


( In this article Amber, a former biologist, explains the ins and out of one the most difficult to understand but important tests done in ME/CFS – maximal cardiopulmonary exercise CPET) testing. In doing so she’s produced a document that both patients and doctors can benefit from (and provides a copy of an actual CPET workup).
Thanks to Amber for her willingness to do the work to shine a light on a very complex subject and for sharing her work on Health Rising. (For this overview a printout might be helpful and a button to produce a document / PDF file is available at the lower left hand part of the page. I added some images – Cort))
Myalgic/encephalomyelitis (ME/CFS) is a disabling neuroimmune disease that affects over 20 million people worldwide. Approximately 25% of patients with this disease are housebound and 80-90% are unable to work.

Because it strikes at the physiological core of what is happening in ME/CFS exercise testing is often used as a stressor in studies. It also provides objective evidence of diminished functionality for those seeking disability.
Despite these staggering statistics, ME/CFS is one of the more challenging conditions for which to receive disability benefits in the United States (and elsewhere). The reasons for this are complex, but stem largely from a mischaracterization of the disease by the Centers for Disease Control and Prevention (CDC) and a long history of poor research funding from the National Institutes of Health (NIH).

Poor funding has slowed research and left patients without a definitive test (i.e. biomarker) for this disease, let alone any FDA-approved treatments. The absence of a diagnostic test and accepted treatments has allowed deeply flawed stereotypes to take hold in medicine, a fact not lost on long-term disability (LTD) companies and the Social Security Administration (SSA). This places the burden of proof on patients.
One of the only tests that shows the disability experienced in ME/CFS is the 2-day cardiopulmonary exercise test (CPET). The CPET directly measures an individual’s capacity for work and is considered the gold standard for measuring disability – not only for ME/CFS but for a variety of other conditions. A second day of testing is needed for ME/CFS patients because it is the only way to demonstrate the unique impairments underlying the disease.
Having a poorly understood condition means that ME/CFS patients are faced with a tough choice. The 2-day CPET helps to increase the chances of being awarded disability benefits, but undergoing the test increases the risk of getting sicker, as most exercise is strongly contraindicated for ME/CFS patients. No one should have to face such difficult choices, but this is the reality for people with this disease.
Fortunately, ME/CFS patients have strong allies at the Workwell Foundation, Ithaca College, Cornell University, and other research institutions. These groups are focused on understanding the functional impairments found in ME/CFS. In fall 2017, Drs. Maureen Hanson and Betsy Keller, in collaboration with the Workwell Foundation, received one of the three Collaborative Research Center grants awarded by NIH to nail down the immunological, neurological and metabolic changes that underlie post-exertional malaise (PEM) using the 2-day CPET. PEM is a worsening of neuroimmune symptoms that follows exertion and is the cardinal component of ME/CFS.
Using a sample 2-day CPET evaluation (see Appendix 1), the aim of this article is to help patients better understand how to read a CPET report.
Testing for Disability at the Workwell Foundation
Researchers at the Workwell Foundation pioneered the 2-day CPET for ME/CFS and are the experts at writing reports that assess the level of disability experienced by ME/CFS patients during and after physical exertion. A 2-day CPET can also confirm a ME/CFS diagnosis by demonstrating PEM. They have published extensively on exercise intolerance in ME/CFS, lending further credibility to their work.
People with ME/CFS often show a marked drop in functional capacity on the second day of exercise testing, which is not found in other conditions. According to Workwell, even patients with severe heart failure can repeat their results on the second day of exercise testing. Day-to-day test variability is less than 8% for healthy individuals. The abnormal response between the two tests provides evidence of impaired recovery after exertion (aka PEM).
It is impossible to fake a CPET, so the results tend to carry far more weight than a list of subjective symptoms.
The CPET is also called a maximal graded exercise test. The “maximal” part refers to exercising until it is no longer possible, while seated on a cycle ergometer (stationary exercise bike). A CPET can be done on a treadmill, although this is not recommended by the Workwell Foundation due to the risk of falling and other reasons.

Patient undergoing CPET test on bicycle at Workwell
A maximal effort is required to measure the aerobic energy impairments that are unique to ME/CFS (submaximal testing is not sufficient).
The graded exercise part of the test (not to be confused with Graded Exercise Therapy!) involves a 10 watt/minute ramping protocol; i.e., for each minute of the test, pedal resistance increases by 10 W (this amount may vary depending on age, gender, and level of illness).
Prior to the test, patients are hooked up to a 10-lead ECG and vitals are recorded. When ready, patients mount a stationary exercise bike that is fitted with equipment that captures and analyzes expired gasses to determine oxygen consumption, carbon dioxide production, and pulmonary ventilation. Heart rate and blood pressure are measured before, during, and after the test. Two exercise tests are performed on consecutive days to determine the response to exertion.
Prior to the test, patients are provided with a chart showing different levels of perceived exertion, with 20 being the highest level of difficulty. Patients must reach a minimum level of 17 for the test to be considered a valid maximal exercise test.
The tests last for 8-12 minutes and the vast majority of Workwell clients are able to successfully complete it on both days.
Patients are told that if they try to stop before the relevant data are collected, they will be asked to continue. However, patients are not told when to stop so as to not influence the test. Most patients go beyond the point necessary in an effort to make the test as meaningful as possible.
After reaching the maximum amount of exercise tolerated, patients are given a cool down period during which they continue pedaling without resistance.
The test is repeated the following day at the same time.
What gets measured in the 2-day CPET?
Assessment of effort
Quantifying effort is essential for addressing the misguided belief that ME/CFS patients are deconditioned couch potatoes, or worse, malingerers. The Workwell Foundation has two ways of measuring effort. First, they measure peak respiratory exchange ratio (RER), which is the ratio between the amount of carbon dioxide produced and oxygen used. RER is an objective measure and cannot be faked. According to the American Heart Association, a RER greater than 1.1 indicates excellent effort. Second, they use the patient-reported scale for perceived exertion, with anything above 17 points (out of 20-point scale) indicating that maximal effort was reached during the test.
The Workwell Foundation states that nearly all ME/CFS patients give it their all during testing and maximum effort is nearly always reached.
Metabolic responses
VO2 max: VO2 is a measure of the body’s efficiency at doing work. VO2 max is the maximum rate of oxygen consumption during incremental exercise. It is expressed in milliliters (mL) of oxygen (O2)/kilogram(kg)/minute and depends on age and gender. VO2 max is reached when O2 levels remain at a steady level despite an increase in workload.
VO2 max is a direct measure of disability because it captures the functional capacity, or level of work, a person is capable of doing. The average VO2 max is around 35–40 mL/kg/min in healthy sedentary males and 27–31 mL/kg/min in healthy sedentary females (Table 1) and declines by ~10% each decade after the age of 30. VO2 max is approximately double for endurance athletes.
A functional capacity (VO2 max actual/ VO2 max predicted) greater than 85% is considered normal.
Table 1. VO2 max by gender and age.
