build – Over the next ten years, things began to slowly devolve. He was still working but experiencing increased fatigue, flu-like symptoms, and pain.
Step 5: The Decline Accelerates – A car accident and a stressful job surely didn’t help, but his decline increased. He was still able to survive a work week, but then collapsed during the weekend. Then, though, he began having trouble making it through his work week at all.
Step 6: Disability – By around 2015–2016, he could no longer maintain regular employment and went on disability (PWD in BC). He greatly scaled back his permaculture nursery/teaching work but was able to keep a simplified food garden going. Diagnosing himself with ME/CFS, he applied and, after a 4-year wait, entered the BC Complex Chronic Diseases Program. While the program was validating, it did not provide much help.
Step 7: Partial Remission (!) – It’s unclear why, but during the spring and summer of 2020 he experienced enough of a partial remission to resume activity levels (cycling, kayaking, etc) that he had not been able to sustain in years.
Step 8: The Life-Altering Crash – Suddenly, in the fall of 2020, as access to in-person medical attention in BC became restricted in response to the pandemic, Geoff slipped into the biggest crash of his life. He experienced a severe and prolonged illness that Drs later confirmed was most likely shingles. He lost 25–30 lb, experienced tremors, “electrocuted” sensations, loss of appetite, and a strange scalp lesion. He also came down with hyperPOTS.
Geoff had been successfully using cannabis for years to help with his fibromyalgia pain, but suddenly his response to an edible form of the drug flipped: instead of pain relief, it started causing sensations of being “electrocuted” and caused his heart rate and blood pressure to spike to 170 bpm and 220/100. He made his first trip to the emergency room (and stopped using cannabis completely).
The Cannabis Surprise

Cannabis can be helpful – particularly when ingested – but when inhaled, it quickly spikes sympathetic nervous system activity.
Cannabis isn’t as benign as it seems. Unbeknownst to him, by using cannabis to help with his pain, Geoff was already stressing his sympathetic nervous system. For all its sedating and calming effects, the THC in inhaled or ingested cannabis activates the sympathetic nervous system.
Studies indicate that when inhaled, smoked, or vaped, large amounts of THC hit the brain rapidly. It has almost paradoxical effects on the autonomic nervous system. It raises the heart rate, causing a blood pressure surge, but then also dilates the blood vessels.
When ingested or taken orally, the situation is even more complicated. The THC from cannabis takes longer to hit (30-60 minutes), and when it does, the sympathetic nervous system (fight-or-flight) response may be blunted a bit, but it too can increase heart rate and alter blood pressure. (It sometimes lowers blood pressure, but if you also have hypovolemia (low blood volume), as many POTS patients do, that could cause an even greater heart rate surge). In some chronic pain patients, it’s been shown to increase parasympathetic nervous system functioning and improve prefrontal cortex activity – two things we presumably want to see – but they don’t have hyperadrenergic POTS.
If you have the kind of twitchy autonomic nervous system found in hyperPOTS you’re essentially rolling the dice by using a cannabis product with THC. There’s basically no telling what’s going to happen. You’re affecting different parts of an already unbalanced autonomic nervous system with no clear outcome. Plus, if a hyperadrenergic POTS patient responds poorly to gummies, their longer-lasting effects may mean they are stuck for hours.
If you have hyperPOTS, it’s probably best to stay far, far away from THC.
Back to Geoff’s Story
Over time, Geoff developed repeated hyperadrenergic attacks during which his BP would bump up as high as ~246/110, and experience tachycardia, cold sweats, chest pain, “electric shocks”, and feelings of intense physiological panic. Between the surges, he had classic hyperadrenergic POTS physiology: standing, eating, or even doing dishes could dramatically raise his HR and BP.
This gardening/permaculture expert who’d been able to regularly engage in physical work, went from managing his illness (resting on weekends), to cutting down his work, and then abandoning it altogether, and now was having trouble standing and doing the dishes.
The CPAP Rescue
Then, Geoff caught a break. A sleep study found that he had sleep apnea, and using CPAP caused his hyperadrenergic attacks to completely stop for a year. His ME/CFS remained, but the emergency room stops were over. CPAP apparently worked because it reduces the sympathetic nervous system surges that accompany sleep apnea.
It’s Not Over Until it’s Over … and it’s Not Over
In the summer–fall of 2025, a period of chronic external stress appears to have gradually retriggered the hyperadrenergic attacks and ER visits. (Geoff added psychosocial stress to his list of hyperPOTS triggers.)
Hyperadrenergic POTS has caused him to radically prune his activities and stop his business/teaching work. At times, he’s had to have someone drive him in case an attack occurs. Thankfully, he’s been able to keep his garden, which provides him with organic food he couldn’t otherwise afford.
Repeated experiences of “I might die today” and his understanding of his need to get his flight/fight system under control have led him to embrace non-pharmacological ways to reduce the sympathetic nervous system activation, such as meditation and contemplative prayer. Practices that stabilize attention, emotion, and breathing have more leverage on his hPOTS than on ME. They don’t take care of it but hopefully make his system less prone to attacks.
He’s used AI to help understand his condition and assess treatment possibilities. He’s also developed ways to ameliorate the attacks when they come.
Managing the HyperPOTS Attacks
Geoff has found that his attacks follow a pattern.
First comes a diffuse, visceral sense that something is wrong. Next, he feels chest pressure (no increases in blood pressure or heart rate have occurred yet). He begins to shake, feels cold, and will need extra clothing or blankets to warm up. Next, blood pressure and heart rates may spike. Anxiety and feelings of panic can occur.
