



I believe my book provides a framework ME/CFS patients can use to support their recovery
(Dan Neuffer, a recovered patient, spent years trying to build a big-picture view of this illness. In this provocative blog he argues that researchers often get too wrapped up in their specialties to see the forest for the trees and that there really is a ‘single’ cause for this illness… and it’s staring everyone in the face. )
After so many decades of ME/CFS & Fibromyalgia Syndrome being described as an enigma by the medical world, I see the day in sight that the mystery will give way for clarity for everyone.
The mystery ended for me personally some years ago, shortly before my recovery, in fact. But we are far from all agreeing what is really going on. There are so many different opinions about these illnesses. Some of these are very strong and are aggressively defended and sometimes it gets very adversarial
Some argue that ME is completely different from CFS. That Fibromyalgia is a different illness than either. Some argue that our illness is caused by epigenetic gene expression, others are sure it’s caused by hypo-methylation, others fight tooth and nail to defend Dr Armand’s theory and the Guai Protocol, then there’s mitochondrial dysfunction, sympathetic nervous system arousal, viruses, natural killer cells…the list goes on and on.

I believe that all these hypotheses, ideas and treatments are actually part of the same big puzzle.
I also think we often miss the forest for the trees. I think our focus on the many symptoms of this disorder leads us (and that includes our researchers) to miss the big picture. I’ll make the provocative assertion that there is very little REAL ME/CFS & Fibromyalgia research going on.
Let me explain…
While there are a huge number of scientists and researchers writing papers and doing investigations on this illness, most look at the illness from one aspect of medicine; the aspect they are specialists in.
And in doing so,I think they tend to disregard other facts and things we know about this illness when they form their hypothesis and conclusions. I think they’re missing something and I actually think, call me bold or naïve, that I, a patient who is a laymen, know what that is.
My Story
My story is probably similar to yours, just with a twist at the ending, which is that I eventually recovered after all those years of suffering.
Probably like you, I could talk about it for hours, but then, you have heard stories just like mine before. Our stories are all different, but they are also all the same. And it was by focussing on the similarities of those afflicted with ME/CFS and Fibro, that I found my answers and consequently my recovery.
So I can summarise my story in a few paragraphs:
I got sick. I ran around to countless doctors who didn’t know what was wrong with me. I developed more and more severe and bizarre symptoms. I ran around to more doctors and every alternative “solution” I could find. I eventually learned that I had ME/CFS. I started to develop severe Fibromyalgia Pain. And then, when I said “things can’t get any worse”, they got a whole lot worse!
When things were at their worst, I was forced to change something. I decided to find answers myself. It was a very slow process at first, as I was bed-bound at that time. But I was not looking for what would make me feel better or what would be a good treatment. Because I had already spent years buying every promise and treatment out there, and frankly I was already pretty cynical, sceptical and perhaps downright jaded at that stage.
All I wanted to know is :
What I Think Causes ME/CFS & Fibromyalgia
Dan believes autonomic nervous system problems play a key role in these diseases.
After my decision to find answers to some hard questions, I spent a lot of time reading Not books about the illness, but basic physiology and biochemistry as well as research papers. My background is not in medical science or biochemistry; it’s in physics, specifically optoelectronics and laser systems. So it was all a whole new language to me. However, over a period of time, by applying some sound logic to what I learned, I believe the mystery of this illness unravelled before my eyes.
The word CAUSE! Sounds simple, but actually needs some consideration.
Consider this:
A boy falls and his arm breaks. What is the Cause?
- The impact on his arm during the fall? (do you stop here?)
- His low bone density that causes his bones to break easily? (do you stop here?)
- The wrong mineral composition that led to low bone density? (do you stop here?)
- The specific reason that led to his poor mineral composition?
And so it is with CFS/ME and Fibromyalgia:
- Yes, low cortisol contributes to fatigue, BUT WHY IS IT LOW?
- Yes, killer cell abnormalities lead to poor immune function, BUT WHY ARE THEY ABNORMAL?
- Yes, inflammation contributes to pain, BUT WHY DO YOU HAVE INFLAMMATION?
- Yes, mitochondrial dysfunction and nutrient deficiencies cause metabolic dysfunction, BUT WHY DO YOU HAVE MITOCHONDRIAL DYSFUNCTION AND NUTRIENT DEFICIENCIES?
- Yes, methylation creates problems with neurotransmitter production and countless other processes, BUT WHY DO YOU HAVE METHYLATION PROBLEMS?
- Yes protein deposits on nerve ‘gates’ may cause fibromyalgia tender points, BUT WHY WOULD WE GET PROTEIN DEPOSITS?
In order to really identify a “CAUSE”, surely we have to look at the ROOT CAUSE. The reason for the problem, the problem that causes ALL OTHER PROBLEMS. The problem that leads to ALL the symptoms.
I recognised that there must be a reason behind this illness. Yes, we are all different, with different stories of how we got ill. With different symptoms. And even with different stories of how we recovered (those of us that do so). But there is still so much in common.
It appeared to me that certain things need to be in place to make sure that “the cause” of this illness was the real McCoy. This is not a perfect list, and I am open for some better criteria, but for me these were a good start:
1. Does it explain the symptoms?
2. Does it explain why certain treatments work?
3. Does it explain why certain treatments don’t work?
4. Does it explain why people recover despite using different treatments?
5. Does it explain how people get sick in the different ways?
6. Does it explain why treatments that work to recover some people, don’t work for others?
7. Is the explanation congruent with the vast majority of the research and people’s experience with the illness?
Because the way I see it, most of the explanations out there of what causes this illness, don’t really stack up when you ask even just a few hard questions. That is not to say they don’t have value. In fact, they are often important pieces of the puzzle in explaining the dynamics of the illness and the symptoms. But nonetheless, I believe that all but ONE are secondary dysfunctions.
The Various Hypotheses: Are They All Right? OR Are They are All Wrong?
I don’t really think that the cause of this illness is a mystery at all (after I completed my hypothesis, I found researchers all over the world that in essence describe large parts of the central theme of my explanation)
The Big Clue
I believe the biggest and most glaringly obvious clue regarding the cause for ME/CFS and Fibromyalgia Syndrome is the almost RIDICULOUSLY LARGE number of problems that occur.
List of Common Symptoms

Are the many symptoms in chronic fatigue syndrome and fibromyalgia our best clue to this disorder?
- severe fatigue
- loss of muscle power
- tenderness or pain in distinct locations on the body (fibromyalgia symptom)
- flu-like symptoms (including tender lymph nodes, muscle aches, sore throat, headaches, nausea)
- gastrointestinal disturbance
- low-grade fever
- depressed immune system leading to recurrent infections (more prominent in CFS & CFIDS)
- mental processing problems often described as ‘brain fog’
- unrefreshing sleep
- inflammation
List of Other Symptoms
Whilst some regard the above list to be the core ME/CFS/FMS symptoms, there are actually many others. These include but are not limited to:
- orthostatic hypotension – when a person’s blood pressure falls as they stand up and momentarily feel dizzy, nauseous, have dimmed vision or numbness and tingling
- the need to urinate, often along with unquenchable thirst
- heart palpitations and chest pains
- muscle twitching described by some people as jolts or flashes
- chills and cold extremities
- allergies
- significant change in weight
- decreased libido
- morning stiffness
- alcohol intolerance
- rashes
List of Psychological CFS Symptoms
- mood swings
- anxiety
- depression
- irritability
- emotional “flattening”
List of More Obscure and Strange CFS Symptoms
- strange smell sensations often described as ammonium
- allodynia – which is when your skin hurts to be touched
- paresthesia – which are sensations such as itching, numbness, tingling, burning or a feeling that something is crawling on you
- hypersensitivity to sound and or light
- profuse sweating
- multiple chemical sensitivities
- electromagnetic hypersensitivity
Given all these symptoms it’s no wonder that some people don’t think this is a real disease.
In my view, there are clearly only possible 2 explanations that really explain ALL these symptoms:
- We are all in a mass conspiracy of COMPLETE hypochondriac insanity (this has been the preferred diagnosis of some doctors for many years) OR
- This illness is a dysfunction of the ONLY system that controls or influences EVERY system in the whole body, the Autonomic Nervous System(ANS)
Now I hope we can all agree to dismiss the first option without discussion.
The Key Player in Chronic Fatigue Syndrome – the Autonomic Nervous System
I make the case that this ANS dysfunction, which can clearly be observed, explains why all the dysfunctions occur, why the different treatments work, why people get sick in such different ways and recover with such different treatments. It explains the symptoms as well as the peculiar commonalities and histories amongst people with this illness. Why?
Because it affects every system in your body. Because it’s involved in pain sensation, it regulates the immune system, heart rate, blood flows to every organ in your body, blood volume, your digestion, the saliva in your mouth, your temperature regulation, your ability to exercise. . Problems like immune dysfunction, oxidative stress, toxic accumulation, cellular dysfunction can all be linked to a dysfunctioning ANS.
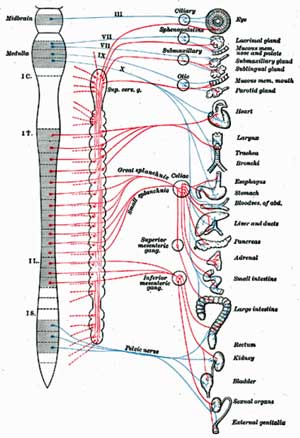
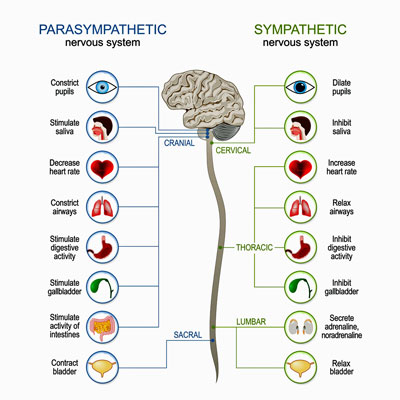
The autonomic nervous system impacts virtually every area of our body
The autonomic nervous system (ANS) is the control station of our body. It affects everything from heart rate, respiration and digestion to perspiration, salivation, urination and pupillary dilation and sexual arousal and it largely functions subconsciously. The main homeostatic regulator in your body; it gets you ready to meet the challenges of the world and then helps you repair your wounds afterwards…and it’s not working the way it should in ME/CFS/FMS.
People often divide it into two subsystems; the parasympathetic nervous system (rest and digest) and the sympathetic nervous system (fight or flight). But the function of the ANS is complex and works both neurologically as well as hormonally.
For example, the ANS dysfunction can be directly linked to the problems of:
- too low cortisol (usually in the morning) or too high cortisol (often at night), as the ANS directly controls these levels via the Hypothalamus and Pituitary glands;
- immune dysfunction, as too much cortisol can halt the maturation of white blood cells and also suppresses the release of the interleukin messengers. It can even shrink the thymus gland and destroy white blood cells;
- excessive pain, as the brain centres dealing with pain perception are directly linked with the limbic brain and the ANS, as well as excessively long term tension and fibrous tissue accumulation in muscles and nerves possibly occurs from overactive sympathetic activation;
- gut dysfunction, because the gut is directly regulated by the ANS which literally can completely stop or flush the digestive system/process;
- neurotransmitter levels which are directly stimulated by the ANS.
But the ANS dysfunction can also be indirectly linked to problems of:
- methylation which can become dysfunctional as a result of excessive oxidative stress through excessive sympathetic arousal, gut dysfunction and the consequent glutathione depletion (a vicious cycle here);
- nutrient deficiencies which result directly from the ANS dysfunction that affects mineral levels via the adrenal axis, but also by the malabsorption due to gut dysfunction.
The list goes on and on. And to make matters more confusing, some of the secondary dysfunctions cause further dysfunctions, some of which can also perpetuate in their own right if not addressed. It becomes messy and confusing.
In my view, this dysfunction of the ANS goes way beyond an overactive sympathetic arousal or a dysfunctional HPA axis that some people suggest. It is a dysfunction and hence not regular or steady in nature and it not only affects many other hormones besides those produced via the adrenal axis; it also is essentially a nervous system dysfunction, so it is neurally mediated.