FEMALE
(mL/kg/min)
| Age | Very Poor | Poor | Fair | Good | Excellent | Superior |
| 13-19 | <25.0 | 25.0-30.9 | 31.0-34.9 | 35.0-38.9 | 39.0-41.9 | >41.9 |
| 20-29 | <23.6 | 23.6-28.9 | 29.0-32.9 | 33.0-36.9 | 37.0-41.0 | >41.0 |
| 30-39 | <22.8 | 22.8-26.9 | 27.0-31.4 | 31.5-35.6 | 35.7-40.0 | >40.0 |
| 40-49 | <21.0 | 21.0-24.4 | 24.5-28.9 | 29.0-32.8 | 32.9-36.9 | >36.9 |
| 50-59 | <20.2 | 20.2-22.7 | 22.8-26.9 | 27.0-31.4 | 31.5-35.7 | >35.7 |
| 60+ | <17.5 | 17.5-20.1 | 20.2-24.4 | 24.5-30.2 | 30.3-31.4 | >31.4 |
MALE
(mL/kg/min)
| Age | Very Poor | Poor | Fair | Good | Excellent | Superior |
| 13-19 | <35 | 35.0-38.3 | 38.4-45.1 | 45.2-50.9 | 51.0-55.9 | >55.9 |
| 20-29 | <33 | 33.0-36.4 | 36.5-42.4 | 42.5-46.4 | 46.5-52.4 | >52.4 |
| 30-39 | <31.5 | 31.5-35.4 | 35.5-40.9 | 41.0-44.9 | 45.0-49.4 | >49.4 |
| 40-49 | <30.2 | 30.2-33.5 | 33.6-38.9 | 39.0-43.7 | 43.8-48 | >48 |
| 50-59 | <26.1 | 26.1-30.9 | 31.0-35.7 | 35.8-40.9 | 41.0-45.3 | >45.3 |
| 60+ | <20.5 | 20.5-26.0 | 26.1-32.2 | 32.3-36.4 | 36.5-44.2 | >44.2 |
Using the example in Appendix 1, VO2 max was 21.7 mL/kg/min on day 2 of CPET testing. At 50 years of age, this is classified as “poor function” (Table 1).
V/AT: No one lives or works at their VO2 max. The more relevant measure of disability for ME/CFS patients is the ventilatory/anaerobic threshold (V/AT) because it shows the amount of work that can reasonably be sustained. V/AT corresponds to the point at which lactate and/or lactic acid begin to accumulate exponentially and cannot be cleared from muscles and the blood stream faster than it is generated. This represents the point at which anaerobic metabolism – an inefficient form of energy production that produces toxic by-products – kicks in. This happens, in part, because there is not enough oxygen to keep up with demand.

The aerobic energy production system (the tortoise) provides long periods of sustained energy. Problems with that system make sustained activity difficult or impossible for people with ME/CFS. (Tortoise image from CC BY 1.0, https://commons.wikimedia.org/w/index.php?curid=13617)
V/AT can be expressed either as the amount of oxygen (VO2) that is consumed at the anaerobic threshold or as the heart rate at which the crossover into anaerobic metabolism occurs. If this occurs at a low rate of oxygen consumption and/or at a low heart rate, normal daily activities may be more than a person with ME/CFS can manage.
Most of our energy demand is met using aerobic metabolism, which typically covers energy for activities such as walking, seated tasks, and other basic activities of daily living. According to Workwell, the reduction in V/AT following exertion demonstrates that there is a greater reliance on anaerobic metabolism to support lower intensity work that would normally be met with aerobic metabolism.
Energy expenditure at or above V/AT is fatiguing, can only be sustained for short periods of time and results in the delayed recovery seen during PEM. This is why Workwell cautions against spending more than 2 minutes with your heart rate above V/AT and minimizing the number of times V/AT is crossed in a day.
According to Workwell, VO2 and work intensity at V/AT are important measures of the capacity to do continuous work.
As Staci Stevens from the Workwell Foundation puts it, aerobic and anaerobic metabolism are like the tortoise and the hare. Aerobic metabolism is the long and slow system (the tortoise), but one that nets 36 ATP molecules per molecule of glucose. Anaerobic metabolism (the hare) is typically reserved for shorter and more intense bursts of activity, with only a net gain of 2 ATP molecules produced using this system. In ME/CFS, the tortoise is sick, requiring the hare to do basic daily activities that should be covered by aerobic metabolism. Overreliance on anaerobic metabolism causes PEM.
In the example (Appendix 1), VO2 max didn’t tell the full story. The heart rate at the anaerobic threshold on the second day occurred at a mere 69 beats per minute (bpm). That’s the maximal heart rate this person could muster before hitting their anaerobic threshold and beginning to incur damage in the form of lactic acid accumulations, pain, fatigue, etc. That low heart rate indicated that one day after a short exercise test, there was little aerobic capacity left. Any moderate physical activity would put them over their anaerobic threshold.

The anaerobic energy production system (the hare) provides short bursts of energy that cannot be sustained. An inability to use the aerobic energy production systems for sustained activities, forces people with ME/CFS to use their anaerobic energy production system – resulting in pain and fatigue. (From By Tim Felce (Airwolfhound) – Hare, CC BY-SA 2.0, https://commons.wikimedia.org/w/index.php?curid=27813655)
For scale, the suggested target heart rate zone for exercise from the American Heart Association for a healthy 50-year-old person is 85-145 bpm.
Similarly, VO2 at the anaerobic threshold is 10.2 mL/kg/min, which presents a far more disabling picture because it places another low ceiling on the level that can be sustained.
In the general population, average V/AT occurs at about 63% of VO2 max in men and 58% of VO2 max in women. In ME/CFS patients, that number can be vastly lower. It is impossible to know the actual number without doing a 2-day CPET.
How metabolic responses translate to disability: The metabolic measures from the 2-day CPET come in handy for disability cases because they provide objective measures of how much work can be safely done in a day. For example, according to Workwell, the International Labor Organization considers 30% of VO2 max as the threshold for acceptable physiological demands over an 8-hr workday.
In the example (Appendix 1), VO2 max on day 2 was 21.7 mL/ kg/min, putting the acceptable amount of physical demand for a typical workday at about 6.5 mL/minute/kg (VO2 max x 0.3). This number can then be compared to the demands that different jobs and activities place on the human body. For example, showering takes 7 mL/ kg/min. ME/CFS patients are advised to not engage in activities that exceed their oxygen consumption threshold.
VO2 max can easily be converted to the metabolic equivalent (MET). The metabolic equivalent is a physiological measure of the cost of doing activities. One MET is equivalent to oxygen use at a rate of 3.5 mL/kg/min, which approximates the rate of energy expenditure at rest for a 40-year old man who weighs 70 kg. METs < 3 are considered light activities, METs between 3 and 6 are considered moderate levels of activity, and METs > 6 correspond to vigorous activities.
Using the example in Appendix 1, a VO2 max of 21.7 mL O2/kg/min could be expressed in METs by dividing through by 3.5 mL O2/kg/min, or 21.7 mL O2/kg/min ÷ 3.5 mL O2/kg/min = 6.2 METs in this example. Thus, the most a person with a VO2 max this low can do is moderate activity, keeping in mind that this is based on VO2 max, which corresponds with the peak activity that is attainable; most people with ME/CFS stay far away from that threshold. For ME/CFS patients, the relevant value is VO2 at V/AT, which is always less than VO2 max.
In the example, V/AT was 10.2 mL O2/kg/min. In this case, the corresponding MET value is 10.2 mL O2/kg/min ÷ 3.5 mL O2/kg/min = 2.9 METs, a substantially lower number. This value can be cross-referenced to the Compendium of Physical Activities to see the types of activities that are safe, given the upper value of METs that can be performed based on V/AT. Since many daily activities fall within the 3-5 METs range, ME/CFS patients may continually exacerbate symptoms associated with PEM by doing simple activities of daily living like brushing teeth, showering, or preparing a quick meal.
A limitation of the METs approach is that it does not account for age and body mass differences and does not consider the fact that some people have a lower level of fitness than others. Research has shown that METs underestimate energy expenditure from 12-22% in people with lower fitness. This is especially true in ME/CFS, in which impaired oxidative metabolism is the norm. Walking at 3 mph requires 4 METs and is classified to be a moderate-intensity activity, but to a person with ME/CFS such activity levels cannot safely be sustained (due to PEM) and can carry a heavy cost of recovery. For this reason, corrected MET values that account for age, weight, and gender are preferable when determining a safe level of energy expenditure for an individual.