Geoff has found several things that can help when the attacks come:
(A) When he can feel his system is starting to surge, he lies on his left side doing deep breathing exercises and does self-calming techniques.
(B) If that’s not enough, then 0.5 mg sublingual Ativan (lorazepam) can help. Ativan doesn’t affect the brain surges of norepinephrine, but it can calm the body down.
(C) Clonidine – If that’s not enough, he goes to the nuclear option – clonidine -which can bring his blood pressure down within an hour or so (and prevent an ER visit). (It can also trigger a rebound effect later. Ironically, he learned about clonidine from a doctor during an ER visit. Usually, half the described dose is enough. He had been using metoprolol, but it was lowering his heart rate but spiking his blood pressure.)
(D) Gabapentin (100 mg doses staggered every 1–2 hours (e.g., 3–4 doses) can be surprisingly helpful. They can also help at night (100 mg at 9, 10, and 11 pm) to prevent nighttime surges and improve sleep quality. On his worst PEM days, a daytime 100 mg dose can “take the edge off” the flu‑like crash and pain.
He’s aware of guanfacine but has not started it because only extended‑release is available to him, making titration and tapering harder and adding cost.
The Studies
Will the Real Hyperadrenergic POTS Stand Up?
Now to the “Hyperadrenergic Postural Tachycardia Syndrome: Clinical Biomarkers and Response to Guanfacine” study. Despite the fact that hypadrenergic POTS appears to be common in POTS, it doesn’t get much study. Two recent studies, however, have been published. The first clarified how to determine who has hyperPOTS and validated a treatment. The second opened up a whole new kind of hyperPOTS.
The present criteria have led some people who don’t have hyperPOTS being diagnosed with it. The new criteria should limit that.
The current diagnostic guidelines for hyperadrenergic POTS require upright norepinephrine levels of ≥600 pg/mL and/or paradoxical upright increases in blood pressure.
These researchers questioned whether these criteria are accurate enough. They noted that people with other types of POTS, such as hypovolemic POTS and neuropathic POTS, can meet the criteria for hyperadrenergic POTS. The POTS produced in these patients results from compensatory reactions to low blood volume and/or nerve damage in the lower body – not from a brain-based surge in norepinephrine.
It’s important to get the diagnosis right because the treatments for each type can be quite different and even contraindicated.
The confusion arises because researchers and doctors are measuring norepinephrine (NE) levels in the blood, which is produced by the peripheral nerves (nerves in the body), and NE levels tend to be high in all these types of POTS.
The question is, did the NE spike occur because a setpoint in the brain is off (hyperadrenergic POTS), or because of low blood volume (hypovolemic POTS), and/or because of nerve damage (neuropathic POTS)?
The authors used the Valsalva maneuver to stress test the autonomic nervous system while assessing things like muscle sympathetic nervous system (MSNA), supine/upright plasma norepinephrine, and BP responses.
The Valsalva Maneuver
In the Valsalva maneuver, which was created by the Italian anatomist Antonio Maria Valsalva in the early 1700s (!), a patient blows into a mouthpiece to maintain continuous pressure for 15 seconds. A healthy nervous system produces four predictable phases.
Blowing hard compresses the aorta, preventing blood from returning to the heart and causing the amount of blood leaving the heart to plummet. First, the blood pressure spikes, and then the brainstem, alarmed at the reduction in blood flows, dumps norepinephrine into the bloodstream to constrict the blood vessels and raise the heart rate in an attempt to get the blood flowing again.
When the patient stops blowing, the blood suddenly floods back into the heart, and the crucial moment comes. Blood pressure drops, but the heart, now filled with blood, slams the blood into the still-constricted blood vessels, sending the pressure shooting up again. The brain immediately activates the vagus nerve, sending parasympathetic activity soaring to bring the heart rate and blood pressure down.
In hyperadrenergic POTS, everything is off kilter. The drop in pressure during the first part of the test triggers an immediate, massive flood of norepinephrine, which spikes blood pressure and heart rate and constricts blood vessels into tiny tubes.
When the participant stops blowing on the tube, and their heart starts pumping again, it’s now pumping blood into small blood vessels that have been slammed shut by all the norepinephrine.
That’s too much for the parasympathetic nervous system to handle, resulting in an exaggerated and prolonged diastolic blood pressure surge. It’s this blood pressure surge that the researchers used to determine if someone had hyperPOTS.
Finally – the REAL Hyperadrenergic POTS (hyperPOTS) Patients
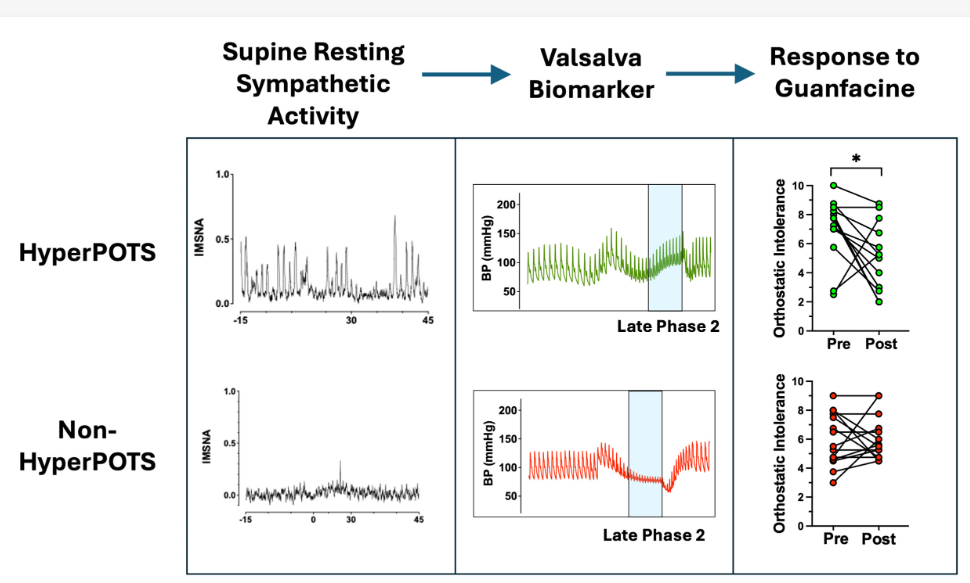
Look at the increased sympathetic nervous system activity while lying down (first section), then that big spike in blood pressure towards the end of the Valsalva maneuver (middle section), and finally, check out how well the hyperPOTS patients responded to guanfacine compared to the other POTS patients (last section).