A Free Copy
If you’d like to learn more about this theory and my recovery you can get a free copy of my book “CFS Unravelled” (over 250 pages) This book has taken me years of research and writing and more hours in front of the computer until the early hours of the morning, than I care to remember. My hope is that it will assist some people in their recovery.
Amazon allows me to make the book free for a number of days and hence it will be Free from the 23rd to 25th of February 2013, right here. It can be read on ANY Kindle device, PC, tablet or other computer device. For a complete list of reading apps – see here.
A Video Explanation
I’ve also produced a 40-minute movie that summarises what I believe is happening in ME/CFS. You can access to it via my website here.
Please realize, that I don’t believe in a single magic pill treatment for all. I offer an explanation that I think fits and a framework which will lead people on their own unique pathways. But I do think that focusing on the ANS dysfunction as opposed to just the secondary problems is critical because in my view, if the ANS dysfunction is not the focus of recovery and is not corrected, then any reduction in symptoms and other bodily dysfunctions will only be temporary. That’s why I speak about the importance of setting goals and creating an action plan.
I’ve recovered using the information and strategies mentioned in this book and I hope others will benefit from what I’ve learned. My hope is that 2013 is the year we all experience personal breakthroughs with chronic fatigue syndrome and fibromyalgia.



Good stuff Dan
Good to see someone thinking outside the box.
I agree with much of what you’ve said although I’ve gone a little further outside the box with my own ‘unified theory’.
You’ve been a little bit of a tease though. To use your own logic – ANS dysfunction is the root cause of ME/CFS and fibromyalgia – but why?
I suspect here may be many ‘whys’ and I guess I’ll have to read the book to find out.
So thanks to you and Amazon for making it freely available for this period!
Ha Ha…Marco – digging a little deeper :)..Good question….What is causing the ANS dysfunction? I imagine that won’t be easy to answer.. For Hornig at the NSU conference it was probably a matter of genetic risk, a window of vulnerability and some environmental insult (pathogen, immune problem, toxin…) – some sort of stressor that hit the system at the right time to shift it in a new direction.
Hi Marco, thanks for the positive comment and thanks for the EXCELLENT question.
THAT is the type of question I think everyone should be asking!
Cort summarises it up well.
Basically I believe that the ANS is overwhelmed by so many stressors of various types such as toxic exposure, physical trauma, infection, psychological stress etc. (usually multiple stressors – ie. the perfect storm), that it has to react SO strongly, that the overreaction in itself becomes a stressor.
This overreaction of the sympathetic nervous system then, over time, gets countered by overactive parasympathetic reaction in an attempt to minimise the damage. But both states are out of balance and as the system flip-flops from one extreme to the other, the problem widens with secondary dysfunctions that perpetuate in their own right (I feel this is often where we lose sight of the real problem).
I think we tend to dig TOO DEEP for answers looking for other factors (ie. something that is broken). In my view the answer is more obvious than that. Whilst I agree that there are pre-disposing factors, I believe that the illness is actually a valiant attempt by the nervous system to deal with an overwhelming and continuing amount of stress.
But it is much more than just about stress avoidance or reduction (remember the parasympathetic dominance, too much of a good thing!), it is about rewiring for appropriate regulation. Based on my own experience and on recent research by Harvard into brain plasticity beyond childhood, I believe it to be possible to reverse this dysfunction. Trying to consciously take over a subconscious function can be helpful to some extent, but in the end the ANS has to function AUTONOMICALLY.
I’m very ill and can read only In short amounts and crash if it is anything more than light reading. I’ve skim read your book as it’s all I can manage. am I right that as well as diet to maintain steady blood sugar levels your primary method of rewiring the brain/ans was meditation? Many thanks
Hi Annie. I totally understand the challenge of reading. My hope was always to create a video series, but it has just not been affordable. Hopefully I can make a resource available like that in the future somehow.
Whilst I have created the free 40 minute video explanation summary, it doesn’t really replace the book. So I suggest that rather than skimming (you will miss the bigger picture doing this, it will just look like all the other stuff you have read before!), read it carefully and in small chunks. Don’t push yourself, take your time.
Diet and meditation are surprisingly hepful and an important part of the overall process in my opinion. However, as some of the people here have pointed out, that alone often won’t work for people. (but it is possible, I know some who have succeeded this way).
Instead, you need to get your head around the whole concept, and then explore your own triggers and address these. The book points out the different areas to investigate. Many people tell me a “light bulb” goes off and they see where they have to focus their attention and efforts. I also recommend that you then get the appropriate help where necessary.
I am sorry not be able to give you a simpler solution, but that unfortunately is the nature of the illness. We need tailored approaches, despite the fact that many powerful strategies can be shared by virtually all people. But unless you address that trigger that is holding you back, your progress can be frustrated.
Good luck – 🙂
Thanks Dan
How wonderful if you would provide an audio version of the book. That would meet Annie’s need as well as numerous others. So very excited to consume the information you are providing…..going to read today. Thank you!
In responding to the comment of unable to read, this is my suggestion: Try using Microsoft Narrator. I have trouble reading books due to falling asleep. I was able to use the narrator and have the book read to me while I was driving, doing housework, etc. I need to listen to the book again, but I got most of the information. I had the book read within a week. That is a record for me!
Great idea. Never heard of MS Narrator before. Thanks 🙂
What a great idea Laura, very clever. I followed this up and found that I had to Kindle for PC with Accessibility Plugin here:
http://www.amazon.com/gp/feature.html?ie=UTF8&docId=1000632481
Once I installed this, and turned on the Narrator (in a Programs/Accessories/Accessibility), then I just had to press CTRL + R and it read in an excellent female voice.
Thank you so much Laura, reading can be difficult, so I think this is an excellent resource.
Dan
Thank you for making your book available through Amazon without cost! As a person who has had MECFS for 38 years, I look forward to finding answers in your book and will read it with great anticipation.
Sincerely,
Nita
Hi Nita…I haven’t read the book either but my gut (ouch) intuition is that Dan is on the right track. I look forward to reading it as well.
Very interesting article – thanks Dan. And with which I much agree. It always struck me on PR that we all suffer the same symptoms in varying degrees and I recall asking my GP (after various specialised investigations) – is there anyone who would consider them all with no luck whatsoever- in the end resorting to leaving areas out outside their field.Still feel whatever sets the chain of events into motion would be a great find.
Dan,
I absolutely agree with you and thank you for your generous sharing of experience, knowledge and hope.
As most of become unwilling experts at the various biochemical mechanisms in our body and the ensuing dysfunction that occurs, we naturally begin to accumulate an understanding of anatomy and physiology in an effort to help ourselves navigate the gauntlet of medical decisions we have to make on our own behalf.
I, too, have seen the ANS connection and am currently exploring theories of viral inflammation of this core system in our bodies. I look forward to reading your book—thank you!
Thanks for your comment, I hope you enjoy the book.
The point I make (as per above reply to Marco), is that we are looking too deep sometimes for an external causal factor.
I am suggesting that things are not necessarily “broken” due to something, but instead are just not working correctly. (REALLY not correctly, and for a long time!)
I’ve thought for a long time that concentrating on secondary dysfunctions is less useful that finding the primary one. I’ll read the book with interest.
The book is also available for free on Amazon.co.uk at the moment.
As regards the location: Wyller believes the locus of ME/CFS is the brainstem – which regulates ANS functioning and can induce hypersensitivity by overwhelming the upper control regions of the brain. Here’s from Wikipedia on the brainstem
Studies suggest that the HPA axis problems probably originate in the hypothalamus, which is regulated by the brainstem, not the adrenal gland…
If I remember correctly, the Lights believe (I think) that an infection of peripheral ganglia – another important ANS regulatory area, I believe – plays a role.
And there’s the enteric nervous system – which is almost it’s own branch of the autonomic nervous system..
There are lots of possible connections.
Wikipedia has a good article on the ANS
Thank you for making the book available for free!
Can anyone help me with a practical issue? I’ve “bought” it at Amazon, but I can’t make it download to my Kindle for PC on my actual computer – it ends up in the Kindle Cloud online at Amazon. How do I go about downloading it to my PC?
Hmmm…Here some suggestions from an email Dan sent out.. I remember when I downloaded it on my computer I used a kindle app to do that.
The book can be read on ANY computer device, so don’t worry if you don’t have a Kindle. In fact, you can even read Kindle books online using a cloud reader. You can download reading apps for free from Amazon HERE.
1.) You buy it using “one-click” on your Amazon Account
2.) Deliver it to your “kindle on PC” or other reader.
3.) Open the Kindle App program and enter your Amazon account details under TOOLS – OPTIONS – REGISTRATION
4.) “SYNC” it by clicking TOOLS – SYNC AND CHECK FOR NEW ITEMS
Hope that helps. If you get stuck you can check out Amazon Help Here:
http://www.amazon.com/gp/help/customer/display.html/ref=hp_left_ac?ie=UTF8&nodeId=200783640
Hi, Anne. I downloaded it last night to my pc and phone. Had a few probs, but finally got there.
You may have to uninstall and reinstall the Kindle app on your pc, or you may need to go into your “Orders” and try and manually download it, or both.
Good luck!
CJ
Within your Amazon account you can find your order of the book and then “deliver” it to the various devices (ie. Kindle on PC) – I think it was under actions – 🙂
Hi,
For years now I’ve thought that my problems lie in my ANS. Now there is a book that claims to explain this and I can’t get it because I don’t live in the States. What a bummer. I’m far past expecting miracle cures but am interested in anything that anyone has found that may help.
So close and yet so far away. Any suggestions?
Kathryn
I’m sure a way can be found to get it to you…
Kathryn, the book is available ALL OVER THE WORLD – just look the Amazon you are supposed to use in your country and download there, here are few more links:
Here are some additional download links:
US Amazon: http://www.amazon.com/dp/B00B3OCVGI
UK Amazon : http://www.amazon.co.uk/dp/B00B3OCVGI
Canada Amazo : http://www.amazon.ca/dp/B00B3OCVGI/
Deutschland Amazon: http://www.amazon.de/dp/B00B3OCVGI
France Amazon: http://www.amazon.fr/dp/B00B3OCVGI/
Italia Amazon: http://www.amazon.it/k/dp/B00B3OCVGI
España Amazon: http://www.amazon.es/dp/B00B3OCVGI
I believe some countries need to use certain Amazon pages:
Republic of Ireland : use US Amazon instead of UK
Australia, NZ & India: use the US Amazon
More instructions on my facebook page here : http://www.facebook.com/cfsunravelled
Yes! Yes! Yes! This resonates so greatly.
Thank you Dan for such insightful learning and finding your way through an illness that leaves us feeling so vulnerable. This learning and insight you have gained is a gift to all of us suffering with CFS/ME.
Thank you Cort for posting this and the whole website.
I agree that what causes ANS dysfunction is a “perfect storm” of genetic predisposition and trauma ( environmental, infectious, emotional) that seems to engage the development of this disease.
I have been housebound since Oct. 2011. I am just starting to recover through my own learning. I am a visual artist who is now just starting to work again. I think if I can add anything to Dan’s and Corts fresh perspective it would be that I am starting to observe the way my brain works (functionally). It is a creative brain that tends to overwork by looking at all sides of any issue. I suspect that fellow Fibromyalgia, CFS/ME sufferers are “deep” thinkers who have a tendency to overburden their brain.
Thanks again,
Betty
Your comment ” I suspect that fellow Fibromyalgia, CFS/ME sufferers are “deep” thinkers who have a tendency to overburden their brain.” is interesting fore every person to consider.
It appears that there are a couple of distinct personality profiles within the CFS/Fibro population. I find they are often extremely driven and/or caring people. This may be a contributing factor to coming into a position of overwhelming stress.
Although obviously, if you move into a ‘toxic home’, have pesticide exposure or a car accident or immunisation this may be less relevant.
Just want to make sure everyone who is trying to understand these body systems is aware of Khan Academy. Thanks to that great organization, I’m familiar with ATP production, Krebs Cycle, mitochondria cells and their function. It’s a terrific resource, and very friendly to PWCs. The videos are usually about 10 minutes in length.