VO2 and METs can also be matched against the New York Heart Association’s (NYHA) Functional Classification to determine disability according to how limited a person is during activity. Using these criteria, the data in Appendix 1 show moderate-to-severe disability.
Work in Watts
Work is measured in Watts (W), which is a rate expressed as energy per unit time. For example, a 100 W light bulb turned on for 1 hour will use 100 Watts/hour. A 50 W light bulb could remain on for 2 hours using the same energy. A human’s ability to perform work can also be thought of in this way. The average human produces/uses about 100 W (the same as a lightbulb!) in a day, with about 20% of this used to operate the brain.
Workload (in Watts) at V/AT provides a stark picture of how ill ME/CFS patients are. If it takes 100 W to power the human body, and the workload at V/AT is a fraction of that, it would show another aspect of disability. In Appendix 1, workload at V/AT ranged between 36 Watts on day 1 and 31 Watts on day 2, which is equivalent to very light housework. Ironing and cooking range from 35-44 Watts, suggesting that even these light activities are too demanding.
Cardiovascular responses
The cardiovascular data also provide insights about level of disability. As above, the V/AT represents the point at which anaerobic metabolism (and acidosis from lactic acid production) occurs. ME/CFS patients use the V/AT as a benchmark for pacing, with the goal being to spend as much of the day as possible below this value.
If you can’t do a two-day CPET you can use a multiplier (.6, .5, .4, .3 ) and then assess your response to get an idea of your safe heart rate using this formula: (220 bpm – age) x 0.6 or 0.5 or 0.4 or 0.3 = safe heart rate.
Although there are rules of thumb to help guide pacing decisions, the 2-day CPET is the only way to know actual V/AT and the change in V/AT between days 1 and 2. Using the example in Appendix 1, and applying a multiplier commonly used by ME/CFS patients (0.6), a 50-year-old’s AT would be = (220 bpm – age) x 0.6 = (220 bpm – 50) x 0.6 = 102 bpm. Actual AT, as measured by a 2-day CPET, was 69 bpm in the example – a far more disabling picture.
One way to approximate AT is to do the calculations using different multipliers (0.4, 0.5, and 0.6) and get familiar with how your body responds to exceeding each of these different thresholds. Many people learn to recognize symptoms that occur when AT has been crossed (e.g., dizziness, shortness of breath). If you are using an estimated AT of 100 bpm and feel horrible at 85 bpm, this might be an indication that the multiplier used is too high. Better safe than sorry.
Chronotropic insufficiency (CI): Another instructive measure from the 2-day CPET is the peak heart rate obtained during the test. In theory, the maximum heart rate (HR max) that can be achieved is estimated to be around 220 – age. A discrepancy between HR max and actual peak heart rate achieved during the test might indicate chronotropic insufficiency.
Chronotropic insufficiency is the inability of the heart to increase its rate commensurate with demand and is often expressed as the percentage of HR max that is obtained during a maximal exercise test. The ability to perform work depends on an ability to increase oxygen uptake (VO2) and is key to the ability to sustain aerobic exercise. Because the heart rate must increase dramatically during exercise in order to propel enough oxygen-loaded blood to the muscles for them to do their work, an inability to do that properly (CI) can be very disabling.

Chronotropic incompetence or the inability to get the heart rate up to speed during exercise appears to be common in ME/CFS
CI appears to be quite common in ME/CFS, as well as in patients with cardiovascular disease, and produces severe exercise intolerance in its own right, having nothing to do with disorders of the autonomic nervous system that are common in ME/CFS, such as postural orthostatic tachycardia syndrome (POTS), and neurally-mediated hypotension (NMH).
Interestingly, because patients are seated and moving during the CPET, the large rises in HR seen in POTS patients often do not occur during CPET testing, according to the Workwell Foundation. If anything, these patients have a weaker than predicted heart rate response, possibly due to chronotropic insufficiency. The Workwell Foundation is currently preparing a paper looking at CI in ME/CFS.
Respiratory responses
Respiratory responses during the 2-day CPET may also show different aspects of disability in ME/CFS patients. During exercise, CO2 builds up and ventilation (breathing) rate increases. As with VO2, the CPET measures VCO2, or the volume of CO2 exhaled per minute. Another measure, VE, or minute ventilation, is a measure of the O2 inhaled and the CO2 exhaled from a person’s lungs per minute. VE provides a measure of ventilatory efficiency and is measured in mm Hg (mm mercury).
One reason we breathe hard during exercise is to remove C02. Elevated breathing rates (VE) per the amount of CO2 present (VE/VECO2) in ME/CFS suggest that the lungs of people with ME/CFS are working overtime in an attempt to rid their bodies of the CO2 produced during activity/exercise.
VE/VCO2: VE/VCO2 is a measure of CO2 elimination. VE is modulated by CO2 and has a tight, linear relationship with VCO2. The slope of that relationship during exercise – also called VE/VCO2 – is used as an index of ventilatory efficiency. The normal range for the VE/VCO2 is 20-30; values above this are commonly found in ME/CFS. Elevated VE/VCO2 values are associated with diseases that have an increased ventilatory requirement for a given level of exercise or workload, such as heart failure.
Pet CO2 (partial pressure of end-tidal CO2): Pet CO2 is another valuable marker of disease severity and corresponds to the partial pressure (measured in mm Hg) detected at the end of exhalation, when CO2 is highest. Values <40 mm Hg are low and values <30 mm Hg are very low. Low Pet CO2 may be an indication of hyperventilation, decreased cardiac output, or poor pulmonary blood flow and should be assessed.
Low Pet CO2 is associated with orthostatic hypocapnia in ME/CFS.. Hypocapnia is the term for low CO2 in the blood and is caused by deep or rapid breathing (hyperventilation). A retrospective study found evidence for orthostatic hypocapnia in a subset of ME/CFS patients, caused by hyperventilation upon being tilted upright in a tilt table test. This is yet another form of orthostatic intolerance that contributes to the disability picture found in ME/CFS patients.
Conclusion
Each of the variables measured in the CPET provides an opportunity to compare a patient’s values against that which would be predicted based on the general population. The drop in functional capacity between day 1 and day 2 presents a stark, and often bleak, picture for many ME/CFS patients.

Most people with ME/CFS recover from a two-day CPET within a week but others can have much more difficult time. Getting a saline IV may help.
The value of the test is two-fold. First, it provides irrefutable and quantitative evidence on the functional capacity of a person, and thus their ability to perform work. Second, the metabolic, cardiac, work, and respiratory measures provide actual (vs. theoretical) benchmarks for pacing. VO2 max, METs, and workload at V/AT all offer ways to deepen our pacing efforts. We likely know the types of activities that cause us to crash, yet do them anyway. By understanding how activities are classified in terms of corrected METs, Watts, or VO2, patients can better learn how to avoid activities that are all but certain to lead to PEM because such activities will likely invoke anaerobic metabolism.
Ultimately, it is a very personal choice for an ME/CFS patient to either choose or forgo a 2-day CPET for disability purposes. Many patients report permanent losses to health following a CPET, yet many more appear to recover eventually, with 50% of Workwell patients recovering within 1 week. It is hard to predict who will recover and who will not. Just like with any treatment advice, we are all different and ultimately cannot predict how our bodies will respond to an extreme stressor like the CPET.