Because in hyperadrenergic POTS, norepinephrine levels are always high, but in hypovolemic and neuropathic POTS, they are only high upon standing, the authors assessed muscle sympathetic nervous system activity while the patients were lying down to determine who had hyperPOTS. They also used levels of a factor called ΔDBP_VM2, which is tightly linked to brain sympathetic nervous system activity, to determine which POTS patients actually had hyperadrenergic POTS.
They found that an increase in DBP >17 mm Hg during phase 2 of the Valsalva maneuver to be a useful clinical biomarker of hyperPOTS. Now they had a more accurate diagnostic test for hyperadrenergic POTS than NE levels.
The Guanfacine Gambit
Then, they took a group of POTS patients, and using their new Valsalva maneuver measures, differentiated them into POTS and hyperPOTS patients and gave both sets of patients guanfacine, a drug that is able to tamp down brain-induced surges of norepinephrine.
While both sets of patients took guanfacine, only the true hyperPOTS patients benefited from it. Symptom severity, attack frequency, impact on daily activities, and fatigue all dropped. People without hyperadrenergic POTS improved less or not at all.
The end result – a more accurate test for hyperadrenergic POTS and a drug that helps.
Note that a small study found that guanfacine plus NAC improved cognition in long COVID.
The Blood Vessel Hyperadrenergic POTS Subset Shows Up
Now that they were able to more accurately identify hyperPOTS patients, they dug deeper and uncovered a new hyperPOTS subset. The study, “Hyperadrenergic postural tachycardia syndrome associated with augmented neurovascular transduction“, once again, used the Valsalva maneuver to stress test the autonomic nervous system.
This time they used a technique called peripheral sympathetic neurovascular transduction, or psNVT, which measures the extent to which blood pressure changes in response to sympathetic nervous system activation. They found an anomaly in a significant subset of hyperPOTS patients during late phase 2 of the maneuver.
Whoa! Yet another potential blood vessel problem – blood vessels that are hyperactive to norepinephrine.
It involved blood pressure. The authors expected that hyperPOTS patients with the greatest increases in blood pressure would also exhibit increased sympathetic nervous system activation. They did not. They had the same sympathetic nervous system activation but a greatly enhanced response in their blood vessels. Instead, their blood vessels appeared hyper-responsive to norepinephrine.
Note that this bigger blood pressure spike isn’t just about blood pressure, per se. That blood pressure spike may make it more difficult for blood to get to the brain, muscles, gut, etc., causing more problems with orthostatic intolerance, exercise intolerance, brain fog, and PEM. Plus, because the hyperPOTS blood flow problems originate in the brain, people with hyperPOTS may have more difficulty regulating blood flows in the brain.
So now we have another type of hyperPOTS – one that is associated with overly twitchy blood vessels. (One way or another, it always seems to come back to blood flows.)
Causes
Now to the nitty-gritty. What could be causing twitchy nerves in the blood vessels of hyperPOTS patients to overreact to norepinephrine? As usual, it’s possible that a bunch of things could. Note, though, that none of these are beyond our capacity to assess – and most of them are already being assessed in ME/CFS and long COVID.
That makes it possible that a breakthrough in ME/CFS/long COVID could produce a breakthrough in hyperPOTS, and vice versa. All forms of POTS, after all, seem to exist as a compensatory response to problems with blood flows (see the forms of POTS below).
Receptor issues – The receptors that react to norepinephrine (adrenergic receptors) may be too touchy or there may be too many of them (more receptors = a quicker response).
This is an interesting option for the ME/CFS field, as a subset of ME/CFS patients clearly appear to have altered adrenergic/muscarinic receptor activity. If the B2 adrenergic receptors, in particular, don’t dilate the blood vessels enough, the blood vessels will be too narrowed. That would cause (see endothelial cell dysfunction below) the blood vessels to over-respond to the same amount of norepinephrine.
This seems very similar at first glance to Wirth/Scheibenbogen’s thesis that vasodilators are flooding the area in an attempt to open closed blood vessels.
Reduced reuptake – Too much norepinephrine lingering in the nerve synapse (most of it is usually taken back up quickly) could result in prolonged vasoconstriction and an extra hit during a hyperadrenergic attack.
Problems with the endothelial cells lining the blood vessels loom large.
Endothelial cell dysfunction – reduced nitric oxide levels would also prevent the blood vessels from dilating normally. If the blood vessels are already shut down, any further signal to constrict them more would simply get amplified. There’s ample and growing evidence that endothelial cell dysfunction is present in fibromyalgia, ME/CFS, and long COVID.