You can find them under “Biology” at http://www.khanacademy.org
Best,
CJ
Hi again,
On the Canadian website it says that the book is not available in my country. When I saw this I called Amazon and she confirmed this. That’s when I posted my plea for help here.
Then I went back to the Canadian site and clicked on the right hand button that asks that the book be downloaded just to see what would happen and lo and behold it downloaded. Don’t understand it but am just happy it worked.
Am looking forward to reading the book now. Thanks for responding.
Hi.
I’m in Canada and this is the 3rd Kindle book that I’ve downloaded (to PC) from Amazon.com without problems.
The first one was a couple of months ago.
Not sure why you’ve been told otherwise…Sue
Amazon often wants people to use a specific site. I spent a long time trying to help a gentleman in Republic of Ireland (as opposed to norther ireland) who couldn’t get the book. He was using the UK site and should have been using the US site, who would have thought!
I too think Dan is generally correct in his theory of ANS dysfunction, although I believe that that begins in the gut, which is basically a huge part of the ANS after all…
There’s more and more interest in the gut all the time….Mady Hornig has a scenario in which gut issues result in autism or CFS or other disorders and Dr. Chia often traces back enteroviral infections to the gastrointestinal issues. (Remember the 80% positive rate on his gastrointestinal biopsies?) Who knows? My gut problems were not that noticeable but they’ve really got worse over time…(Oddly enough I’m feeling better in other ways…(lol))
Check out Christine’s experience seeing Dr. Chia here – http://www.cortjohnson.org/blog/2013/02/23/me-and-dr-chia-chronic-fatigue-syndrome/
Just skimming through the book (THANK YOU DAN), I think I may have been correct — he says a few months after the shock/trauma of his wife’s difficult pregnancy, he “collapsed with severe intestinal distress”.
Maybe I should join the Psychic Club Network? 🙂
Just switched through the book: Please not another story of CFS being an “ANS dysfunction”, mainly affecting the amygdala – of course through unconscious stress. This is nothing different than the Gupta theory. So the answer is just that easy? stress reduction, swichting off television, meditating and of course eating a “healthy diet” and doing the right supplements? Sorry, but these sort of things counteract every adcocay we are doing for finding treatments and markers. Why, for example, would Rituxan work for 67 percent in a RCT when the Neuffers and Guptas were right and its just stress? I don’t think things like this wil help our cause…
I don’t if that’s the ‘easy’ answer and I can’t imagine that’s all it is…If every one could fix their ME/CFS with Amygdala Retraining I think we’d all know that and be dancing in the streets..That doesn’t mean some people haven’t had real success that way but look at Dr .Chia; he has pretty good ‘success’ rates; ie improvement rates (check out Christine’s visit with him – http://www.cortjohnson.org/blog/2013/02/23/me-and-dr-chia-chronic-fatigue-syndrome/ ) and he’s doing something far different.
This is a heterogeneous disorder….Will it all fit under the autonomic nervous system? Hopefully we’ll find out.
I have the same sentiments as Caroline, but I have realized that Cort has a different opinion and as much as we get frustrated by our differences (I certainly do), I do still hope we are able to find a way to agree on some, but few, overall principles on how to advocate for our sake…
Cort say it is heterogenous disorder, I personally think that a large group of us have one unique and homogenous disorder as defined by the CCC (of which under 10% ever recover fully from), but I agree with Cort that there are patients out there with ME/CFS diagnosis that does not fit that bill. At the same time, I do not see any conflict between Dr. Chia´s results and the Rituximab results; the immune and nervous system are immensely complex and there will certainly be more than one treatment option for people with the same disease…there are multiple drugs for MS, cancer etc.
Cort, I tried to send you a friendly email, but got an error message, could you check if you got it…?
Sorry Lars I appreciate the nice email but I don’t think I got it..
I agree that its common to have a variety of approaches for one disorder. Look at cancer – there are some drugs that work better for a specific cancer but it appears there are usually a variety of drugs to choose from – and cancers are very well defined (!). How much more does it make sense that various drugs/approaches would work better in some ME/CFS vs the others.
Good point on Dr. Chia and to further it – he’s using an herbal preparation that’s probably effecting multiple parts of the immune system; he’s using it for enteroviruses but there’s no telling what else its affecting..I hadn’t thought of that before.
Cort,
Tried sending the email it again through the website. Let me know…
Caroline and Lars, thanks so much for raising your concerns, I do see where you are coming from and agree that any explanation should stand up to the hard questions!
You are right about the similarity, but the “Gupta theory” has actually been around for much longer than either of his or my ‘discovery’. So your scepticism certainly isn’t new.
I personally believe that Ashok’s work is very good, and also that his method works for many (but perhaps not all) people. But as it works for some, I hope you might agree, that this would be significant or at least interesting.
However, the answer is NOT just stress reduction as you describe it, because whilst that works for some people, clearly it does not work for all.
Because the stressors you mention are just one form of stress. It doesn’t address the immune dysfunction that you mention with the drug study or all the other stressors I mention in CFS Unravelled.
The stressors are complex and varied, which is why part of the reason why we are a heterogenous group. That is why I believe that people must tailor their recovery strategy to their own experience, which can be tricky to do on your own.
The reason why different drugs and treatments work on people with CFS/Fibro, is because we suffer a variety of dysfunctions that benefit from these treatments.
However, the view that I am trying to put forward is that the ANS dysfunction is the underlying reason and hence needs to be addressed. But I do appreciate that the solution is not unilateral or as simple as reducing the obvious mental stress in our lives. (wouldn’t that be nice!) – 🙂
You obviously didn’t read much of the book at all. He doesn’t say it’s “just stress”. Gupta isn’t mentioned at all. And surprisingly, the amygdala isn’t mentioned as much as other parts of the brain.
Also very important — he talks about psych stress versus physiological stress (which includes vaccines, chemical exposure, viruses, bacteria, etc.).
Perhaps if you’d actually read a little more of it, you wouldn’t make such hasty and erroneous judgments?
Sorry — my reply was for Caroline.
I’m right there with you, Caroline. I just read every word of the book, and it’s basically a verbose version of the amygdala retraining theory, with some fairly nonspecific padding about diet, exercise, and supplements. I was quite disappointed, in fact, more than disappointed. I was appalled. I’m glad it cost $0.00, or I’d be seeking a refund! If I read one more word about “over-vigilance” in an illness that is best managed through very careful vigilance–and which deals its worst blows when we are under-vigilant–I will scream.
Two things – one of which involves a twist 🙂
One – the idea of hyper-vigilance is that our systems (not ourselves) are over-vigilant, too-turned on–always on alert…and that’s wearing us out…the goal would be, if you have this problem and you may not, is to turn that vigilance down.
Two – I agree that at least I am too under-vigilant; I work too hard, I don’t take enough breaks, don’t eat the right things all the time…and I think Dan, from the descriptions of the book I’ve seen, would agree with that…and probably add some more things to be vigilant about such as stressful thoughts and anything else that stresses your system.
I would love to find something that would turn that arousal off; I’m convinced that one day we will have something that will torpedo it at its source…
I appreciate your attempt at a solution and I agree that the ANS seems dysfunctional. However, I must say I am not a fan of your approach. From what I read in your book, it sounds like the same old psychosomatic blame-the-patient argument. You say:
“IN SUMMARY ·
The ANS dysfunction is the inappropriate and ongoing stress response to a variety of triggers;
· The four main causes of the ANS dysfunction to be addressed are:
1. Conscious and Subconscious Stress and Concern about the illness and symptoms of CFS;
2. Subconscious stress due to bodily dysfunctions (poor blood sugar regulation, toxic stress, hormonal dysfunction etc.etc.)
3. Conscious and Subconscious mental and emotional stress experienced in your current environment;
4. Conscious and Subconscious mental and emotional stress experienced in your past;
A 5th cause is the ANS dysfunction itself. To overcome this you need to:
1. Become aware of inappropriate stress reactions and interrupt these patterns;
2. Reduce you base level of arousal;
Things helpful to reduce your general arousal levels are: § Meditating daily; § Going for leisurely walks in nature; § Listening to music; § Reading a relaxing book; § Avoiding stimulating activities like exciting movies or music.”
Much of that sounds like psychology nonsense. As a psychotherapist myself, I agree that good mental/spiritual health practices (along with physical health management) can be tremendously helpful to support a person who is living with a chronic illness, to keep it from taking over their life. Especially for someone who has not incorporated these things into their life, they might find significant relief.
But it is not a cure.
Personally, I do my own version of your plan, as most PWC’s probably do. We all need to address multiple symptoms and systems.
I am lucky to be fairly functional. I work, go out, spend time with family, etc. But there is no amount of turning off the television or meditating that is going to allow me to hike up a mountain or go dancing.
I wish it were that easy.
I get that this doesn’t apply to you; and it isn’t enough but I don’t get the ‘blame the patient” part. If the ANS system is problematic why not find ways to turn it down? If you have heart problems you find ways to destress the system using relaxation exercises; if you have asthma the same thing applies….
HRV studies invariably show increased flight/fight response in ME/CFS and studies have shown that different meditative techniques can change heart rate variability patterns. You have a physiological measurement – it can change in some people using some techniques…
For instance here’s evidence of autonomic nervous system problems in asthma
It looks like heart rate variability problems are found in asthma as well as ME/CFS except that they’re the opposite…asthma patients have reduced fight/flight and increased ‘rest and digest’
http://www.ncbi.nlm.nih.gov/pubmed/22919165
and here’s a study showing that mindfulness based stress reduction (MBSR) therapies, the same type of stuff I assume Dan is talking about, do help in asthma
Thorax. 2012 Sep;67(9):769-76. doi: 10.1136/thoraxjnl-2011-200253. Epub 2012 Apr 27.
Effect of mindfulness training on asthma quality of life and lung function: a randomised controlled trial.
Pbert L, Madison JM, Druker S, Olendzki N, Magner R, Reed G, Allison J, Carmody J.
RESULTS:
At 12 months MBSR resulted in clinically significant improvements from baseline in quality of life (differential change in Asthma Quality of Life Questionnaire score for MBSR vs control: 0.66 (95% CI 0.30 to 1.03; p<0.001)) but not in lung function (morning PEF, PEF variability and forced expiratory volume in 1 s). MBSR also resulted in clinically significant improvements in perceived stress (differential change in PSS score for MBSR vs control: -4.5 (95% CI -7.1 to -1.9; p=0.001)). There was no significant difference (p=0.301) in percentage of patients in MBSR with well controlled asthma (7.3% at baseline to 19.4%) compared with the control condition (7.5% at baseline to 7.9%).
CONCLUSIONS:
MBSR produced lasting and clinically significant improvements in asthma-related quality of life and stress in patients with persistent asthma, without improvements in lung function.
http://www.ncbi.nlm.nih.gov/pubmed/22544892
As another recovered patient, I have to agree with Dan that the stress system does seem to be the main culprit. I slightly disagree with him in what perpetuates the illness…I think it is more likely that the stress simply causes changes in the brain that need to be reversed before the patient can recover. I agree with Laura that no amount of relaxation will result in recovery once you have full-blown CFS – that didn’t work for me, and it didn’t seem to work for Dan either.
I’m also not sure why you call it “psychology nonsense”. A Lot of research has been done on the effects of stress, and many of the systems such as the HPA axis and autonomic nervous system are very well understood. All of the symptoms and signs of CFS seem to typical of a dysfunctional stress system. It’s certainly possible that CFS is caused by a virus, but the research at the moment seems to be pointing towards the stress system as the most likely cause. That is also my experience from being a recovered patient, and talking to other patients who have recovered.
I actually agree with you, in fact research has clearly shown these changes to be the case by using just basic MRI investigations.
What I hope to convey is that the stressors perpetuate the illness in the sense that they don’t allow the dysfunction to reverse. Think of it like continuously picking a scab that then never heals. But because the scab is itchy, you just can’t help yourself.