Some people bristle at the idea of calling the 2-day CPET a biomarker for ME/CFS because it is unethical to ask patients to knowingly cause harm to themselves. Hopefully, with the advent of a more straightforward biomarker, like a blood test, the 2-day CPET may not be required to win disability cases in the future. However, given that the CPET provides direct measures of functional capacity, it would stand to reason that the utility of the CPET to ME/CFS patients is not going to lessen anytime soon.
FAQ
Many patients have abnormal results that show up on day one. Can the test be stopped at this point and still be used to demonstrate disability?
Patients with a very low VO2 max and V/AT may have the numbers to demonstrate disability (Table 1). However, many patients have found that their results from a 1-day test were dismissed as deconditioning, while others have succeeded in being awarded disability with a 1-day test, presumably because VO2 max was very low and/or there were other factors that helped with their case.
A second test is necessary to document the atypical recovery response and prolonged fatigue associated with PEM. This information shows the lack of ability to sustain work.
Couldn’t the CPET be adapted to be done from bed, especially for severely ill patients, who might reach their anaerobic threshold upon rolling over?
For the CPET to be valid it must be a maximal exercise test. This is not possible while in bed. A maximal test is required for VO2 max and to ensure V/AT has occurred during the test. These variables form the basis for assessing functional capacity and therefore disability.
I did an exercise test at my cardiologist’s office recently. Couldn’t I use the results from that test rather than putting myself through a 2-day CPET?
While a stress test provides valuable information about certain heart conditions, it is not considered a maximal exercise test and therefore VO2 max and V/AT cannot be derived. A 2-day CPET is required to capture the drop in function that is often seen between days 1 and 2.
Is a test invalid if patients arrive already in PEM from the stress of travel?
PEM will lower the anaerobic threshold, so the starting point might be lower than it would be when not in a crash. However, repeating the test often yields a significant drop in function, even though the starting place was low to begin with.
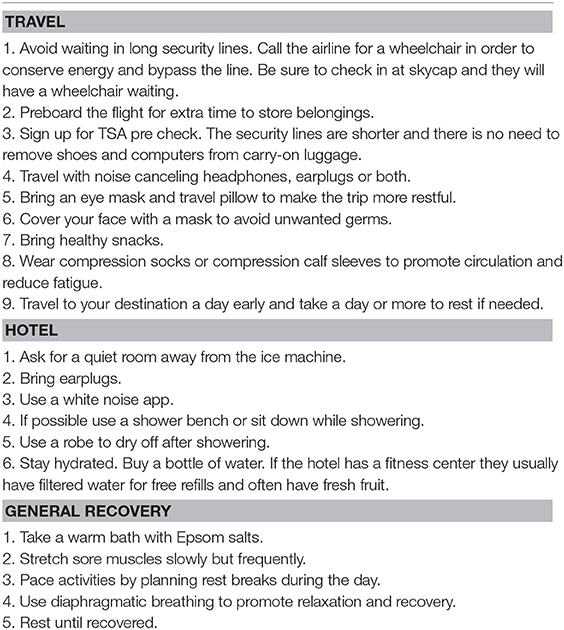
What is the best way to prepare for the test?
The best information on how to prepare for the 2-day CPET comes directly from the Workwell Foundation.
https://www.frontiersin.org/files/Articles/386825/fped-06-00242-HTML/image_m/fped-06-00242-t002.jpg
What is the best airport to fly into?
Sacramento is the closest airport, but San Jose and San Francisco are within 3 hours of Ripon, CA, where the Workwell Foundation is located. However, it is always a good idea to double check where your test is scheduled; higher-risk cardiac patients are required to do their test in Newport Beach, CA, where an MD helps to oversee the test.
How long do I need to stay for the test?
A minimum of 2 nights is required, and it would be wise to arrive the night before (to minimize PEM on day of test) and to stay the night of the second test, and possibly a third, depending on travel distance. Patients are not allowed to drive themselves after the test.
How can I help speed up my recovery?
In addition to the information from Workwell on how to best prepare for the test, they also recommend that patients arrange for IV saline after the test. Saline can still be beneficial even if administered a few days after the test, when PEM really sets in.
How have other patients responded to a 2-day CPET?
Everyone responds differently to the CPET, but it is still worth exploring other patients’ experiences.
Where else can I get a 2-day CPET besides Workwell?
There are a few places that use the same or similar methodology as Workwell, including Betsy Keller at Ithaca College and Laura Black at Hunter-Hopkins Center in North Carolina. Other sites can be found here.
The Workwell Foundation and colleagues recently published a paper outlining their methodology for assessing ME/CFS patients with a 2-day CPET. This paper could be shared with sports medicine physiologists, or others who perform CPET testing, to inform them of how the 2-day test is done for ME/CFS patients. Workwell uses methodologies that adhere to cardiopulmonary testing standards established by the American College of Sports Medicine.
Acknowledgements: Deep gratitude to the Workwell Foundation for being champions of the ME/CFS community and Staci and Jared Stevens for their contributions to this article. Many thanks to Cort Johnson for his excellent editing suggestions.
More on Workwell from Health Rising:
- The Disability Defenders: The Workwell Foundation, Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia
- How Physical Therapists are Getting it About Chronic Fatigue Syndrome (ME/CFS): The Workwell Foundation Pt. I
- The Workwell Foundation Resource Page for Chronic Fatigue Syndrome
Caroline’s Health Rising Articles
- Learn more about Caroline and check out more Health Rising articles from her here.
Appendix 1. Sample 2-day CPET report.
Cardiopulmonary Exercise Test (CPET) Evaluation Report
Findings:
Patient demonstrates cardiopulmonary anomalies*, low function and delayed recovery with severe symptom exacerbation post-exertion. This will severely limit the patient’s ability to engage in normal activities of daily living and precludes employment of even a sedentary/stationary nature. *Treating physician please take note.
Indications:
The patient was referred to our lab for global functional evaluation examining metabolic, cardiovascular and pulmonary function after experiencing physical stress. The patient underwent a cardiopulmonary exercise test-retest over a two-day period. She is 50 years-old, 69 inches tall and weighs 117.4 pounds.
Procedure:
The patient performed symptom limited 10 W/min ramping protocols on a bicycle ergometer while expired gases were collected for determination of oxygen consumption, carbon dioxide production and pulmonary ventilation. Two exercise tests were performed on consecutive days. The heart rate, blood pressure and arterial oxygen saturation were assessed throughout the tests. Appropriate measures were taken to calibrate and test the accuracy and reliability of the testing equipment on both days. These tests were performed to determine functional capacity and assess the recovery response to a standardized physical stressor.
In the fields of exercise science and medicine, cardiopulmonary exercise testing (CPET) is considered the gold standard for measuring and evaluating functional capacity and fatigue. Position statements and/or guidelines for the performance of this testing are available from the American College of Sports Medicine, American Heart Association, American College of Chest Physicians, American Thoracic Society and the American Medical Association, among others. All endorse this method of testing and acknowledge peak oxygen consumption, only available with CPET, as the most accurate measurement of functional capacity. Workwell Foundation has adopted this standardized, reliable and accurate tool to evaluate disability in fatigue-related disorders.
Conclusions:
(1) Assessment of Effort: Normal
The patient was cooperative and there is no evidence of malingering. Respiratory exchange ratio (RER) and rating of perceived exertion (RPE) values met criteria for maximal effort on both tests. Cardiopulmonary exercise testing provides objective measures that can clearly distinguish between indolence and true disability. See page 4, #1 Assessment of Effort.