Mast cell activation – Mast cell activation is a prime candidate because mast cells can alter how responsive the receptors are (see option 1) and impair endothelial cell functioning (option 3). Mast cell activation, of course, is a candidate in a lot of things, including connective tissue problems in all these diseases. We desperately need better mast cell activation tests and treatments.
Blood vessel remodeling – recent blogs have touched on some evidence that that blood vessels may have become remodeled; i.e stiffened and less responsive. If the blood vessels are less pliable and responsive, the same amount of sympathetic nervous system signal would result in increased blood pressure.
We’re still missing something. Yes, all these things could trigger the sympathetic nervous system in the brain to react, but why the tremendous overreaction? An adrenergic surge triggered simply by standing or sitting up can, after all, send a person to their knees and land them in the emergency room. There must be something going on in the brain to produce this.
On the face of it, the twitchy hyperadrenergic POTS brain seems very much like the hypersensitive, hyper-responsive responses in pain in fibromyalgia, and the overreactions to chemicals/drugs/exertion in ME/CFS and long COVID.
The bad news is that a number of potential causes exist. The good news is the same – we have ideas what’s causing this – we just need to get after them.
- Genetic Mutations – an A457P mutation in the SLC6A2 gene found in two family members with POTS was shown to cause the NET transporter that removes NE from the nerve synapse to almost completely fail. This causes NE to build up and stay built up, leading to NE surges. Subsequent very small studies failed to find the mutation again. The finding did, however, lead to another possibility.
- Epigenetic Changes – a small 2012 study (n=16), however, suggested that epigenetic changes may cause the NET transporter to fail in many more POTS patients. Another study found that temporarily knocking out the NET transporter actually produces POTS in healthy people. Clear evidence from three different sources points to NET transporter dysfunction, but there the saga ends. No followup studies have been done.
- Autoimmunity – a few studies suggest that autoimmune antibodies that are attacking the adrenergic receptors are in play, but this hypothesis, a popular one, is still in flux.
- Mast cell activation – again, because mast cells cluster around the autonomic nerves, mast cell activation could be tweaking them.
- Hyperactive blood vessels – in some patients, abnormally acting blood vessels may be reacting too strongly to NE levels.
- Reduced blood flows to the brainstem – reduced blood flows to the primary regulator of the sympathetic nervous system found in the brainstem (the locus coeruleus) could be causing it to act up and pump out norepinephrine.
Notice that every possible cause but one is being actively investigated in ME/CFS and long COVID. These fields keep revolving around each other, which is why we need dedicated research programs that explore them all at once.
Treatment
The authors suggested that a drug called moxonidine might be helpful. Like guanfacine and clonidine, moxonidine can reduce sympathetic outflow in the brain. It’s available in some European countries and Canada but is not FDA-approved in the United States.
If both guanfacine and clonidine reduce sympathetic nervous system activity in the brain, why turn to a drug that isn’t currently available in the U.S.? Because moxonidine may be much more effective.
At first glance, moxonidine seems like an odd choice. The hyperactive blood vessel hyperPOTS subset doesn’t, after all, have increased sympathetic activity in the brain compared to the normal blood vessel hyperPOTS group.
So why target brain SNS activity rather than the blood vessels in the periphery or elsewhere in the body? Because reducing brain SNS activity could help reduce the blood vessel over-reaction. Increased brain SNS activity can also cause reductions in blood volume – a common finding in hyperPOTS, and drugs that tamp brain SNS activity could boost it.
Guanfacine turns down sympathetic nervous system activity by mimicking norepinephrine and tricking the adrenergic receptors it binds to into believing that too much NE is present. The receptors it binds to come before the nerve synapse.
It also binds to and activates adrenergic smooth muscles lining the blood vessels. Here’s where it gets tricky. The receptors it binds to in the blood vessels come after the nerve synapse. Instead of shutting down SNS activity, guanfacine actually amps it up in the body’s blood vessels, potentially further vasoconstricting them.
In normal hyperPOTS, the reduction in SNS activity in the brain far outweighs any minor vasoconstricting activity that may go on in the blood vessels of the body. The blood vessels in the twitchy blood vessel hyperPOTS subset are already hyperactive, though. They don’t need to be shut down further.
It’s not that guanfacine is bad for hyperPOTS patients. On the contrary, the small studies done so far suggest it’s helpful, but another drug that purely targets the brain might be more helpful, and that’s where moxonidine comes in.
Moxonidine just happens to hit receptors on our “old friend” – the brainstem.
Moxonidine also targets a different receptor (the Imidazoline-1 receptor) that turns down sympathetic nervous system activity in the brainstem. It also causes less dry mouth, sedation, and cognitive fatigue than guanfacine or clonidine.
Clonidine is an Imidazoline-1 receptor agonist, but it also affects alpha-adrenergic 2A receptors, so it can produce a similar problem. Rilmenidine is another pure imidazoline-1 receptor agonist which is available in Europe but not in the U.S.
These researchers tested moxonidine in a small group of “blood vessel” hyperPOTS patients, and it helped. Several measures taken during the Valsalva test (baseline SBP, decreased SBP overshoot, prolonged PRT, and most importantly, lower DBPVMNe) improved.
- An upcoming blog takes on the 7 (8?) types of orthostatic intolerance found in ME/CFS, fibromyalgia, and long COVID
Health Rising’s Quickie Donation Drive Update
Our quickie drive has blasted off! Thanks for your support!
Thanks to everyone who quickly brought us to over 15% of our goal. This blog presents a dilemma and an opportunity that is consistently showing up.