Fcp, you write that no amount of relaxation was enough for you to make a recovery. May I ask which approaches you did that you believe led to your recovery? Many thanks
Dan doesn’t say that the illness is psychosomatic. Although Dan doesn’t use it, I believe the term neurosomatic that Dr Goldstein coined would be more accurate. Dan’s theory is very similar to the one described in Betrayal By The Brain, except that he’s taken a bigger-picture view and the treatment is much more accessible. It does require taking responsibility for your illness though, rather than expecting a doctor to cure you.
Laura, I find it disturbing to hear a psychotherapist equate “psychosomatic” with “blame the patient”. Surely you of all people should be aware of the subconscious power of the mind to create dysfunction of all types in a person’s life.
Unimpressed, Graham
‘it does requiring taking responsibility for your illness’. Well, Graham, I am mightily unimpressed with such a sentence. I know many people with this illness, they spend all their time, finances and limited energy resources trying to get better – and, no, not just popping pills from the doc. I find your above comment judgemental and arrogant in the extreme.
In my brain fog I meant to say people try so many things to get better and yet they don’t work time and time again.
I hear that the thought of taking responsibility for your illness causes strong reaction for you. I find taking greater responsibility in challenging situations and learning to accept reality however painfully triggered I may be by it, reduces the stress I feel. Cheers, Graham
Hi Annie. I don’t think Graham meant offence. We have all experienced EXACTLY what you are talking about. I think he meant that the road to recovery is more complex than just accepting a treatment that leads to a cure (because this doesn’t exist).
So we have to do a variety of things and because I suggest a multi-lateral approach that includes help from medical professionals but also making big lifestyle changes including some mental disciplines during the recovery period, a lot falls back on us.
So it isn’t about blame, but rather about empowerment. But it is only empowering if we believe we know what we need to do to move forward. This is obviously hotly contested and not everyone agrees with my framework.
Laura, I am not all “blaming the patient”. The reason for the psychological element is that physiology and psychology are literally connected at the location of the dysfunction, the nervous system. This is why we often feel so irritable when we are unwell.
This is clearly a real physical dysfunction!
Once the dysfunction takes hold, many of the physical dysfunctions trigger and perpetuate the problem I describe. And as I describe above, the problem is also self-perpetuating in nature. So in no way is it just the sick person being negative. Neither will just thinking ‘everything is ok, I am in a happy place’ miraculously cure you.
But I believe that these psychological factors are important as part of an overall plan because not doing them can frustrate progress.
If you are to believe that the ANS dysfunction is centrally implicated in this illness, and there is a great deal of scientific research available to support this, much of which Cort has featured on his recent blogs, then you have to ask yourself how this can be corrected.
Besides annecdotal evidence of a large variety of strategies that have worked for people, there is much research into brain plasticity which has shown the brain to remain plastic even into adulthood. The reason why I mention the meditation (I was VERY reluctant to do this myself!), is because it has been medically proven that this has a huge impact on structures in the brain. (recently there was comprehensive literature review of hundrends of papers that concluded this, but I haven’t found the link – however, here is a link to the work of Dr Sara Lazar that works as part of the Massachusetss General Hospital / Harvard Joint Research – http://www.nmr.mgh.harvard.edu/~lazar/ )
So not only does it address the issues of arousal that I describe as central to the illness (both in terms of being too high and too low), but it has shown to physically change the structures even after a relatively short time!
Because so much of what I describe in the book includes information which we have already heard, people sometimes miss the main message of my book. I have done my best to make a succinct but comprehensive argument. – 🙂
Agreed – just because stress is a factor doesn’t mean the patient is to blame. Every single mammal on the planet experiences psychosomatic symptoms due to stress – from fear causing increased heart-rate, to extreme fear causing bowel movement, to long-term stress causing physical changes in the brain. It would be bizarre to say that rats in a maze are to blame for their brains releasing stress hormones 🙂
For some reason many people are scared of stress being a cause of CFS. There are two possible reasons for this. One reason is a general negative attitude to anything to do with ‘mental illness’: some people think that if you are affected by stress you must be ‘nuts’. A second reason is perhaps a cartesian belief that the mind and body are separate and that stress couldn’t possibly cause any illness symptoms.
Thank you for articulating so well what I am trying to say. I do understand a strong reaction to any suggestion that it is “mental”, would probably have reacted very strongly myself when I was sick.
But also people are misunderstanding the word STRESS. It is not just mental. If you go on an extreme exercise regime, have a physical injury, get an infection or suffer a toxic exposure, your system is experiencing massive stress.
That’s why I believe you see the clusters of CFS/FMS and hence the constant looking for viruses as the cause. Because a severe and aggressive virus, especially on a sub-optimal immune system, could represent a severe life-threatening stress.
But mental stress is just another stressor as a possibility. However, it clearly can become more prominent in the discussion if we look at longer term illness, because personally speaking, it’s hard to think of anything more stressful for me then when I had CFS/FMS. Dealing with such a terrible illness is a real ordeal!
Awesome commend FCP. I think you’ve hit the nail on the head.
Cheers,
Graham
So everybody who is ill (ie has physical stress) is also has a sick “mind”? Or does it only apply to those with ME?
Sorry that you had so much fear and emotional stress but I can’t say I have experienced that. However, I do have ANS issues.
The real problem is suggesting that what you experienced is what everyone else experiences and that what worked for you will work for everyone else. And if it doesn’t work there is something wrong with them. Hmmm where I have heard that before?
This is case in point for why diagnosing on the basis of not feeling well for 6 months and 4 nebulous symptoms is absurd.
Hi – I really appreciate your comment and questions, thank you very much. It warrants a detailed response!
No, not everyone has a “sick mind” as you put it, but many people suffer a whole range of real neurological symptoms and my point was that these can be linked through this explanation. (especially irritability!)
You not experiencing “fear and emotional stress or anxiety” before onset is not unique. Whilst I suffered a trauma a year before I got ill, everything was happy and normal and then I suddenly fell ill. I had been working hard, exercising hard and it was only when I had an immunisation that my illness started. But stressors can be cumulative and invisible until something reaches a tipping point in the body.
The nervous system responds to stress, regardless of whether it is something psychological or physical. That’s why I am suggesting the ANS as the causal and COMMON link. So you had no “psychological” stress leading up to becoming unwell, but I expect that you had another stressor such as a physical trauma, severe infection, toxic exposure or something along those lines.
My view is the OPPOSITE of what you felt I was saying. I DON’T think what worked for me will work for everyone else, in fact we know that is NOT the case. (otherwise we would have magic cure as front page news, right?) That is why I have tried to steer away from the exact things I have done despite this being what people want to know most.
Admittedly, there are a whole lot of strategies that will certainly have a significant positive impact on the vast majority of people (which I share in the book), and I have heard of others with extremely high success rates. But they are not necessarily enough to get everyone over the line. I believe this is because whilst I suggest we have the same underlying cause, the way it is triggered varies and can be VERY individual. That’s why I advocate a tailored solution and getting help from professionals where required.
Your comment “And if it doesn’t work there is something wrong with them.” – well, that would be very unkind to say to anyone with this illness! I think people try their best to get better and just because a strategy that has worked for someone else doesn’t work for you straight away, or even over a longer term, certainly doesn’t mean there is something wrong with them or they should blame themselves.
I do advocate taking personal responsibility, because this is empowering and because unfortunately it appears we cannot rely on a single external treatment to do all the work for us. But blaming oneself because you haven’t gotten over the illness is inappropriate and very counterproductive!
Sorry, I wasn’t sure what you meant about the 6 months or the nebulous symptoms.
The 6 months and nebulous symptoms bit is my snarky assessment of the CDC criteria. My point being that it is extremely unlikely that everyone based on such broad criteria has the same condition.
The other problem I see with the current criteria is that as the PACE and other “research” studies have shown is that one can have significant problems but no longer meet the criteria (however they choose to define it) for ME or CFS. For example, I don’t consider “fatigue” a primary or even a main complaint now but do have many of the immune (ie rather severe immune deficiency, something bordering on Mastocytosis or other strange immune dysfunction) and ANS issues (ie temp dysregulation, blood pressure, constant tachycardia, paradoxical breathing…). I also have difficult exercising aerobically (see deMeileir recent comments about ventilation, mine is 50% of normal) but have few problems with moderate activity.
My frustration is over the “fatigue” issue. There is a sense that if one no longer has “fatigue” then they are cured.
I appreciate the take charge approach but you have to realize there is almost guaranteed blowback by the CDC, disability/insurance companies jumping on the bandwagon and saying “see all these patients need are several counseling sessions, GET, some dietary assistance, stress management and maybe a few pills and they will be out of our hair”.
Well, what can I say? I think you and I are on the same page, even if you don’t think so.
I agree with you that CFS is about a huge range of problems and the name focussing on Fatigue is misplaced, just like it is with Fibromyalgia. Given your symptoms and your views about recovery (the last paragraph), I am surprised at your response to the book. It seems to me that we are on the same page.
I explain why GET is not helpful and why mere stress management and supplemenation whilst helpful, certainly isn’t necessarily going to get you there. But your and my defintion of ‘stress’ and ‘stress management’ is probably miles apart!
Perhaps consider reading the book again. I realise that a lot of the connections are a bit subtle. My main message is that the ANS dysfunction needs to be normalised for recovery, and that this is achieved by creating a low stress environment over a period of time whilst reconditioning the nervous system. It is a little more involved than the simplistic approach you mention. There probably needs to be a deeper discussion about this in the book, but I was trying not to overwhelm too much.
Stress is wide and varied and sometimes not easily recognised. When strong neuroassociation form over time, we sometimes don’t even realise the stressors as they don’t bother us on a conscious level, so a lot of this happens subconsciously which is where the ANS predominatly operates.
This is also true with physical stressors. You might have learned to ignore your symptoms and not be too bothered by, let’s say your gut dyfunction. However, with the ANS in flip flop mode, you are just reinforcing it constantly. The same happens when you have hypoglycaemic episodes and so on.
And when you mother in law comes over, and you get irritated and walk out to take a deep breath, it’s not like a healthy person where you just say whatever and get on with it. You may say it, but the damage of reinforcement has occured already (flip flop flip flop). Just because you think it doesn’t matter and you rationalise it (even with the counseling – 😉 ), doesn’t mean that these experiences don’t reinforce this dysfunction.
My goodness!! One of the things I’ve always appreciated about Cort is that he disseminates loads of information without bias, trusting his readers to their own interpretation and application. Since no one can say for certain the cause nor the perfect treatment for all people diagnosed with ME/CFS…and the possibility of many triggers to our similar symptoms…the more knowledge we have, the more options we can choose to explore, or not, for ourselves.
Last March, Research 1st (an arm of the CFIDS Association of America) posted an article by Alan Pocinki, MD, FACP of George Washington University Hospital, titled “Dysfunction Junction: The ANS and CFS”…for those interested. It resonated with me. The question I have is, if a dysfunction of the ANS is a feature of ME/CFS, is it a cause or an effect?
Keep up the good work, Cort!
Christine Mc
Oops…this comment was meant for post of Feb 18 re: Wyller’s study. Sorry about that, Dan. And thank you for the free book. Downloaded it last night…looking forward to reading it!
Christine
One interesting connection between:
• Autonomic nervous system (ANS) dysfunction, as discussed by Dan Neuffer in this article
• Brainstem dysfunction (which Wyller believes is the locus of ME/CFS)
• Enteroviruses (which statistically are strongly linked to ME/CFS)
is that viruses from a reservoir of enteroviral infection in the stomach can climb up along the vagus nerve, and get into the brainstem.
The vagus nerve, which is a major part of the autonomic nervous system, runs from the stomach to the brainstem, and Chia states that enteroviruses can transit along the length of this nerve in only about 3 days, by a ferrying process called retrograde axonal transport (RAT) that moves viruses along the nerve. Since the vagus nerve terminates in the brainstem, this allows enteroviruses traveling along this nerve to get direct entry into the brainstem. Ref: http://www.youtube.com/watch?v=Hl69xOZnDJI
There are certain host defense barriers that halt or impede the RAT transit of viruses along the vagus nerve, but presumably in ME/CFS, these host defenses are failing.
One simple theory of ME/CFS that I have been toying with is that the individuals who get ME/CFS from a viral infection are those whose host defenses could not prevent viruses in the stomach from traveling along the vagus nerve and reaching the brainstem.