2) Metabolic Responses: Abnormal
Peak and submaximal oxygen consumption was abnormally reduced between tests (11%, 16%). Day to day test variability for metabolic processes is less than 8% for healthy individuals. Abnormally high variability for these measures indicates a disruption of homeostasis during physical activity. Test 2 measured value for oxygen consumption at the ventilatory/anaerobic threshold indicates severe to moderate disability using the Weber/New York Heart Association criteria. See page 4, #2 Metabolic Responses.
3) Workload: Abnormal
Submaximal workload was abnormally reduced between tests (14%). This indicates a diminished capacity for activity post exertion. Submaximal workload of 36 to 31 watts is equivalent to light housework activities such as ironing or cooking which range from 35 to 44 watts. See page 4, #3 Work in Watts.
4) Cardiovascular Responses: Abnormal
Peak heart at only 71% to 65% of predicted value may indicate chronotropic incompetence. Diminished maximum heart rate is a significant functional impairment. Certain patient medications may affect heart rate. See also Respiratory Responses below. See page 5, #4 Cardiovascular Responses.
5) Respiratory Responses: Abnormal
Values for exhaled carbon dioxide were reduced, i.e., low PetCO2 (<40 mmHg) and elevated VE/VCO2 (>30). These measures show impaired ventilatory efficiency and are considered indicators for chronic metabolic acidosis, and/or cardiovascular disease, and/or pulmonary disease. Low exhaled CO2 levels can also be indicative of orthostatic hypocapnia. See page 5, #5 Respiratory Responses.
6) Recovery Response: Abnormal
A recovery time of 24 hours or less and minor muscle soreness is considered normal following exercise testing. This patient’s recovery time of 7+ days along with excessive fatigue and symptom exacerbation should be considered an extreme reaction to physical activity. See page 5, #6
Results:
- Assessment of Effort
The American Heart Association cite peak respiratory exchange ratio (RER) as the most accurate and reliable gauge of subject effort during cardiopulmonary exercise testing. A peak RER ≥1.10 is generally considered an indication of excellent patient effort. An RER between 1.0 and 1.09 indicates good effort.
| Test Criteria | Test 1 | Test 2 |
| RER >= 1.10 | 1.19 | 1.17 |
| RPE >= 17 | 20 | 20 |
RER = Respiratory Exchange Ratio
RPE = Rate of Perceived Exertion
- Metabolic Responses
| Peak Values | Oxygen Consumption
(mL/min) |
Oxygen Consumption
(mL/min/kg) |
Percent Predicted
(%) |
| Test 1 | 1299 | 24.4 | 95 |
| Test 2 | 1158 | 21.7 | 84 |
| V/AT | Oxygen Consumption
(mL/min) |
Oxygen Consumption
(mL/min/kg) |
Percent Predicted
% |
| Test 1 | 651 | 12.2 | 47 |
| Test 2 | 543 | 10.2 | 40 |
| mL/min – milliliters per minute
mL/kg/min – milliliters per kilogram per minute V/AT – ventilatory/anaerobic threshold (determined using V-slope, ventilatory equivalents, and end-tidal pressure methods) |
- Work in Watts
| Workload | V/AT (W) | Peak (W) | Percent Predicted
% |
| Test 1 | 36 | 103 | 113 |
| Test 2 | 31 | 89 | 98 |
W – Watts
V/AT – Ventilatory/Anaerobic Threshold
- Cardiovascular Response
| Heart Rate | Resting seated
(bpm) |
V/AT
(bpm) |
Peak
(bpm) |
Percent Predicted
(%) |
| Test 1 | 67 | 76 | 121 | 71 |
| Test 2 | 64 | 69 | 111 | 65 |
| Blood Pressure | Resting Seated
(mmHg) |
Resting Supine
(mmHg) |
Peak
(mmHg) |
| Test 1 | 94/68 | 108/78 | 170/88 |
| Test 2 | 118/80 | 112/92 | 174/90 |
- bpm – beats per minute
- mmHg – millimeters of mercury
- V/AT – ventilatory/anaerobic threshold
- Respiratory Response
| VE/VCO2 | PETCO2
(mmHg) |
VE
(L/min) |
VE % Predicted | |
| Test 1 | 35 | 34 | 59.1 | 45 |
| Test 2 | 34 | 34 | 59.0 | 38 |
|
- Recovery Response
A post exercise test log was maintained by the patient. Following testing the patient experienced profound fatigue, weakness, difficulty walking, dizziness/lightheadedness, nausea, pressure headache, increased thirst, burning sensation in limbs and head, erratic heart rate, and cognitive difficulties. Patient was not recovered 7 days post-testing.
Summary:
The patient’s low peak oxygen consumption, reduced oxygen consumption at the ventilatory/anaerobic threshold (V/AT)* and symptom exacerbation post activity indicates significant impairment. Energy expenditures at, or close to the V/AT represent vigorous activity and can be sustained for only short periods of time. The International Labor Organization regard 30% or less of maximal oxygen consumption (VO2 max) as the threshold for acceptable physiological demands over an 8-hour work day. Estimated energy expenditures for most occupations and life activities can be found in the Compendium of Physical Activities.
Based upon a test 2 measured peak exercise capacity of 21.7 ml.kg-1.min-1, the safe limit for sustained activity is an oxygen consumption of around 6.5 ml.kg-1.min-1. The estimated oxygen requirement for seated office or computer work is 5.25 ml.kg-1min-1. However, even sedentary work involves more than just sitting at a desk. For normal office tasks, the energy cost rises to 10.5 ml.kg-1.min-1 which is above the V/AT. Driving to and from work would require 8.75 ml.kg-1.min-1 of oxygen. In addition, every day activities such as showering (7.0 ml.kg-1.min-1) or making the bed (11.6 ml.kg-1.min-1) represent significant energy demands. The patient should limit activities requiring oxygen consumption above 6.5 ml.kg-1.min-1 and avoid, if possible, activities requiring oxygen consumption beyond the test 2 V/AT of 10.2 ml.kg-1.min-1. Maximal heart rate should not exceed 69 beats per minute. Energy expenditures at or close to this level will likely result in symptom exacerbation and delayed recovery.
Even a sedentary job would require more energy than can be safely sustained.



{kind=link}
{kind=link}
Thank you, Caroline. Yours is an excellent article that describes the 2-day CPET, discovered by Staci Stevens, very well. It’s such a complex subject and you have really done it justice. The importance of the 2-day CPET to the ME field -researchers, physicians and patients – cannot be underestimated.
Worth noting that Jennie Spotila has a full–and very scary–account of her 2 day CPET on her OccupyME blog site.
Check out all sorts of resources on the two-day CPET, exercise testing in ME/CFS, exercise and pacing in Health Rising’s Exercise Resource Center – https://www.healthrising.org/forums/resources/exercise-resource-center-for-chronic-fatigue-syndrome.168/
1) Does insurance typically pay for this test? If so, for what ICD10 codes and under what conditions?
2) Even though we are all excited to use this for our disability claims, it seems like it’s an excellent opportunity to collect. Blood and urine before, during and after, to measure changes in cytokines, oxidative and nitrosative stress and depletion of other metabolic resources, like amino acids, B vitamins, antioxidants, NAD+, and NAD+/NADH ratio, Krebs cycle metabolites, and markers of inflammation which might inform the treatment process, so we can get well?
I suspect there would be severe metabolic abnormalities that wpuld become evident, that replenishing metabolites or positively altering biochemical pathways might change the Day 2 (or Day 3) results and not damage people.
Kaiser Permanente wouldn’t do a 2 day CPET to prove disability. Kaiser also stated they do not fill out SSDI paperwork for “CFS”, necessitating paying out-of-pocket to see an out-of-network doctor just to apply for SSDI.