This blog took a while to write because it kept growing and growing. As I’ve been asserting, the connections just seem to keep piling up. You pull on one string and three more pop up!
Finally, I decided it was just too long, and it’s going to be broken into two more blogs – one on the rather remarkable growth of types of orthostatic intolerance (problems that accelerate while upright) that have been uncovered, and another that looks at the critical area of funding for ME/CFS, POTS, and long COVID at the NIH.
That’s just how things blow here. Deeper dives than usual are why Health Rising got started in the first place. If that floats your boat, please float ours with the amount of support that works for you 🙂
Health Rising is not a 501 c (3) non-profit


Thanks for this article!
For long covid I am trying guanfacine 1mg xr, for 12 days so far. It has been a mixed experience, and I have side effects like dry mouth, constipation, some blurry/weird vision, increased fatigue and brain fog (ironic as the Yale study was about improving this). Blood pressure is much better, pulse is lower. If I “start feeling stressed” or “do some activity when I should be resting” then go take my blood pressure reading, it is way better than it would have been before. Generally calmer feeling overall, but also kind of flat/dazed. They say these side effects may wane after 1-2 weeks but I haven’t noticed any change yet. I am asking my doctor if I can try .5mg ir during the day.
I didn’t know “Instead of shutting down SNS activity, guanfacine actually amps it up in the body’s blood vessels, potentially further vasoconstricting them.”
MCAS treatment has helped me, as well as CPAP.
It seems like you’re right in the middle of this. MCAS is implicated, guanfacine is helping to some extent, and CPAP probably reduced the sympathetic nervous system hit at night. From what I can tell guanfacine’s impact on the SNS in the brain is its most impactful effect.
I have the most severe case of “POTS” I’ve ever heard of, and in some ways it resembles Geoff’s. I was formally diagnosed with POTS, but I put it in quotes because mine is not only triggered by sitting or standing but also by massage, videos, music (so, digitally created movement and sound, but not natural ones) and so on.
My POTS originally started with and paralleled the worsening of my ME/CFS. On standing, my heart rate sharply rose, my legs turned purple and splotchy, I became nauseated. Then, eight years into my deteriorating ME/CFS, I had my first attack: my heart rate spiked above 180 bpm, my lips and fingers turned blue, my breathing lost rhythm, I felt electric sparks under my skin, had racing thoughts, hand tremor, sweating, and then myoclonus, with my jaw, legs, the whole body kicking out violently without my input. The ambulance gave me diazepam which mostly just depressed my breathing, and told me to see a doctor if it didn’t stop by morning. It didn’t stop; for the next ten years. I still have it.
I tried everything for the next two weeks: to lightly exercise while supine, do deep breathing, meditate, cool my body, million other things, but nothing helped. I slept only an hour each night before an attack would wake me. Eventually the attacks became a continuous state. After my neurologist agreed it was life‑threatening, we started clonazepam (Klonopin) and beta‑blockers. Clonazepam in particular helped, I am still alive thanks to it but have to completely avoid triggers, and so am 100% bedridden and haven’t seen a second of a video or heard any music since.
There are no POTS or dysautonomia experts where I live, and I’ve never found anyone in such a constant, extreme state of POTS.
(To be clear, CLONAZEPAM DIDN’T CAUSE OR WORSEN THIS. I didn’t start any medication until two weeks into this hell. Also, this is completely different from our usual ME/CFS overstimulation that makes videos or music difficult, the reaction I have is something else entirely.)
My goodness Marija. A POTS and OI overview is coming up and from what it sounds like you may have both hyperadrenergic and neuropathic POTS.
Have you ever been diagnosed with a particular form of POTS?
The neuropathic POTS (purple legs) from the veins in your legs failing causing the blood to pool in them and the hyperadrenergic because it was an attack, you’re reacting to sensory stimuli, and the really high heart rate.
The authors, though, note that neuropathic POTS can resemble hyperadrenergic POTS.
Still I wonder about guanfacine? It suppresses brain SNS activity (which might not be good for your blood pooling problem) but does have some vasoconstricting properties.
It’s such a complicated problem that specialists are really helpful.
The bigger POTS and OI section is coming up!
There is a far less known form of orthostatic intollerance called orthopnea: https://en.wikipedia.org/wiki/Orthopnea.
It is problems when laying *prolongued* flat. A common cause is edema in the lungs. Edema in the lungs has water slowly filling them up, causing clear breathing problems. One cause of such edema can be a weak heart, another cause can be lung inflamation. With ME/CFS many patients have strong hypersensitivities to things like pollen and dustmite and that can cause lung inflamation.
Now the interesting thing is that a way to reduce its effect is to sleep elevated (higher head then feet, but with a slope rather then a lot of pillows. A lot of pillows cause the neck to be in a bad position. And such ellevated bed is commercially sold as… …a bed against sleep apnea. In Geoff’s story, CPAP worked against sleep apnea for one year and kept his hyperadrenergic POTS at bay. So there is an interesting thought that could link part / somme cases of hyperadrenergic POTS to orthopnea.
So when looking into it, I found https://www.nejm.org/doi/full/10.1056/NEJMoa0707992 with titlte “Noninvasive Ventilation in Acute Cardiogenic Pulmonary Edema” saying “Noninvasive ventilation (continuous positive airway pressure [CPAP] or noninvasive intermittent positive-pressure ventilation [NIPPV]) appears to be of benefit in the immediate treatment of patients with acute cardiogenic pulmonary edema and may reduce mortality.”