In other words, my idea is that ME/CFS arises simply from a combination of a viral infection, and a breach in the host defense barriers of the vagus nerve, which allows the virus to enter the brain.
Furthermore, it occurred to me that by supporting the health of the vagus nerve and the autonomic nervous system, you can boost these vagus nerve host defense barriers, thereby halting the continual flow of viruses traveling along the vagus nerve from stomach to brainstem, and this may then allow the brainstem infection to finally clear up, and ME/CFS to heal.
This is a very interesting and notable comment.
Please see my response to Marco below for my thoughts.
I didnt get this until late. Last night the site was not working. Now I see the deadline for the free book ended Feb25. Can I still get the download? Is the video still available? I find this very interestng. I have had fibro for over 40 yrs. If you can please reply on facebook to me.
cindy
On the right track!
I have said consistently on this website that the problem lies in the brain / nervous system. The immune defects are secondary.
More research in this area, less on viruses, please!!!!
Why not both? I am not sure I can buy into the brain has been magically “rewired” yet. I’d rather see the theory that an enterovirus, VZV or other similar virus has gotten into the nervous system (ie like the Lights suggest) remain on the table until disproven.
Having now skimmed the book there is a lot I can agree on and also agree that a conservative approach is probably the best one.
But the answer to one ‘why?’ appears to be missing and may be where out two approaches diverge. Why US?
I can accept the notion of a ‘perfect storm’ overwhelming our ability to maintain homeostasis and this becoming a self perpetuating cycle (as I also suggest).
But why do we end up with ME/CFS and others don’t. Many are subject to much greater environmental and psychological stressors – their own ‘perfect storm’, yet don’t develop ME/CFS.
You also stated that you developed PTSD which is another interesting condition in which (it is estimated) some 90% of the population are subjected to severe traumatic incidents in their lifetime yet only a small percentage develop full blown PTSD.
Both examples suggest a predisposition of some sort.
You did mention having a ‘type A’ personality. I’m afraid that doesn’t cut it for me. Just another example of the ‘nominal fallacy’ of giving something a name and assuming that is sufficient explanation.
I’ve proposed a neurological model that predisposes us to developing a range of neuroinflammatory conditions including ME/CFS and which I suggest might also be recognisable from early ‘prodromal’ symptoms long prior to developing ME/CFS.
This model also suggests that pharmaceutical interventions may be possible and could greatly speed recovery.
I would also suggest that over time (6 years illness is a relatively short time-span for many) that some things may indeed become ‘broken’.
Any thoughts on this Dan if you’re still monitoring responses?
Thanks for your comment Marco and also Hip above.
I can see that you both are very technical, and very knowledgable. I do appreciate your deep thinking and the models you put forward. So please realise that I am not trying to take anything away from them!
It is my view that anyone can develop CFS/ME/FMS if they try hard enough (in hindsight, I did ALL the things that put pressure on the system, but how was I supposed to know – so I am not suggesting blame like some people think I am). But I don’t deny that a variety of predisposing factors are involved.
But predisposing is different than saying they are inevitable. I can have a predisposition to heart disease because I don’t metabolise omega 6 fatty acids as well, but that in no way means I am going to get it whilst I live a healthy lifestyle.
I briefly mention one predisposing factor in my video, which is that the locus coerulus (LC) doesn’t mature until later in life. So if a person suffered a period of severe stress in childhood for instance, then I believe this affects the cortisol receptors in the brain and the maturation of the LC. (please remember, stress comes in many forms – please don’t all keep thinking I am talking about just having to bliss out in a meadow and think happy thoughts!),
So such a weakness can then become a proplem when the perfect storm hits as the balance between neural and hormonal resonses becomes unstable and we are no longer able to maintain homestasis.
Marco and Hip, I think we can go into the details of how all these things happen, and I expect that you have a done an excellent job and may be fully or partially correct.
However, I challenge the view that we cannot get better without the use of drugs or that the illness is caused by a virus per se, even if it proves one day that we discover such a virus and that it has a role to play. We have to ponder the word “cause” carefully.
When someone sneezed across the road, I used to get sick when I had CFS (slight exageration, but only slight – 🙂 ) Last winter my whole family got sick, infecting each other with a virus. Because of my experience, I usually take better care of myself than most as I value health now. I eat good food, get sunshine, exercise and so on. Healthy as horse now. I didn’t get sick, the whole flu/cold season! So why? I ask, was their sickness ’caused’ by the virus or by lack of immune function? I know one person who hasn’t had a cold in 30 years! Think about it!
People recover all the time without treating such viruses. Why do we have to look for something inherently broken when we can see that people succeed in recovery in all manner of ways, all explained by this model of the ANS dysfunction?
And I understand your point that if people are sick for longer (say decades), that perhaps something is “broken”. Believe me, I pondered this a lot before I recovered, even when I was fully convinced by the ANS explanation! There are a lot of reasons why one might be able to make a supportive argument for this.
But given that recovery is possible, what is the value of focussing on such a possiblity? And in any case, I have seen ‘broken’ things get normalised due to ‘unexplainable’ phenomenon. Let’s face it, we only scratch the surface of the insane complexity of physiology, there is so much nobody knows. So why form unhelpful beliefs or assertions when we don’t know that they are really certain. And even “certain” terminal patients recover from cancer.
(sorry about the lengthy reply, didn’t mean to write a second blog – 🙂 )
Possibly, but you should also keep open the possibility that something is “broken” – in at least a segment of this heterogenous population. Part of the challenge with this is that it is unclear what mechanisms are in play.
Take celiac disease for example (sometimes a reason for “CFS”). If you did all the “right” things but continued to eat gluten you’re going to continue to feel miserable. It would take some understanding what was going on in your body to know enough to avoid gluten.
Hi Dan
I don’t believe we are too far apart in our thinking but whereas you propose that we were 100% normal and healthy prior to encountering the ‘perfect storm’ of various stressors I would contend that we have a (probably lifelong) predisposition to develop a neuroinflammatory state and it is this predisposition rather than any particular combination of stressors that results in the ‘state’ of ME/CFS (but could have resulted in a variety of other states that would attract alternative diagnoses). I also propose that regardless of any ‘lifestyle’ approach we remain vulnerable, perhaps increasingly so as we age.
In fact I would contend that it is this neuroinflammatory state that preceded the ‘perfect storm’ and ensured an impaired response regardless of the nature of the stressors.
You may consider this as merely a philosophical matter. You may stress the psychological and physiological aspects whereas I stress the neurological and physiological. Of course all three feed into creating and perpetuating the problem.
Where we differ is that I propose that the main driver underlying ME/CFS is not as ‘benign’ or reversible as you suggest.
One example is peripheral neuropathies which many PWME/CFS suffer. If your model is to include fibromyalgia (which I would agree i should) then it needs to explain (as in part 2 of my ‘blog’) the finding of peripheral neuropathy (confirmed by biopsy) in a cohort of fibro patients. These neuropathies may be reversible up to a point. Often they are not and result in permanent and increasing morbidity.
I also agree that a predisposition does not mean that developing any disease is inevitable and that ‘lifestyle’ can impact. But if you are genetically inclined to high cholesterol (as now appears to be the case regardless of decades of ‘lifestyle’ admonishments from the medical profession) you might not be too pleased to be refused the statins that might head off a heart attack or to be treated with lifestyle recommendations only in the event of a heart attack happening.
One approach needn’t preclude the other.
We may disagree on some points but I do agree that a conservative approach and various ‘lifestyle’ changes can be beneficial.
But I would also suggest that we could get there and stay there much quicker if the neuroinflammation was treated medically.
You make valid points Marco.
I also agree that medical intervention and treatments THAT DO NO HARM, can be very beneficial. Anything to reduce the burden and stress and symptoms on the system is helpful because this reduces the triggers in my view.
In fact, I know of people who have done just that to recover, they treated all their dysfunctions and supported their body and after a while they recovered. My only problem is that this doesn’t tend to work on it’s own, perhaps most of the time. I don’t actually have any stats to know for sure, but I think most of us agree that simply treating everything hasn’t led to recovery, even if it has helped.
However, treating the neuroinflammation is obviously getting much closer to the heart of the problem that I suggest, so your suggestion may hold much promise. My only concern is that if the other triggers are not addressed, it may still be ineffective in terms of total recovery. And based on the little that I have learned about neurochemistry, I have significant concerns about drugs that affect the brain directly, because this field is simply too complex and not well-enough understood. So I think people need to tread carefully.
Nonetheless, it strikes me that any medical treatment that affects neuroinflammation should certainly be investigated and it would be helpfu if the medical community would focus more on this aspect of CFS/FMS.
Dan, your hypothesis is provocative. I think I had your perfect CFS storm – divorced after 10 years of marriage while attending college and working at night. It was a real push to get that degree. Extremely stressful! Then a couple of years later, remarried and got pregnant at age 37. I remember the day CFS hit me. I was outside tending to the dogs, which I did every morning. But that morning was very different. I was 7 months pregnant, and the exhaustion I felt that day exceeded anything I had ever experienced, and that was the end of ever feeling healthy again. Just that one day. Hormones? My OB said I was tired because I was pregnant, and that all pregnant women are tired. I knew that was wong, because no woman would ever have more than one kid if they felt like that!
I downloaded your book – thank you for the free copy, but I fear I have too much brain fog to get through all the biochemistry! I’ll try, though. I’d sure like to go hiking again one day, or give my dog the daily walk he deserves.
Thanks for sharing your hypothesis!
Kathy
Thanks for the comment Kathy. I am pleased the ‘perfect storm’ resonated with you. It is a very common theme in CFS/FMS and hence I felt an important clue, beside the unreasonably high number of symptoms. I mention pregnancy in the book and why this can be a trigger due to the change in hormones. I hope you enjoy the book. Please don’t skim, the people who do (even the ones who really like it), don’t get the message of my book or make the connections.
I think that the ANS plays a major rol in this illness. But the overdrive reaction of this system can also be for compensation by lack of energy. (nor)adrenaline – cortisoll – immuunsystem. The parasympaticus don’t work anymore because the immunesystem is overactive. The system works both ways. It is complicated, but i agree the ANS can be the cause. If that is the cause i think there is a big problem in this system. I think the reason for this is an infection.
I’m sure infection is an initial trigger (it was for me) but I am also close to sure that it is not a perpetuating factor. The immune system and viruses has been studied quite a lot over the last 20 years and about the only relatively consistent finding is quite low natural killer cell activity, which could be caused by a number of non-immunity related factors. Viral studies have consistently proven disappointing. It may be that the degree of immune suppression resulting from some biochemical cause does of course perpetuate some sort of minor viral involvement.
I would be delighted if someone announced tomorrow they had found a treatable viral cause, but I think its highly unlikely.
For all her good intentions, Klimas et al seem to have been going around in circles with immune theories with little if any meaningful progress.
As I say I hope I am proven wrong but I’ve been watching the work of Klimas for more than 15 years and have seen little there that inspires hope in me.
To me its the people who are studying the brain and ANS who hold the hope
At the moment the ANS situation is even worse than the NKC/immune approach. At least with the immune system people have had some progress improving it. With the ANS, they tell you “yes, there are abnormalities there” but we don’t know why and can’t do anything about it yet. At least that’s what I’ve been told.
From an academic perspective the ANS may be more promising in the long term but for those struggling day to day it’s meaningless.
I currently see Klimas who as you pointed out is focused on the immune system. However, I also see Komaroff and Natelson who are more focused on the brain/ANS. Klimas is far better at the current time for improving daily function. The other 2 might ultimately provide a better solution but as they say “in the long run we’re all dead”.
The immune system is directly controlled by the ANS. But it is not just a immune regulation problem, but excessive cortisol levels directly lead to immune dysfunction as I point out in the blog.
I swallowed all the things I could find to boost my immune system, but it wasn’t until I recovered that it became strong. I would say, that it is now stronger than ever before in my life, which has been surprising to me. I think like most people, before I had CFS my lifestyle wasn’t that good. People with CFS really learn how to leave a healthy life!