I thought it was just my doctor at Kaiser, but I guess it’s the whole Kaiser system. She wouldn’t fill out any paperwork.
I have a friend with a Kaiser doctor who did but maybe he was just super caring and did the extra work on his own.
I guess I need to find an outside doctor
Such a great idea Learner. From talking to them I believe that Workwell would just love to start having people get on the bike – work them up – give them an intervention – and then see if that improves how they do.
What a great idea!
Does anyone know if this the same diagnostic testing that is performed by Dr. David Systrom at Brigham and Women’s Hospital in Boston?
I am wondering the same thing 65String. My daughter will be seeing Dr. Systrom next week for a 1-day physical test and muscle biopsy. Are the physical tests similar or approach a different set of observations?
If you feel comfortable please let us know how it goes. Dr. Systrom is, I believe, one of the key people helping us understand this disease. We are very lucky to have him and I’m sure your daughter will get a lot of interesting information 🙂 Congratulations on getting her in there.
6String,
No,this is a different test. Systrom’s test is a one-day invasive CPET (iCPET). Catheters are inserted into the radial artery in the wrist and into the pulmonary vein in order to allow him to measure blood pressures in various parts of the heart and circulatory system, as well as oxygen extraction in the muscles. Systrom’s goal is really to identify the underlying physiological causes of exercise intolerance in ME/CFS and to try to treat it. His focus is not on documenting disability. I think his test can be used to prove disability if the results are severely abnormal, but it might not be that helpful in patients who are only mildly or moderately ill. A lot of disability lawyers seem to prefer the 2-day CPET, although maybe in part because they are more familiar with it than with the iCPET.
The 2 day is different from the CPET-3 done by Dr Systrom. The CPET-3 includes catheter into the heart to monitor the blood flow while the 2 day uses blood draws. Both provide information explaining how the person’s body is not functioning normally. The 2 day test provides a Target HR which is very helpful with pacing. In combination, medications and pacing may help you feel better by avoiding PEM
Not to mention that the invasive CPET costs 30K! (I just asked :))
I don’t think so. Similar but not nearly as intense. My test w dr David starring is coming up in July. It’s only a 3 hr test not two days. Not nearly as involved or intebse
I am 98% bedridden and gradually ill for 31 years. With not ruelling out everything at the time I got ill, I -so ill as I am now and hearing that some patients have found out after years that ME/cfs was a wrong diagnosis- find it “cruell” that I am for so long no longer able to do a 2 day excercise test to know for shure that I have ME/cfs. Also I could use the treshold off hartrate so much to stay under it because I still get worse and worse.
Also, just a one day test, for ruling out heart or lungproblems is for me sadly impossible. I notice more and more, even lying down in bed, that periods my heart beats to slow and suddenly beats to fast or to hard. I often also have no energy to breath properly in my muscles. I can even not see a cardiolist or someone for the lungs for that. Has anyone bedridden for decades, have the same experience of the to slow hart rate and then to fast even just in bed? And the no strenght to breath at times? Has anyone any idea what to do? I feel hopelous with my problems to even not being able to see a specialist. A hospitalisation, there am I much to ill for.
Has anyboddy any idea at what heartrate I should stay under because I did not understand it how to count it(am way to ill)
thank you!
“to fast even just in bed? And the no strenght to breath at times? Has anyone any idea what to do?”
I am not bedridden. But I often have very high (very probably over 150 or even over 180 bpm, too fast to count manually) hart rate late at night / early morning when in bed.
What helps me is:
* doing circulation exercises
* get up and sit for 15 minutes
* lay myself on my side with the hart on the lower side
All three can get my hart rate with fairly good repeatability to a low 60-70 bpm in something between !5 seconds! to 15 minutes and maintain so for 30 minutes up to 2 hours. In your condition only the last method may be realistic. If you try please report results. I already had feedback from others saying it can stabilize too high hart rate.
“I often also have no energy to breath properly in my muscles.” I had that sometimes too at my worst. I agree it’s a very scary feeling. By getting slowly better, doing classic breathing training (only very small and low effort series a day but repeated over more then a year) with a physical therapist AND by only increasing effort breathing while in deepest need breathing got slowly better over time.
Only increase effort breathing while in deepest need, and not when one “just” has a lack of breathing, may seem a bad idea. But consider it “breathing pacing”: keep some reserves in breathing even if it is too short for normal functioning in order to have some reserves and avoid the very costly and disastrous “deep breathing failures”.
Wish you the very best!
thank you for your suggestiond de jurgen! I also think like you that it is because I am so ill.
with the breathingtraining I would like your opinion. I get from every “exercise” a muscle weakness.But I thought at maybe on my bed yogabreathing. But then I thought, what if they go to far (with an instructor) and I get also provoced muscle weakness in my breathing muscles.
would you try yoga breathing for that?
I certainly would let you know about heartrate or anything. And yes, it is in my bed 🙁 to slow or to fast.
thank you for your reaction!
de jurgen. did you also have the change whith the mutch to slow heart beats and then on the other hand the to fast?
may I ask you how you did get better? I am only getting worse and worse, do not know where it stops.It was 31 years like a siral downside. I do not know what to do anymore.
with my hertbeat, I even get it just turning around in bed that it skipps or flatters or so.
thank you very much!
“I get from every “exercise” a muscle weakness.”
I am lucky to have found a good and intuitive physical therapist that takes my feedback into account.
The therapy started with her trying to explain how I could improve my breathing and what I should be aware of when I get it wright.
I only get one type of breathing very good now: diaphragm breathing. At the beginning I wasn’t even able to move my diaphragm the least bit. Luckily she could explain it in a way I could visualize, something that works well for me.
The early “exercises” were sometimes no more then to try and get a breathing wright 5 times. And do so only a few times a day. She especially warned that doing more may not yield better results. The goal was “to get a feeling of breathing more efficient” and “let it sink in my unconsciousness so I would start to do it more and more automatic.
After three months of daily training I got the hang of it. She said I proved to have great body awareness as I picked it up really fast. After a year I could breath slower then she can she claims. But I still can only do this diaphragma breathing good and fail at all other breathing techniques. Luckily for me (and many others) it is the most efficient “base line” technique for low energy activities.
So it kinda takes more commitment (and some mental ability to focus/adapt) then muscle power and endurance. One has to breath anyways. A slow, small and efficient exercise will do and be better then to try and learn a new technique while trying to max breath in and out. So IMO it’s very low access IF you find a good PT.
“did you also have the change whit the much to slow heart beats and then on the other hand the to fast?”
I *think* I sometimes hit 50 – 45 – 40 bpm but in a “solid” way, I do not feel it to be weak and problematic. It’s very rare and only when I am pretty good.
It however remembers me of something else: when I barely can move my chest to breath I have an “adrenaline collapse”. Then I somehow cannot panic, be afraid nor angry nor anxious despite alarming circumstances, even if I try. It could be temporal adrenal insufficiency/exhaustion or what Veronique Md suggests is the brain powering down the adrenals in order to let me hibernate.
-> Does collapsed breathing go hand in hand with this (lack off fear/anxiety…) and poor hart beat?
If so, going from too low to too high hart beat (and reverse) may be adrenals being unable to push you trough to adrenals getting out a high amount of adrenaline to drag you forward a bit further.
“may I ask you how you did get better?”
I’m slowly writing a “Me current improvement” series on the forum where I try and explain what works for me. No guarantees it’ll work for someone else! I hope to be able to add a bit over one topic a week.
I’m completely bamboozled by this article. What type of specialist would I need to show this to, in order to get a layperson summary. Even the numbered points at the end are not within my understanding.