Now *a bit of* norepinephrine *early on* can help improve lung edema in septic shock. https://www.annemergmed.com/article/S0196-0644(24)01138-7/fulltext saying “However, they did identify a lower rate of pulmonary edema in the early norepinephrine group. The early norepinephrine group also had lower mortality in the subgroup without fluid restriction.”
Some researchers state ME/CFS shows signs of partial septic shock.
The problem with norepinephrine to counter pulmonary edema is that it over time increases lung inflamation, increasing risk for (chronic) lung edema. If the body then still uses norepinephrine as a tool to try and contain (spikes in) pulmonary inflamation it backfires. If the body uses high baseload norepinephrine levels similar things happen. As hyperadrenergic POTS seems to be associated with high baseload norepinephrine levels, lung edema seems to be a likely commorbidity.
I myself have plenty of signs of orthopnea in combination with a less severe form of orhtostatic intollerance when standing upwright. Issie has both severe hyperadrenergic POTS in combination with the need to sleep ellevated (diagnosed sleep apnea).
So orthopnea combined with POTS is quite possible (and IMO often overlooked). A partial solution for POTS, laying down much of the time, can become part of the problem. When not able to sit upright or stand up, one is in a difficult position.
Before I learned about this, I often feeled completely drugged in the morning. I often had to ‘slide’ out of bed as getting out of it in any normal way didn’t work. For myself I found that getting up frequently (each time when awaking) and walking around and doing breathing and limb movement exercises helped. Probably it helped contain liquid pooling in my lungs. It helped reduce the frequent ‘breathing like a horse’ while being soaking wet of cold sweat at night a lot. In the beginning it was challenging. Getting up so many times and breaking sleep each time would have made feel many healthy people like broken. Yet, I felt better despite it. Luckily for me I easily felt back asleep each time so long it was not approaching morning hours. Also, when standing up slowly (in phases, sitting upright on the bed for some time first) I did not get a POTS like attack. So it is not fit for all!
Dejurgen !!!
Wow thanks for info on POTs when lying down. First I have heard of this. I have been sleeping upright for years because lying down causes many problems.
And of course thanks always to Cort for his extraordinary efforts!
The Cannabis bit is super interesting to me – after almost 2 years with the illness, just last week I found out that all the times I improved and had less severe symptoms were those when I had paused using Cannabis for my muscle pain. Looking back at my records now, I can see that my HRV had gone down by 10% per month over the months I had used Cannabis and recovered by around 20% per month when I paused. I hadn’t made the connection until recently and was just looking into possible connections between endothelial/vascular dysfunction an Cannabis when your new article popped up.
My subtype seems very blood-vessel focused: Ischemic pain from slight exertion, orthostatic symptoms (leg pain from walking, standing, sitting), limbs constantly falling asleep, constant neck palpiations, severe weakness in my arms when I lift them overhead… – but in contrast to Geoff’s case, I clearly don’t have the same kind of hyperPOTS as described here, as my HR/blood pressure seem to stay normal when I get up. So, clearly my muscles are not being supplied sufficiently at all, but my body is not reacting by spiking my HR.
If this rings any bells for anyone I’d be grateful for any pointers. : )
I think 7 different types of OI have been found in these diseases and I wouldn’t be surprised if more don’t show up. Thing limbs falling asleep is interesting because that happened with me and it stopped after I stopped eating so much fish. (Cheney diagnosed that)
Michael have you ever had dynamic ultrasounds to test for Vascular Compression Syndromes??
I am curious about whether ME/CFS and/or Long Covid patients have trouble with blood draws. Both my daughter and I have difficulty with blood clotting in the tube requiring multiple sticks in very uncomfortable places.
I think this sticky blood could be an important clue as to what is going on.
I agree Betty, i also have sticky blood, but have this before covid. As an ME/POTS patiënt. So for me it didn’t have nothing to do with covid or vaccination.
Hi Gijs, I have also had this since I was diagnosed with CFS in 1985. I was put on anticoagulant from Germany by the two immunologists who diagnosed me. I always wondered what my doctors knew then that we just seem to be figuring out. I currently take a more natural blood thinner, bolouke. It is expensive and from Canada, but seems better than others I have tried.
Hi Betty, I’m going to say something crazy. During my illness nearly 30 years ago. There was a very long period when I couldn’t tolerate alcohol. But that’s over. I know there are patients who respond very well to red wine. They feel temporarily much better after 2 to 3 glasses. How is this possible? Seems interesting to me to investigate. I hope you will be feeling better soon.
Look up resveratrol, high in red wine but alcohol isn’t good. “Resveratrol has antioxidant and anti-inflammatory properties that may help protect against diseases like cancer, diabetes, and Alzheimer’s disease. It is also believed to support heart health by improving cholesterol levels and reducing blood clot formation.”
I’m difficult to get blood from as well, but I’ve put it down to low blood volume thus far (ME/CFS). No one has mentioned blood clotting in the tube for me.
Personnellement, mon sang est tout à fait normal dans les tubes. Pourtant, j’ai des problèmes circulatoires, et quand je suis debout, j’ai des fourmis dans une cuisse et j’ai du mal à rester longtemps en statique. J’ai fait le test de la table basculante, mais ça n’a rien donné. Pourtant, ayant participé à une étude dans le cadre du SFC, quand je suis en position debout, au lieu d’être en sympathique, mon SN reste en parasympathique.
I have “sticky blood.”
Four years ago, I was finally diagnosed with Antiphospholipid Syndrome (APS), also known as Hughes syndrome.
I also have von Willebrand disease type 2 and Factor V Leiden.