Obviously I don’t agree that this discussion about the ANS is meaningless at all, because most (not all) of the people I have spoken to or know off that have recovered have focussed on this to achieve recovery. Whlist this may all be not so accepted, I hear of places in Europe (Skandinavia) where doctors actually prescribe specific ANS coaching. I have heard this second hand and have not been able to verify it. Also, this ANS hypothesis has a much wider acceptance in the UK.
You really need to be more specific in regards to immune system dysfunction. Klimas’ research is generally geared towards NKC activity. Key components of this are deficiencies in perforin and granzymes. Please provide references how this deficiency is caused by a “stressed” ANS. Thanks.
What Hip says rings a bell with me: I got CFS after a bout of aggressive flu; it only lasted for two days but I had to vomit every 15 minutes during my waking hours. This was after a prolonged period of sleep deprivation (onset of menopauze) and doing too much yoga (hindsight, practised for more than an hour every day). That fits the bill I would say!
Oke, lets say it is not an infection. What would be the cause of the abnormal ANS respons? Still it can be a compensation for lack of energy just like diabetes. Or is the ANS broken. We don’t know. It is verry difficult to find out. But we al agree that the ANS is a big problem. I think that an abnormal respons from nor adreanline on any stimuli can play a major role.
I don’t believe the ANS to be broken, I believe it to be dysfunctional. Based on my research and experience, I fully believe that by removing the triggers of the dysfunction for a period of time and reconditioning the neural response to the triggers, that this change can be effected and lead to recovery.
My recovery was achieved this way an I have heard of many others that have also done this.
Thanks Dan. I have also POTS, did you have POTS and the patiënts who are healthy now? I did not have a bad lifestyle at all. when i am 60 seconds on a bike or walk 5 minutes i am feeling verry bad. Even after 15 years of illness. I still do not know what your hypothese is that causes this dysfunction of the ANS. Can you explain? Or you think we are born with this. I agree the ANS can explain everything but there is somthing verry wrong.
I just don’t see how this ANS-as-cause theory can account for the extreme intolerance of exertion that people with ME experience nor for all the other accumulating scientific (as opposed to anecdotal–which your story is) evidence of profound physical abnormalities in this disease. There is so much evidence now that points to a much more complicated situation. Muscle biopsies have shown abnormalities of energy production at the cellular level. Lipkin declares that there is definitely B-cell activation, suggestive of either an autoimmune process or an ongoing infective process. Patients in Norway have shown dramatic responses to drugs that treat autoimmunity. I could go on and on.
The “accumulating stress” stories are exactly what Rudyard Kipling would have called a “just-so story.” You can tell any story in retrospect to explain how something happened. One person said above, I was working really hard, got divorced, then got remarried and got pregnant. Well, you know, just about half the population could say the same, but they didn’t get ME/CFS! In retrospect, you could probably paint almost any part of almost any person’s life as a “perfect storm” of stress, because that’s how life is…hard and challenging and ever-changing.
I happened to be at a pretty mellow period in my life when my disease began, but, according to Dan, of course, there must have been underlying or unconscious or accumulated stresses. He’s the self-nominated expert, so he knows better than I do, apparently!
Honestly, I think the stress theory is outright silly. Just plain silly. Just as silly as it was for ulcers or diabetes or epilepsy or any of the other things that were ascribed to it. Just as silly as saying that schizophrenia is caused by bad mothering. Or that multiple sclerosis is caused by hysteria.
Personal accounts of recovery are encouraging and can be enlightening, but it doesn’t serve the rest of us when a person claims that their recovery experience has unique relevance to the whole universe of “CFS” patients. Dan, you went through what you went through. Then you thought a lot about it, and read up (selectively), and came up with an explanation that you think works. Fine. It has exactly that much value. No more. Unfortunately, despite your congenial tone on this forum, your book takes a much more aggressive stance. You do, in fact, in more than one place, say that, if your program doesn’t work for people, then they haven’t done it thoroughly enough or aren’t taking responsibility, or don’t really want to get well.
If your only readers were going to be people who’ve been around the merry-go-round of this illness for a long time and have healthy skepticism, I wouldn’t worry so much. But you are also going to reach some people in the early stages following diagnosis, and they may be led down a dead end by you (and end up blaming themselves). This is irresponsible.
Thank you for your comments and feedback.
I don’t deny the dysfunctions you mention at all, in fact I discuss this cellular dysfunction in the book at some length.
I also totally appreciate your comments about the effective treatments, and it makes sense right? After all, if you have an immune dysfunction and there is a drug that helps with immune dysfunction, than you can expect that this would have some sort of a positive effect.
In no way am I saying that the only thing in CFS is the ANS dysfunction. Clearly there is a HUGE list of problems which respond to lots of different treatments. All I am asserting is that the ANS dysfunction is the root cause.
Of course you don’t have to agree with my view and I appreciate you taking a reasonable stance with your disagreement.
In terms of the stressors, I agree that people don’t always have psychological stress before onset, but in my experience their illness is usually triggered by a stressor of some kind (like an infection, physical accident etc.)
Regarding your comments “You do, in fact, in more than one place, say that, if your program doesn’t work for people, then they haven’t done it thoroughly enough or aren’t taking responsibility, or don’t really want to get well.” , don’t reflect the message I am trying to give.
So I am really sorry if my book has come across aggresively, and am dysmayed at the idea that anyone would feel I am blaming them for their illness. If you wish to contact me with specifics that you found offensive, I would certainly seek to correct my wording or tone, because that was not my intention. Not sure if you can appreciate how big a project this was and how much work it took. I do feel passionate about what I am saying, perhaps that didn’t translate well for everyone and some parts clearly need to be reworded.
I really appreciate the feedback and am sorry for any offense.
Thank you for your work Dan. I do have just a few questions. Why do you think women are more prone to develop CFS and fibro?
Also, elevated tumor necrosis factor has been found in both CFS and fibro. How do you think this may relate to the ANS?
In fibromyalgia, Dr. Wood has found spinal cord degeneration. This would explain the peripheral neuropathy. Do you think there is a connection to the ANS?
There seems to be a problem with collagen production in fibromyalgia. Research has shown reduced levels of collagen cross-linking. This would of course explain the connection to mitral valve prolapse, TMJ, and hypermobility. Do you believe the decreased collagen cross-linking is related to the ANS?
I just lost my lengthy reply – HOW FRUSTRATING!
Annesse, that’s a lot of questions – 🙂 You are all such clever people and I am sure if you have a bit of a look you can make most of the connections without too much difficulty.
Also please keep in mind that the connection between the ANS and different symptoms and dysfunctions is not always direct. In my view, often their are secondary dysfunctions that create this further problems. To try and make the connection to all dysfunctions would be an almost never ending job, and I am undertain how useful this would be.
But let me give you some brief thoughts (again – 🙂 ):
Whilst I have my own suspicions and thoughts about this difference between men and women, I am not sure they add a lot. All I will say is that we have very different hormone profiles, deal with stress in different way and experience different stressors. For example, pregnancy actually further changes the hormone profile and supresses the immune system to stop the immune system attacking the foreign tissue in your body (ie. the baby).
Regarding cytokines, as per my comment in the blog, these can be very adversely affected by excessive cortisol which is directly linked to the ANS.
I don’t know about the work of Dr Wood specifically, or the exact mechanism of this degenerationl. However, inflammation is very damaging over long periods of time, so no surprises there. And of course inflammation is a big part of CFS, hence the name Myalgic encephalomyelitis. And yes, I do believe it is linked to this dysfunction because inflammation and immune function is regulated by the ANS but as per your first question, can also be very damaging. I think if you follow Marco’s blog who had looked at this in great detail, who will find a better answer there, hopefully the connection to the problems with ANS regulation become apparent.
I don’t know anything about collagen cross-linking. What do you think?
I look forward to reading this book, and perhaps these issues are addressed in the book, but I have a few questions about your theory. Please don’t take these questions the wrong way. I am asking because I think a theory is made stronger if it can withstand a little scrutiny. I do think you are on to something here.
If the ANS is malfunctioning in all CFS patients, then why do only a relatively small percentage of these patients have abnormal autonomic functioning tests? From the literature I have read, it seems that a percentage, perhaps 25% or so, of CFS patients have confirmed autonomic dysfunction evidenced by abnormal tilt tests. Maybe I have missed something, but are their studies showing high percentages of CFS patients with abnormal QSART, TST, Valsalva, cold pressor, sweat gland nerve fiber density skin biopsies tests results? What about abnormal COMPASS scores or other validated autonomic scoring methods?
Also, the psychological symptoms that have been observed in CFS are not observed to a similar extent in other disorders of the autonomic nervous system, such as Multiple System Atrophy, Pure Autonomic Failure, or Postural Tachycardia Syndrome, so how would you account for this difference?
Another question, which I see others have asked above… if your ANS theory is correct, then what is causing the ANS dysfunction in CFS patients? I do not agree with the idea that it’s just stress in the traditional sense of the word. The ANS was built specifically to handle stress. That is one of its main functions, to allow the body to adapt to rapidly changing conditions and stressors. I think when we answer the, “what causes ANS dysfunction?” question, we are back to square one with having 1001 possible causes, with each patient potentially having his or her own unique cause, and there goes the unified theory out the window.
I did want to respond to ‘throughhiker’ who seems to argue that it can’t be the ANS because of the evidence of B-cell activation, autoimmune, infectious causes and muscle biopsies showing cellular energy production problems. ALL of those things can cause autonomic dysfunction, mostly by causing autonomic neuropathy. This is well documented in medical literature.
I believe, and I say “believe” because there is not enough data at this time to say this with any scientific certainly, that a substantial percentage of CFS patients have an undiagnosed autoimmune disease. Probably not everyone, but I “believe” many. Autoimmune diseases can be systemic, including attacking the ANS, and they can cause every symptom on the CFS symptom lists. They are notoriously difficult to diagnose. They do not always present in a way that can be confirmed by bloodwork (for example, it is widely published that about 30% of Sjogren’s patients do not have the SS-A or SS-B antibodies that are often used to diagnose Sjogren’s). Sometimes they do have a genetic or loosely inherited aspect to them. Sometimes it is known that they run in families, but the specific genes have not been fully identified yet. Then there is the reality that modern science has yet to discover every autoimmune disease, and even for the autoimmune diseases and antibodies that have been recognized in a lab, we do not have easily reproducible blood test for each of them yet. Finally, while there has been little research in the role of autoimmunity in CFS, just like ‘throughhiker’ I was very intrigued by the research out of Norway a year or two ago on Rituxan (a B cell deleting chemo drug that is also used in Rheumatoid Arthritis and non-Hodgkins lymphoma).
For the record, I was mislabeled with CFS, POTS and fibro. I wasn’t buying it. The POTS diagnosis was the closest fit, but it still didn’t explain WHY I was sick, since POTS, by definition, does not have a known cause. Just like CFS, at this time POTS is viewed as having a heterogenous origin. But Mayo Clinic has very credible research showing that 50% of POTS patients have autonomic neuropathy. I have autonomic neuropathy confirmed by all of the mentioned autonomic tests, and after searching far and wide for a cause, I finally found it. I have seronegative Sjogren’s Syndrome – an autoimmune disease that is attacking my autonomic nerves and other important parts of me. Normal bloodwork, but an absolute positive on my minor salivary gland lip biopsy. Long story short… my doctors put me on IVIG, my autonomic nerves grew back, and my symptoms went away. If the IVIG ever stops working, Rituxan is the next drug for me.
I would encourage all CFS patients to learn about Sjogren’s and make sure your doctors have properly ruled it out. Blood work alone cannot rule it out. Here is the most recent diagnostic criteria:
http://www.rheumatology.org/practice/clinical/classification/2012%20ACR%20Sjogrens%20Classification%20Criteria-FINAL.pdf
Lauren~I think you raise a very interesting point:
“Also, the psychological symptoms that have been observed in CFS are not observed to a similar extent in other disorders of the autonomic nervous system, such as Multiple System Atrophy, Pure Autonomic Failure, or Postural Tachycardia Syndrome, so how would you account for this difference?”