I have used an Exercise Physiologist in the past, but I’m not confident in their openness to this sort of thing.
Would a general practitioner/MD have sufficient knowledge?
Exactly ManShadow. I had this test done at Workwell in 2014 with worse numbers than in this article. I have seen pulmonologists, rheumatologists, cardiologists, etc., at best they ignore it. Most comment on it as if it were a one day test and move on.
I think you would need a good cardiologist or exercise physiologist or a ME/CFS MD who is interested and willing to learn. Really, this should easily be within the realm of understanding of an MD – if they’re willing to learn. I think that last part is the key – if they’re willing to engage with this stuff…
OK. Well I might run it by my MD then. Although, after reading of the lengthy recovery times and non-recovery of some PWME after a 2-day CPET, I think I’ll stick with trying to going back to work first.
It is such difficult subject matter. Even Staci Stevens says that they continue to learn so much from CPET and, as she told me, “it is that simple, and it is that hard.” Or something like that.
My experience has been that most MDs I have encountered do not know how to interpret a CPET. Same with lawyers. Sadly, the two most important types of people we need to understand these reports! I have the good fortune to be working with a very talented attorney, who also works closely with Workwell, and he confirmed that he knows more about CPETs than most doctors he deals with, so that is saying something. And he is someone who set out to understand these reports and how to use them to win cases for his clients, so I trust his experience.
My piece was an attempt to provide patients with the tools to better understand their own CPET reports. The piece would be quite a slog for someone who does not have one in hand (though I provide a sample so people can follow along with their own). It is essential that we know what these reports are saying so that we can make sure our doctors represent the results in an accurate way and to make sure that all of the features of disability that turn up during a CPET are used as evidence in a case.
Or, if not for disability purposes, the CPET can still give us invaluable information about our health (or lack thereof!). For example, it might indicate an underlying health condition that can then be followed up with a doctor. And, of course, it provides invaluable pacing information. I am in no way suggesting that people go out and get a CPET, but if you’ve had one done, it is super useful information.
I will give you the advice my attorney gave me – make sure that whoever gets your CPET report also gets this recent paper from Workwell and colleagues. Cort so kindly did a summary of this article late last year. A peer-reviewed article will carry more weight than what I wrote. My piece is meant to serve as a bridge between a scientific article and understanding an individual’s CPET report. I could also see it being helpful to a doctor who is wanting to better understand how the various measures translate into disability.
https://www.frontiersin.org/articles/10.3389/fped.2018.00242/full
Cort’s write-up on this piece:
https://www.healthrising.org/blog/2018/11/19/workwell-cpet-deconditioning-dilemma-chronic-fatigue-syndrome-me-cfs/
I will work to create a companion document that distills some of the many points I raise in the article, but there are several articles out there that explain the general gist of CPET.
Thanks for the extra info. It is encouraging to know this data can be of use in the right hands. The HR guide also sounds like something I’d love to have. It’s just that I’m too scared of PEM and the possibility of slipping back to moderate or worse. And a couple weeks ago I was sure I was ready for part-time employment. Then I carried my 25kg dog for a minute or two…. Whoops!
So I guess if this latest round of treatment doesn’t help me get back to work, then my desperation will likely be enough to try the CPET route. On that note, is there a source of info that outlines the currently known best practices to avoid or reduce PEM? Sounds like the saline drip is a good thing. Is there anything else?
For those who found this piece a bit difficult to read and absorb, I wrote a “CPET lite” article that might be a little easier to follow 🙂
https://chronicallycaroline.com/category/uncategorized/
Caroline- would you mind sharing your talented attorney’s name?
Question right off the bat: do you know how they measure V/AT? Do they prick finger every minute to check lactate level?
This is an excellent and very useful article, thanks. Not just for the purpose of disability, which is HUGE obviously, it could shed some light as to what’s going on with CFS. An illness decreases VO2Max, and so does overtraining. I wonder if a concussion fatigue in an athlete immediately decreases VO2Max too. Some concussions trigger microglial over-activation and CFS-like fatigue.
Using AT heart rate as the pacing parameter may work for some/most patients, but I don’t think lactate buildup is not the cause of PEM. Severely ill patients can suffer from PEM by simply walking from the bedroom to bathroom. Even for some moderate cases, squatting a couple of times can trigger PEM. There should be enough oxygen/glucose in the bloodstream to power 20 feet walk or 2 squats, lactate should not be an issue. I think there is something else going on in CFS that makes a minimal exertion equivalent to an overtraining.
I believe the low VO2Max, V/AT and strong lactate buildup may not be what it seems.
I believe all of them could mask a very early and strong shifting from Krebbs cycle and glycolysis for producing NADH/ATP towards the PPP producing NADPH and ATP.
It would make sense in a disease with very strong body wide baseline oxidative stress. Allowing the Krebbs cycle to speed up will create plenty additional ROS. In a disease with said chronic high oxidative stress that will reduce stocks of anti-oxidant to very minimal even at rest. The smallest exertion will create a massive unbalance and that oxidative stress will go near unchallenged and create devastation.
If so, the logical solution is to turn down NADH/ATP production as much as possible by turning down the Krebbs cycle and shifting production of every part of the Krebbs cycle that can produce either NADH or NADPH towards NADPH.
Then, fire up the PPP very high in order to produce combined ATP and NADPH. NADPH is needed to recycle vital anti-oxidant glutathione that would be needed in huge quantities if the hypothesis is wright.
It’s actually not the PPP that produces ATP but the PPP “intermingles” with part of the glycolysis pathway to produce glucose-6-P and some ATP on the side.
It is IMO this strong interlink between PPP and glycolysis that makes it *very* hard to distinguish between both. As very few assume that the PPP can become so dominant under certain situations it may be wrongly believed to be anaerobic functioning as in “full glycolysis”.
The picture changes though, as you move into moderate/mild phase. When you stay within your limit, you recover from the post-exercise fatigue, presumably from metabolic/oxidative damage, within 24 hours or so. It’s a fantastic fatigue disproportionate to the exertion, but you recover nonetheless. It is when you go over the bright red line that you get hit by a bus almost exactly after 24 hours for some patients and struggle for days. Not sure how massive oxidation alone could account for that.
The early lactate buildup could be just another symptom common to all central fatigue, possibly from glycolysis/ppp switch as you said. That’s why I’d be interested to know if people suffering from concussion fatigue or overtraining syndrome exhibit similar V/AT anomaly.
“you get hit by a bus almost exactly after 24 hours for some patients and struggle for days. Not sure how massive oxidation alone could account for that.”
IMO the un-counteracted strong oxidative stress assault is such an aggressive emergency that the body depletes anything that can produce anti-oxidant. That includes glutathione, building blocks for making glutathione (note that many amino acids are very low in ME according to metabolics), and proteins for glucose harvesting (potentially for fueling the PPP pathway).
This makes restoring from this “oxidative stress assault” slow. As long as oxidative stress remains high and problematic energy production will remain low but also NO will be massively reduced by oxidative stress. Also, probably hundreds of biochemical pathways get blocked by high levels of oxidized glutathione. There are plenty of pathways described in which oxidized glutathione acts as an inhibitor). So the blood flow and many key biochemical pathways should be derailed for hours. Having a derailed blood flow also derails breathing and that is on top of an already impaired breathing / oxygenation “normal” capacity.
What’s worse, having hours lasting too high oxidative stress while having depleted oxidative stress defenses, the RBC act as a last line of defense binding to hydrogen peroxide and ROS. That’s a described reaction. Problem is, for every single molecule of peroxide bound this way 3 more positions of oxygen are very firmly locked (oxygen binds so hard it does not release), making for a total of 4 positions for carrying oxygen that are unavailable for every molecule of ROS bound to RBC. Releasing that ROS from the RBC is a slow process that requires plenty of “over-breathing” or bathing the RBC in copious amounts of air (air hunger).