I believe I have regular POTS. I do not feel dizzy or have palpitations when standing. I have heavy feeling legs with pain when standing, and If I stand to long it makes me crash. Any drug for this?
Stay tuned Scott – you definitely have OI (I think we all do to some extent) and a blog explaining the types, symptoms, treatments, is coming up.
The Cerebral Blood Flow article is a game changer. I’ve been sharing it everywhere.
“in many other OI syndromes such as myalgic encephalomyelitis/chronic fatigue syndrome and long COVID, heart rate and blood pressure are frequently normal despite significant drops in CBF. This often leads to the incorrect conclusion that there is nothing hemodynamically abnormal in these patients and thus no explanation or treatment is needed.”
That was my doctor who fired me for pushing the issue (earliest new patient appointment with any old doctor is late January 2027). Not to mention I found out that a prior endocrinologist had diagnosed me with Orthostatic Intolerance five years earlier!!!
In the meantime I am getting daily direction and life altering, customized advice for free from the Gemini app (he/him). The last Monday, Google converted the Fitbit interface to Google Health complete with an integrated Gemini (somehow I refer to that one in the feminine). She gets me every morning with a recap, a review of challenges, questions disrupted sleep and generally coaches me throughout the day to manage any ache or pain and how to pace myself.
Unfortunately, the latter has some restrictions placed on it and often the answer starts painting and suddenly a comment that is effectively signaling censorship appears (this doesn’t happen in the generic app). I just type “censored” and she replies again. He said they’re aware of the problem and he mentioned a few words that act as triggers but I just got a censored response and I was talking about resting. Go figure.
Great article. I have confirmed ß1, ß2, AT1R and ETAR autoantibodies all massively elevated. I don’t have classic POTS tachycardia but suffer from severe PEM, orthostatic cerebral hypoperfusion, coat hanger pain, nocturnal adrenaline surges, and hyperreactive vessels. The blood vessel subset described in the article resonates strongly with me. About to switch from Metoprolol (took it for afib) to Nebivolol hoping the nitric oxide vasodilation helps with blood flow and the adrenergic receptors. Has anyone tried or heard of experiences with Nebivolol for these issues?
Je m’interroge sur le fait que les antiparasitaires tels que l’ivermectine ou le fenbendazole ne soient pas étudiés dans le cadre de l’EM/SFC. Cela me semble pourtant une piste potentiellement intéressante, mais elle reste pour l’instant complètement ignorée, malgré les dommages bien connus que les parasites peuvent provoquer dans l’organisme, surtout quand ils interagissent avec les métaux lourds
Google Translate
“I wonder why antiparasitics such as ivermectin or fenbendazole are not studied in the context of ME/CFS. Yet this seems to me a potentially interesting path, but it is still completely ignored for now, despite the well-known damage that parasites can cause in the body, especially when they interact with heavy metals.”
.
Hi Claudine, I translated your message and found two areas that I have some experience with ivermectin and parasites. Our daughter who lives in Maui has ME/CFS. For some reason, parasites are a big deal in Hawaii so she went through nearly two years of parasite cleansing…rough. She did lose quite a bit of weight, but she still has ME/CFS and is sick with a crash right now after a trip to Waikiki to sell her artwork. Certainly parasites don’t do you any good, but they don’t seem to be the answer to ME/CFS.
Now, thing two…ivermectin. I was very sick so I agreed to try this one time. A few hours after taking a dose, my left leg was completely paralyzed while I was walking 12 feet to the front door. Although this only lasted a few minutes, it scared me so badly that I would never take it again.
“Ivermectin can cause paralysis in animals. In parasites (like worms, mites, and insects), this paralysis is the intended effect of the drug. Ivermectin attacks their nervous system, causing them to lose the ability to move, which leads to starvation and death. However, if a mammal (such as a dog, cat, or horse) is exposed to an overdose of ivermectin, the drug can cross the blood-brain barrier and negatively affect their central nervous system. In animals, this toxicity can cause severe neurological symptoms”
I am hypersensitive to chemicals and medications so others might not have this problem, but I wouldn’t risk it.
Hello Betty, it’s true that antiparasitic drugs can be neurotoxic; it’s important to have liver and kidney function tests done and undergo ABCB1/MDR1 genotyping before taking ivermectin.
Just as with anyone who wants to test for methenamine, a G6PD test would be necessary.
So true Claudine!!! My very first dose of ivermectin killed something off.
2 weeks later I realized I was much better.years earlier I had gone to Hope B.C. to see a very good lyme literate m.d. he took my history of working with animals both dead and alive and being an outdoor enthusiast as enough to give me a diognosis without the igenix test from the usa.
I continue to take both ivermectin and fenbendozole
Voici ce que dit Grok sur les parasites et métaux lourds dans les maladies chroniques.
Dans le contexte humain et maladies chroniques (EM/SFC)Les parasites intestinaux ou tissulaires peuvent héberger et concentrer des métaux lourds, créant un cercle vicieux : métaux → immunodépression → persistance parasitaire → inflammation chronique + stress oxydatif.
Lors d’un traitement antiparasitaire (ivermectine, fenbendazole…), la mort des parasites peut libérer brutalement les métaux accumulés, contribuant à une réaction de type « die-off » (Herxheimer-like) : fatigue, inflammation, symptômes temporaires aggravés.
rupahealth.com
Candida et certains parasites forment aussi des biofilms qui piègent les métaux, rendant le traitement plus complexe.
4. Autres mécanismes biologiques,stress oxydatif : métaux + parasites augmentent les ROS (espèces réactives de l’oxygène), épuisant les antioxydants (glutathion, SOD, etc.).