The ANS does control the secretion and flow of bodily fluids, so I think some of the symptoms of dryness associated with Sjogren’s and CFS and fibro could be contributed to a dysfunction in the ANS. Research shows that Sjogren’s patients have ANS dysfunction.
The elevated levels of tumor necrosis factor found in CFS and fibro are also found in Sjogren’s. In the study entitled “Tumor necrosis factor-alpha in tears of patients with Sjogren’s syndrome” researchers discovered TNF in the tears of patients with Sjogren’s syndrome, but did not detect TNF in the tears of normal controls. The researchers concluded, “TNF-alpha was detected in the tears of patients with SS, and tear TNF-levels showed a significant correlation with the grade of corneal epithelial damage, suggesting that TNF-alpha is a potent mediator in keratoconjunctivitis sicca.”
I believe the ANS dysfunction and TNF are two strong common denominators that CFS, fibro, and Sjogren’s patients share, which is why they are associated. Which is why I was asking Dan about the connection to the ANS and elevated TNF.
Here is some more information on the involvement of TNF in Sjogren’s.
The Future of Biologic Agents in the Treatment of Sjögren’s Syndrome
Jiska M. Meijer,1 Justin Pijpe,1 Hendrika Bootsma,2 Arjan Vissink,1 and Cees G. M. Kallenberg2
There is an overexpression of TNF-α, which is secreted by CD4+ T lymphocytes, mononuclear cells, and epithelial cells [2]. The intraglandular synthesis of TNF-α causes destruction of acini by up-regulation of Fas at the surface of the glandular epithelial cells, stimulation of secretion of type 2 and 9 matrix metalloproteases by epithelial cells, and overexpression of different chemokines [3–5].
Hi Lauren,
No, I don’t go into that detail in the book, because it was written predominately for the layperson that is often already overwhelmed by what I am saying, so it makes sense for you to pose the question. And scrutiny is great –
However, a detailed answer to these great questions is just about another book. Let me share some thoughts, hopefully Cort and some others will chip in.
You must appreciate that I actually came to my explanation on my own from the ground up. It was only afterwards that I realised that others had already postulated this long ago (I am not as original as I first thought – ) and that there is also much current research to demonstrate what I suggest. But being convinced myself, I don’t keep chasing new research. So I didn’t find my explanation in someone’s research paper or someone’s book, I pieced it together from known physiology and research about many aspects of CFS/FMS dysfunction.
If you use google scholar, you will find lots and lots of the type of evidence you are looking for, but here I go anyway.
The tilt test is only looking at one aspect of ANS dysfunction. There are many others. But not all papers find the same results. I have seen papers that show a difference for the cold pressor test, but not for heart rate response to deep breathing, whilst others clearly show difference in hear rate variability. It has to do with the subjects used and the specific testing methods.
I also believe that part of the variability in outcomes is that the dysfunction changes over time. In fact, when people first fall ill, I think that they don’t necessarily always have CFS/FMS, I think it often develops as the initial illness puts more pressure on the system.
Also keep in mind that there are different types of ANS dysfunctions. Whilst the brain stem is involved (where perhaps other ANS dysfunction usually occurs), in CFS/FMS, I am suggesting that we are seeing a flip/flipping from one end of the spectrum to the other. And a great deal of this comes from the limbic brain which then ties in with the other symptoms, especially pain perception.
I also feel that many of the psychological symptoms not only arise from this dysfunction in the limbic brain, but also from the change in neurotransmitter levels and hormones. I believe this changes occur not only due to the system trying to compensate for the extremes, but also because hormone receptors change over time (again, this is why I don’t think that we always actually have CFS/FMS when we first get ill)
The Dorsal Raphe is perhaps one of the most notable areas here. But also as secondary dysfunctions take hold (such as poor methylation), so that production and breakdown of various neurotransmitters is directly affected. And then there is Zinc which is crucial for brain function, and whilst I believe it is not generally considered a neurotransmitter, perhaps it should be! It is directly involved in modulating brain responsivity or excitability (sorry, couldn’t think of the right word).
Yes, the ANS is built to handle stress, but like any system, it only works to a point. I disagree about your unified theory point. If I theorise that my house is under water because the dam gates have been opened, then there can still be many reasons why this has happened. An electrical problem, human error, a mechanical problem, too much rain etc etc.
I see reasons other than genetic pre-dispositions as also being involved. I know some families where CFS/FMS is prevalent.
I agree that many people are misdiagnosed. You make a REALLY valid point about diagnosis. I think that true CFS/FMS is best characterised by the experience of a wider scope of symptoms rather than just focussing on a couple such as fatigue, pain, immune dysfunction or orthostatic intolerance.
In fact I think it is really dangerous not to be more diligent in identifying CFS/FMS, which is why exhaustive medical investigations are VERY important. I feel I can’t stress this strongly enough.
Hi Lauren!
I actually agree with everything you said 100%. I wasn’t at all arguing that the ANS isn’t part of the problem. I have terrible orthostatic intolerance–it’s possibly my biggest problem. Like you, however, I don’t see the ANS, or especially “stress” messing up the ANS, as causal. Rather, some infective or autoimmune process is likely harming the ANS and preventing it from working properly. From everything I have read, I am leaning toward an autoimmune explanation myself.
I am intrigued by your new diagnosis of Sjogren’s. I’m so happy that you have found a solution that has helped you! Since autonomic symptoms were so central to your illness, as they are to mine, I am suddenly wondering if I might also have Sjogren’s. I remember very early in my illness (8 years ago), I kept reading descriptions of Sjogren’s and feeling that they sounded a lot like my illness. I will follow up on this. Meanwhile, I would love to contact you by email to learn more about your illness, your diagnosis, and your treatment. Can we arrange that?
Hi
Is there any way I can get my hands on a copy of this book? I went on Amazon but its just the Kindle edition they do and I don’t have a Kindle.
Thanks in advance
Vanya
You don’t need a kindle – it can be read on any computer device with these free APPS:
http://www.amazon.com/gp/feature.html/ref=sv_kstore_1?ie=UTF8&docId=1000493771
I took the time to read your book. You have it backwards. Methylation controls the ANS, not the other way around.
According to Vinitsky: “When the resources for methylation are limited, those functions that are not immediately necessary for survival or stress reversal will be reduced or suspended. The consequences of this principle account for the evolution of regional and generalized autonomic dysfunction.”
Read more: http://www.faqs.org/patents/app/20120231089#ixzz2MAfKikjv
This is not to say that the ANS doesn’t have an influence on methylation in that stress depletes B vitamins, which are needed for good methylation function. Or that addressing ongoing stress or past traumas still causing stress wouldn’t help take a load off that system. If stress is your main issue, then you should by all means address it. Emotional Freedom Technique or EMDR can be helpful for rapidly resolving past traumas. CBT can be helpful for learning how to deal with ongoing stress. But this would be part of an overall strategy, not a sole treatment.
It’s ridiculous to say that a person doesn’t know when they’re stressed. They do. There are all kinds of physical and mental signs. Even little kids know when they have butterflies in their stomachs.
If what you’re saying is true, why doesn’t every hard driving Type A person who burns that candle at both ends have ME/CFS? This would be every doctor in medical school, every politician on the campaign trail, every elite athlete, and so on. In fact, I don’t think humans would have survived history at all if this were the case. Humans have had plenty of long term severe stress in history – wars, famines, plagues, climate change, etc.
Personality doesn’t have anything to do with developing ME/CFS. In fact, of the 5 PWC’s I know in person, they’re all very mellow personalities, not hard driving at all, the exact opposite of what you predict. If a proper survey was ever done (not on the internet as certain personalities are over-represented), I think you would find the whole range of personalities, as you would for any disease.
So, we’ve always had stress, we’ve always had viruses (nobody up to this point has been able to find a novel virus causing ME/CFS). What’s new? The amount and type of toxins present in modern every day life. Most people are totally unaware of their exposures. It starts in utero, and goes on 24-7 every day of your life, unless you’ve learned to pay attention and clean up your environment. Which, of course, is impossible to do totally, seeing as how we’ve screwed it up so badly. Even native people living in the pristine Arctic thousands of miles from civilization have dioxins and flame retardants in their fat.
MCS is due to glutathione depletion. For every toxin molecule, your body uses one glutathione molecule to deal with it. No glutathione, no detoxification – you react to a tiny drop of say, paint thinner, as if you had stuck your head in a bucket of it and inhaled the fumes deeply. Read Sherry Roger’s book “Tired or Toxic” for a very enlightening look at MCS, detoxification, and where the various exposures come from. Glutathione depletion is due, of course, to methylation cycle dysfunction.
The reason why some people get sick and some people don’t (given the same exposures) is genetic susceptibility. If your methylation cycle is already genetically compromised from conception, you’ve already started with half a deck of cards.
This hypothesis also explains why there has been an astronomic increase in all types of “modern” chronic complex diseases – autism, cancer, and mental illness, just to name a few besides ME/CFS.
Your hypothesis doesn’t explain why ME/CFS can run in families (even those who are adopted and don’t have the same exposures as their birth parents, nor does it explain clusters). Clusters of Type A people having stress? Really? Sounds like hysteria to me.
And last, but not least, you’re spelling Rich’s last name wrong – it’s KonyNenburg, not Konyenburg.
I agree with you Calendonia. When I got sick, it was at good time of my life. The “stress” came after I got sick. Funny how some of my very close friends and family have the following going on:
– Loss of child
– Difficult divorce
– Sick mother who has to move into home with very unhappy spouse and 3 kids
– Loss of high paying job and significant change in lifestyle
and none of them have gotten CFS. Stress is part of being alive and is certainly not a new variable.
I wholeheartedly agree with your statements about stress–you have put it so clearly! It is so interesting that Dan (and others) keep insisting that the illness is triggered by a stressful experience, because, of course, if a big part of the illness is that the ANS is damaged (by some factor, whether infective, autoimmune, or toxic), then any big stress (physical or emotional) could create a sudden “reveal” of the illness, and could then easily be interpreted as more central or “causative” than it really is. So there would be people who could point to a stressful event as the source of their illness, and there would be others who would have no such evident “cause,” and that is exactly what we see in ME/CFS. This is exactly the situation with multiple sclerosis: some people have a sudden “reveal” of the disease after a stressful event and others don’t, but the stress isn’t in any way causative or even terribly meaningful. It’s just the moment in life that revealed an underlying disease process.
Yes, I’ve heard the word “unveiling” which is an alternate way of saying “revealing”.
The cure for CFS is never going to be hidden at the end of a book.
Most CFS people won’t even be able to reach the second chapter of it.
These are cruel ways to make money.
A “cure” (ie. a single treatment that works for everyone that can simply be applied, like a medication) does not exist for CFS.
So it is not in the book.
Everyone that bought the book (free or otherwise), can see the second chapter. I suspect you didn’t download the book but that you just looked at the preview on the Amazon site.
Nothing cruel about it. – 🙂
They just posted last year a clinical trial about this!
Autonomic Nervous System and Chronic Fatigue Syndrome (CFS&ANS)
http://clinicaltrials.gov/show/NCT00580619
No results have been posted yet
Thank you for being forward and make medical doctors think!
Thanks Emily, that’s a really good trial.
I have to say, my initial and overwhelming response is “thank goodness, AT LAST!!!…application of logic and a healthy dose of common sense at last!” Quite right, the observation that these illnesses are yet to be investigated by the medical fraternity with a ‘top, down’, holistic approach. I use holistic in all forms of it’s definition, colloquially accepted and otherwise.
Your hypothesis would also account for the statistically high number of persons with other illnesses who tend to develop Fibromyalgia as a supposed secondary, or potential longer term ‘complication’ of their initial diagnosed ailment. Hypermobility/EDS and Lupus are two that spring to mind.