And then there comes the night, a moment where blood flow and breathing naturally goes to low gear even in healthy people. When it’s already low in ME patients on normal days you start the night severely damaged in this area when overexerting that day IMO. And as the night passes it only gets worse. That makes for (at least with me) even (a lot) more problematic nights then usual.
In order to save breathing and blood flow to the brain, the body produces increasingly high amounts of adrenaline to keep this at minimum levels. At the very least during such nights my adrenaline levels go sky high.
That makes one wake up very unrefreshed, with plenty of damage and waste to clean up, very low reserves of anti-oxidant and still recovering blood flow. Doing any activity soon gets too much, even just resting. Where adrenaline (and nor-adrenaline and cortisol) would get you trough the day (and normal days, we are fight or flight people) now you have far lower levels of each of these due to over usage during the night. The adrenals need a break. And when the adrenals of an ME patient take a brake, he feels like shit.
That’s just my guess on it. I do appreciate your take on it too and hope to learn from you when you get further taking that route ;-).
“And as the night passes it only gets worse.” My night time experience is quite interesting (to me at least). There are times I wake up completely fatigue-free and ache-free after 5 hrs of sleep or so, I would go “this is how recovery feels like!”. I go back to sleep and then, by the time I wake up, I am the usual fatigued/achy person. Other times, probably 2-3 hours into sleep, I am overcome with unbelievable ache/fatigue, I’d be literally quaking under the comforter.
My explanation has been that the inflammation ebbs and flows during the sleep. Repair is one of the key function of the sleep and it’s known that inflammasome is a key regulator of sleep. So it’s possible that the inflammation spikes at certain stages of sleep and then completely subsides in different stages, resulting in what I have observed.
My sleep also has been mostly refreshing, usual amount of fatigue and ache notwithstanding, except when I’m suffering from PEM, for the past a few years. I no longer wake up dazed and groggy. It’s really the PEM and hypersensitivity to exertion that’s been stubbornly remaining and therefore limiting my ability to less than 20%. And this changing pictures is why I think researchers should include more on moderate/mild patients instead of solely focusing on severely ill. The wider perspective could give them more clues and keep them from mistaking CFS for something else.
Your imagination is fodder for thought as always. I do learn from it while trying to wade through the thickets of the processes you describe. 🙂
Hi Caroline, Good to see you again on healthrising! What has been the outcome of your treatment with Dr. Carroll for CSF leaks? After I read your blog on leaks, I set out trying to get in to see Dr. Carroll too, was also diagnosed with a pretty big leak, and I’ve had 3 patches. I’m now wading through months of rebound intracranial hypertension. I’ve always wondered how you turned out, how much relief of symptoms you got, what your treatment journey looked like. And thank you so much for that leak blog. Before reading it, leaks weren’t on my radar at all. Thanks again and best wishes.
Thank you for all of your effort (and certainly PEM!) for pulling this together, Caroline. I’m sharing it with a new physical therapist, so pleased that she’ll see the level of knowledge patients share with each other, and that the links to studies referenced are all here. When meeting a new health provider, it’s easy for them to think that the information we share through social media is on the level of “exercise is good for everyone!” I love that articles like this and all that Cort presents on HealthRising show the amazing level of scientific knowledge patients have attained in order to move the bar forward for themselves and the community. I know that you’re a scientist by training, Caroline, so understanding the complexities of this subject may come more easily to you than me for sure, but your passion for it shows how much you’ve embraced this path of loss and change. Once again I am in awe. Thank you.
Thank you for putting this information together. I was wondering if you can provide a reference for this section from the sample report?
“However, even sedentary work involves more than just sitting at a desk. For normal office tasks, the energy cost rises to 10.5 ml.kg-1.min-1 which is above the V/AT. Driving to and from work would require 8.75 ml.kg-1.min-1 of oxygen. In addition, every day activities such as showering (7.0 ml.kg-1.min-1) or making the bed (11.6 ml.kg-1.min-1) represent significant energy demands. ”
I would like to be able to use this information, but need a source? Thank you.
Hi Karla! Yes, I can provide you with a source! The numbers come from the Compendium of Physical Activities.
https://sites.google.com/site/compendiumofphysicalactivities/Activity-Categories/transportation
It is a cumbersome website, but you’ll get the hang of it.
But you have to do a little work first. The Compendium lists the costs of activities in METs. This is why I included all of that information in my piece because we need to be able to move back and forth between VO2 (oxygen consumption) and METs.
To get METs from VO2, simply divide the VO2 by 3.5.
Conversely, to convert METs to VO2, multiply the METs value you see in the Compendium by 3.5 to get the corresponding VO2 value.
I much prefer to work in VO2 units because it is a direct measurement. METs worry me a bit because they standardize everything based on males who are of middle age and reasonably healthy. This is why I included the bit on corrected METs, but the formula I include in that link is no fun to work with, trust me. But, in theory, you have all of the data in your CPET report to calculate what your corrected METs are. But for the sake of simplicity and to answer your question, use the back-calculation above with the values in the Compendium.
Let me know if that doesn’t make sense I can try to elaborate further!
One other thing – did you know that you can get your full data from Workwell (assuming that is where you had yours done). Guessing the other labs would provide the data as well. If you want to geek out more on your data, I suggest you request it. Good luck!
Hi Caroline,
Thank you for your reply.. I have looked through the Compendium, and whilst it is useful, I don’t understand how you’ve arrived at the specific energy costs you’ve used.
I understand that sedentary work involves more than sitting at a desk, but I can’t find anything in the Compendium that indicates it would be an energy cost of 10.5 ml.kg-1.min-1. From my reading, desk work is 1.5 METs, or 5.25 ml.kg-1.min-1. Whilst it obviously incorporates more than just siting at a desk, I haven’t been able to find activities listed that reflect this. So I’m interested to know how you arrived at this figure – what else has been included, and what is the logic for the inclusion?
Or have I missed something obvious? Thanks again.
Hi Caroline,
Thanks so much for your reply – I’m very sorry, because I don’t think I articulated correctly what I wanted the source for.
You stated that sedentary desk work is more than sitting at a desk, and that the energy cost of this would be 10.5 ml.kg-1.min-1.
Given the Compendium lists this as a 1.5 MET activity, this would then equal an energy cost of 5.25 ml.kg-1.min-1.
So what I’m confused about is how you arrived at the energy cost of 10.5 ml.kg-1.min-1 for desk work?
I can’t see where the extra energy cost comes from (nor can I find a relevant entry in the compendium).
Apologies for being unclear previously, and thanks in advance for your patience!
Hi Karla, Those numbers came from the Workwell report, not from me. I asked Staci Stevens (@Workwell Foundation), and she referred me to Todd Davenport (who wrote the report). But she confirmed that, yes, those numbers come from the Compendium.
I recall Staci telling me that you have to be a little careful when looking at activities in the Compendium because a seated task may cost a certain amount of oxygen, but it is more relevant to look at all of the activities required to do a seated job, like getting up, taking a shower, driving to work, walking to the printer, etc.. Even the most sedentary job costs so much more than simply sitting. That is the best I can come up with for you. So, if you are trying to estimate energy costs in METs or VO2 I would encourage you to think about in the way that Staci Stevens explained.
I know, not a very satisfying response, but I will keep digging to see if there is a way to recreate those numbers using the Compendium. I am also trying to track down the source that looks at the costs of activities in terms of Watts. 🙂
Thanks Caroline, that makes sense!