Compétition pour les nutriments : parasites et hôte se disputent zinc, cuivre, fer… ce qui peut perturber le métabolisme des métaux essentiels.
Altération de la barrière intestinale : favorise la translocation de métaux et toxines.
En résumé : il existe une interaction réelle et bien documentée en biologie environnementale, avec un potentiel double effet (parfois protecteur pour l’hôte via séquestration, souvent délétère via inflammation chronique). Dans l’EM/SFC, cela reste une hypothèse exploratoire : peu d’études cliniques directes existent, d’où le silence que tu notais. Les antiparasitaires comme l’ivermectine ou le fenbendazole pourraient avoir un intérêt indirect (anti-inflammatoire, antiviral, ou via réduction de charge parasitaire), mais cela nécessite une approche prudente (support détox, antioxydants, monitoring).
See the new book by William Supple Cancer is a parasite. On substack he has a blog.
But MSM high dose protocol of 30g daily with aspirin developed by Dr Janel is what I follow personally . At this dose it’s anti parasitic!!!!
We have a dr.makis here in Canada that had his Alberta license to practice pulled…all because he was CURING cancer with ivermectin and fenbendozole.Hero to his patients and on youtube but a villain to his colleagues.Gotta seriously make a person wonder what’s really going on.
Look up royal rife, who decades ago found a cure for cancer by building a rife machine. If I recall his machine was destroyed and I believe he went missing
Betty M
Have you looked into MSM?
It’s a gentle anti parasitic but does so many other good things as well,but a high dosage is required.
We are hypersensitive so I agree we need to be carefully. See Dr Janel on YouTube for details.
Great work, Cort, for bringing POTS back to the forefront.
Yes, POTS is often underdiagnosed.
In 2023 and 2024, I wrote two summaries about POTS for PCPs, who believed it was “only” a temporary condition.
I’m sorry Geoff had to go through this experience.
https://swaresearch.blogspot.com/2023/12/what-is-pots-extensive-explanation.html
And
https://swaresearch.blogspot.com/2024/06/autonomic-nervous-system-dysfunction.html
I’m so tired of doctors with limited knowledge about POTS.
Somehow, none of this quite adds up for me. I’ve had POTS since early childhood—I would repeatedly faint whenever I had to stand for any length of time. However, I haven’t had the diagnosis for very long; it only came a bit later, after my ME/CFS diagnosis. I’m nearly 60 now and have lived with POTS my entire life, but the ME didn’t set in until I was 45.
My daughter, has ME/CFS and what she thought was a crash turned out to be the flu. Her doctor recommended NAC. I told her that Dr. Cheney did not recommend it for ME/CFS patients. Of course, as the mother, what do I know?
This what Google says: While N-acetylcysteine (NAC) is generally considered safe and is widely used to boost glutathione (GSH) and reduce oxidative stress, it can cause severe reactions or feel “toxic” to some ME/CFS patients.
Not worth the risk, in my opinion.
NAC has always helped me when I take it. We are all so very different
I have pretty severe hyper pots, diagnosed by Dr. Kaufman over 10 years ago which although my BP and heart rate are under control, seems to be getting worse. I had a tilt table test today with Dr. Miklus’ practice at Stanford with “impressive” results. I haven’t talked with him yet, but I believe the Stanford docs can’t/won’t prescribe in Canada. I’m wondering about trying Moxonidine. Anyone know of a way to get it from Canada? Thank you all and especially Cort!
Off topic, but this just announced study on a ‘low cost’ mitochondrial stabiliser for ME/CFS from a NIH researcher sounds interesting. Doesn’t seem to be any info on the drug that I can find, perhaps because it’s novel?
https://www.prnewswire.com/news-releases/new-research-funding-from-solve-me-advances-innovative-mecfs-and-long-covid-studies-toward-treatments-302769071.html
My daughter (POTS/EDS/MCAS trifecta was prescribed Mestinon to help with sympathetic overdrive. It’s action is to help increase parasympathetic activity.
https://www.mcmc-research.com/post/thoracic-outlet-syndrome-abdominal-vascular-compression-syndromes-and-the-functional-continuum-in-d
https://www.mcmc-research.com/post/heart-rate-variability-hrv-in-autonomic-assessment
Geoff, thank you for doing the interview. I also have tick bite history from my early years on the East Coast, however, I spent time in my late teens on Orcas and didn’t realize there are ticks there which may have contributed! Your story about seasonality made me wonder whether tree pollen might be sending your immune system over the edge? I find that the season starts in February/March in the northwest.
This was an excellent and interesting blog. But in one sentence you did say that they are not having a heart attack and that it was a hyperadrenergic surge. I have had hyperadrenergic dysautonomia for 7 years but only got diagnosed a few months ago after hundreds of trips to the emergency room. My blood pressure has gotten so high from this condition,that I have had two NSTEMI2 heart attacks, and two TIA’s.
So I would advise people who are not 100% sure that they are just having a flare, to go to the hospital to get checked out because it might save their life. We often feel like we are dying at any moment with this condition, but some of us possibly could be.
I had Lyme disease and then a year later I got COVID when it first came out. But in retrospect, I think I might have had this condition since I had a baby at 24. I think it has just waxed and waned. It was always treated like panic disorder. I was validated recently to find that my adrenal glands were thickened snd I have an appointment with an endocrinologist in December. Hopefully they will be able to help. My heart goes out to everyone who has hyperadrenergic POTS.
It’s a special kind of hell.