We live in hope and a resoundingly huge thank you to you for providing an avenue of what looks to be real hope for real answers and possible solutions or effective treatment. Not to mention the restoration of faith that logical thinking still exists 😉 🙂
Thank you Mel, I really appreciate your positive comment. 🙂
Hi Dan, I agree with your hypothesis regarding the ANS being the central problem in ME/CFS. Though I think the original stressor – the virus / mycoplasma / toxin / heavy metal / mitochondria toxin / other stressors which infect the ANS or disrupt the ANS are the real root causes. The ANS needs a significant stressor or set of stressors in order for it to dysfunction, and reach the levels of dysfunction found in ME/CFS patients. And the stressor(s) has to be the root cause. The genetic studies of Dr. Light in Utah have provided us with some very deep insights into the ANS and its relationship to immune function, muscle function, mitochondria etc. and their work is continuing in this regard.
The emphasis on psychological stress is important in the context of great pressures on people nowadays from having to work harder and longer in a highly competitive globalised economy which largely enriches the already rich while driving most people either into poverty and unemployment or over-priced homes and lifestyles, unsustainable debt and/or stress-related illnesses and early death. And of course, for ME/CFS patients there is the stress of loss of job, loss of marriage, loss of home in some cases, no ME/CFS clinics and no treatment, and the discrimination and stigma which ME/CFS patients are forced to suffer in many societies, its particularly bad in the republic of Ireland. In Ireland the view of many people, including the ‘holy joes’ is that ME/CFS patients deserve a kick in the ass to get back working again ; this is outrageous and nasty, but shows how hard peoples attitudes in some societies.
I am working with some other ME/CFS patients and their carers / families to get the governments to build a new type of ME/CFS clinic in Ireland and Britain. And I have come to the same conclusion as yourself, Dan, in relation to the ANS and stressors, and included our hypothesis on our web site http://www.cfs-ireland.com
http://www.cfs-ireland.com/diagram5a.jpg
http://www.cfs-ireland.com/diagram11.jpg
The diagnosis and treatment of ME/CFS is complex and multi-faceted and not predicated on one factor alone. This is outlined in our clinic proposal. I think that stressors and the ANS are the key.
Congratulations on your book, Dan, it is a significant contribution to the field.
Hi David – thank you very much for your positive feedback and well done for efforts to help people with ME/CFS. I wholeheartedly agree with your comment about the ignorant comments by some people about ME/CFS. It truly is nasty, although I suspect people are just ignorant and perhaps not realising how inappropriate and incorrect their comments are. But so frustrating when people are already suffering, to have to hear stuff like that. Even being recovered for some years now, it still pushes my buttons.
Your argument about the root cause make sense, because after all this (whatever it is with each person) started the illness. But in my view, whilst there may be one obvious trigger, there are usually multiple factors at play at onset, including a variety of predispositions.
Having said that, the reason why I describe the ANS as the root cause, is that even when the original cause or trigger is extinguised, the illness perpetuates and I believe the ANS dysfunction to be the root cause of this. Good luck with your work in Ireland – 🙂
dunno where to post this; too tired to put it into context, but…it interested me. So for what its worth @
http://news.wustl.edu/news/Pages/25064.aspx
New clues to causes of peripheral nerve damage
March 6, 2013
By Caroline Arbanas
Anyone whose hand or foot has “fallen asleep” has an idea of the numbness and tingling often experienced by people with peripheral nerve damage. The condition also can cause a range of other symptoms, including unrelenting pain, stinging, burning, itching and sensitivity to touch.
Although peripheral neuropathies afflict some 20 million Americans, their underlying causes are not completely understood. Much research has focused on the breakdown of cellular energy factories in nerve cells as a contributing factor.
Now, new research at Washington University School of Medicine in St. Louis points to a more central role in damage to energy factories in other cells: Schwann cells, which grow alongside neurons and enable nerve signals to travel from the spinal cord to the tips of the fingers and toes.
The finding may lead to new therapeutic strategies to more effectively treat symptoms of this highly variable disorder, the scientists report March 6 in the journal Neuron.
“We found that a toxic substance builds up in Schwann cells that have disabled energy factories, leading to the same kind of nerve damage seen in patients with neuropathies,” says senior author Jeffrey Milbrandt, MD, PhD, the James S. McDonnell Professor of Genetics and head of the Department of Genetics. “Now, we’re evaluating whether drugs can block the buildup of that toxin, which could lead to a new treatment for the condition.”
The most common cause of peripheral neuropathy is diabetes, which accounts for about half of all cases. The condition also can occur in cancer patients treated with chemotherapy, which can damage nerves.
In the body, Schwann cells wrap tightly around nerve axons, the fibers that relay nerve signals. Graduate student and first author Andreu Viader and colleagues in Milbrandt’s lab studied Schwann cells in mice with genetically disabled mitochondria, or cellular energy factories. Under normal conditions, these mitochondria produce fuel and intermediates of energy metabolism that allow nerve cells to function.
The researchers showed that the crippled mitochondria activated a stress response in the Schwann cells. Instead of synthesizing fatty acids, a key component of Schwann cells, the cells burned fatty acids for fuel.
Over time, inefficient burning of fatty acids by the crippled mitochondria leads to a build up of acylcarnitines, a toxic substance, in the Schwann cells. The researchers found levels of acylcarnitines up to 100-fold higher in these mutant Schwann cells than in healthy Schwann cells.
And the bad news doesn’t end there. Eventually, the toxin leaks out of the Schwann cells and onto the nerve axons. Studying neurons in petri dishes, the researchers showed that acylcarnitines damage nerve axons and disrupt the ability of nerves to relay signals.
“The toxin leaking out of the Schwann cells and onto the adjacent nerve axons causes damage that results in pain, numbness, tingling and other symptoms,” Milbrandt says. “We think that is a likely mechanism to explain the degeneration of axons that is known to occur in peripheral neuropathies.”
The new research suggests that drugs that inhibit the buildup of acylcarnitines may block axonal degeneration. Milbrandt and his team now are evaluating the drugs in mice with disabled Schwann cells to see if they can slow or alleviate the decay of axons.
——————————————————————————–
The research is supported by the National Institutes of Health (NIH) Neuroscience Blueprint Center Core Grant (P30 NS057105), the HOPE Center for Neurological Disorders and the National Institutes of Health (AG13730 and PPG 2P01 HL057278).
Viader A, Sasaki Y, Kim S, Strickland A, Workman CS, Yang K, Cross RW, Milbrandt J. Aberrant Schwann cell lipid metabolism linked to mitochondrial deficits leads to axon degeneration and neuropathy. Neuron. March 6, 2013.
Washington University School of Medicine’s 2,100 employed and volunteer faculty physicians also are the medical staff of Barnes-Jewish and St. Louis Children’s hospitals. The School of Medicine is one of the leading medical research, teaching and patient care institutions in the nation, currently ranked sixth in the nation by U.S. News & World Report. Through its affiliations with Barnes-Jewish and St. Louis Children’s hospitals, the School of Medicine is linked to BJC HealthCare.
I can’t believe we are even discussing this. I became ill suddenly in January 1990 (23 years ago!) after a very bad flu. I understand that my brain was damaged by the flu and will never recover. My primary Dr. at this point is a cardiologist — the only Dr. who so far has addressed my ANS symptoms primarily and prescribed appropriate ANS-calming drugs (calcium channel blocker, beta blocker, hormone therapy and later anti-anxiety medication for super IBS and a state of over-excitement of the brain that had to be stopped). I had two reactions to your book and this site. Both are strong enough that I wished to post.
I went to look at your book right away because I have never given up hope of finding something I hadn’t seen before but I am dismayed by what I found. 1) This is old news and 2) I can’t believe you would charge money for it if it were a cure (and it is advertised as a cure).
I received the very best instructions when I was first diagnosed with FMS in the context of CFS. I was to r-e-l-a-x any way I could. I had a premier Dr. in Fibromyalgia. He wrote one of the first substantial books on Fibro. He seemed to “get” my illness and I felt relief. But after many years of complaining about the same symptoms, I was told that I needed to try harder to find stress relief that worked. I was made to feel as if I wasn’t trying hard enough or I would be better. That, I know now, is complete nonsense. When working with a Dr. to relieve symptoms pharmacologically, I finally got relief I needed. I suppose that the intent of your book was to provide the preliminary and necessary physical and psychological stress measures that most of the CFS patients I have read know and adhere to early on with relief but no cessation of CFS. This is simple stuff to those of us who have been ill for decades.
Now, the hard part is that I know how hard it must have been to research and write this book. I know authors and I know CFS sufferers. But I have to say that if any true CFS sufferer (including me) ever found a cure, or the magic marker for CFS, they would shout it from the rooftops (and online forums) for all to hear and hope that no one went without hearing about it. Yes, I know, CFS can inhibit one’s earning power so why wouldn’t a book be a good way to make money? Because in this form (Eureka!) it sounds like snake oil. Amazon’s description of it certainly didn’t help. “…the Discovery Essential for You To Recover.”
Dan, I’m sorry but this isn’t a discovery. It isn’t going to help me recover, although I subscribe to the methods myself, and it feeds false hope in the way it is presented. I especially resent the notion that some CFS sufferers aren’t taking responsibility for recovery.
Sorry, but after 23 years of listening to sufferers online and reading everything I could get my hands on, I can’t believe that you actually had CFS if you are truly well now. I haven’t seen one actual recovery, although some have periods of wellness or even get better over time, they are still damaged. I believe that you may have had something with similar symptoms to CFS, but if you did have CFS and recovered, you should be in a medical journal STAT because you are one in a million.
Thank you for your comment, I am sorry about how you feel about the book.
Please contact me via the website to give me any specifics about how the book is advertised as a “cure”, because it certainly doesn’t contain one (unfortunately!). If you had the chance to read the book, you probably realised that I am describing my view of the illness as more complex than that.
I understand your feelings about anybody possibly recovering from CFS.
I’ve had CFIDS for 30 years following a C-section on July 4, 1982. All symptoms turned on that day and my life has been very difficult living with all the horrible symptoms.I have most of them,. Done lots of alternative treatments but still ill. Last year was diagnosed with psoriatic arthritis and I’m allowing the docs to treat me with Embrel. Have not started yet, but I feel at this point I don’t have much to lose. Just wondering if others have run into this and if the Embrel helped the CFIDS/CFS/Fibro/ME?
Sheila
I was wondering what your thoughts were on MTFHR testing and if you think they are worth getting? Also just want to thank you for putting out this information for those of us who have suffered for so long without a voice.
Kitt
It’s my understanding that a significant proportion of the population (I believe around 20%, but don’t quote me) have this polymorphism – and yet have no symptoms of any type.
So whilst methylation is an issue in my view, it is not a causal factor. None of the people that I have met that recovered (even after 20+ years) used the methylation protocol to do so. It’s just another secondary dysfunction in my view.
You might like to check out my explanation video on my site: http://cfsunravelled.com/video-explanation/ for more details of what I mean.
Cheers,
Dan
Other than maintaining proper nutrition and balancing hormone levels, what is the next step in your opinion for treating people with CFS/ME/Fibromyalgia? We find that this protocol works for a vast majority of our patients, but there are a few who don’t seem to benefit from our efforts. We use proper nutrition, bio identical hormone replacement therapy (with regular blood tests), and natural supplementation as well as other techniques based on individual needs but the more we can learn, the better. Looking forward to your response! Thanks : )
I describe a multi-lateral appraoch in CFS Unravelled.
But other key things required are creating a healing environment. This means dealing with the stress of having the terrible illness, as well as addressing any other stressors. It’s about interupting the trigger neuroassociations in the nervous system and rewiring it to function normally.
I didn’t go into enough depth in the book about this because it doesn’t lend itself as easily to the written word and aim of the book was to convince the reader of the etiology in the first place. However, I hope to describe this in more detail in 2014.
Also, people may need to address any past trauma’s. Whilst these may not have made them sick in the past, once the ANS dysfunction sets in, it can keep them locked in the illness!
Hope that helps. 🙂
If it wasnt for Dan’s ANS Rewire Program i dont know how and if i would ever get my life back like a normal person. I have my life back at 32 years old and suffered since i was 16! Thank you thank you thank you 🙂
Hi, is anyone currently looking at this, as most of the comments, apart from the last one, are from years ago? I have information I’d love to share with others, if anyone’s interested?! Tracey
Thanks Tracey – please either post in the comments or send it to me at cortrising@gmail.com. 🙂
Hi Tracey,i am interested in what you have to say I am listening.