


“We’re saying that ME/CFS is a program priority now…..Give us a chance to prove we’re serious – because we are.” Francis Collins
“We recognize and empathize with the suffering experienced by people with ME/CFS and their frustration that so little is known and so little research has been done to find answers. We aim to change that. The NIH is committed to unraveling the underlying biologic cause(s) of ME/CFS as swiftly as possible.” Collins and Koroshetz
The NIH is looking to the future in this conference, but what future? The title of the conference is “Accelerating Research”. The NIH has certainly accelerated research in ME/CFS – our funding is about double what it was 5 years ago – but acceleration by itself does not mean a field is strong or able to fulfill a disease’s needs.
In 2015 Francis Collins said, “we are going to ramp this up” and that the NIH was now serious about ME/CFS. He also acknowledged the NIH’s historical neglect of the field.
“Given the seriousness of the condition, I don’t think we have focused enough of our attention on this.” Collins
It’s important to note just how bad things were prior to the NIH’s re-invigoration of ME/CFS research in 2015, in order to put the NIH’s next actions in context. We were at such a low ebb – an almost historically low ebb in 2015 – that any increase was going to seem significant.
 Health Rising’s Quickie Summer Donation Drive is On!
Health Rising’s Quickie Summer Donation Drive is On!If my figures are correct, the five million dollars in funding ME/CFS received in 2014 was, adjusted for inflation, the lowest amount of funding it had received from the NIH in over twenty years. ME/CFS was receiving more funding in 1991 – just a couple of years after the NIH started funding it – than it was in 2014. We were in a seriously deep hole – even by our horrifically low standards. (We hit an even lower level in 2007 and 2008).
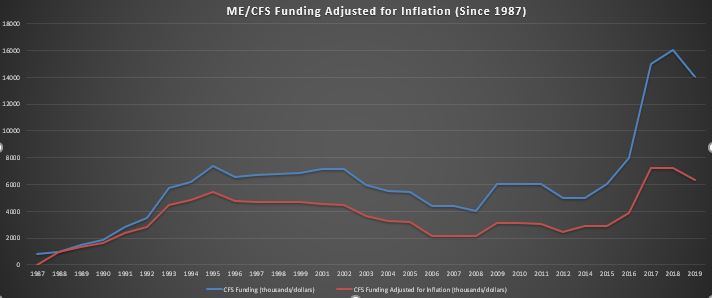
After adjusting for inflation, the recent boost in funding still leaves ME/CFS funding well within historical norms; i.e. still neglected.
Thankfully, funding did triple in 2016 ($16 million). That was the most funding – adjusted for inflation – that this disease has ever received, but not by much. It was only about $2 million more in 1993 dollars than our prior peak ($8 million) on that date.
Since 2016, ME/CFS funding has declined by almost 15%. The NIH estimates that it will spend $14 million on ME/CFS this year, which adjusted for inflation, is just a bit above what the NIH was spending on this disease in 1994.
So yes, Collins and the NIH have accelerated research funding, but only to a level of neglect that the ME/CFS field is very familiar with.
Returning a field to a former level of abject neglect does not denote serious action. It looks like more of the same. Even with Collins’s re-invigoration of ME/CFS research, the NIH really hasn’t budged an inch in 20 years.
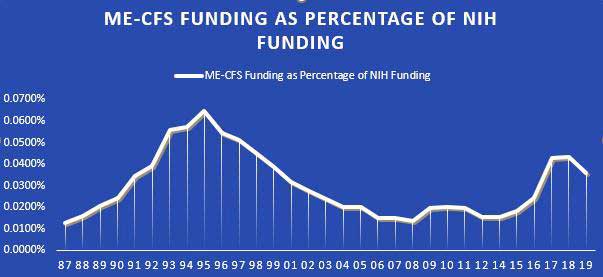
The NIH allocated a significantly higher portion of its budget to ME/CFS in the mid-nineties than now.
In one important way the situation is actually worse than it’s ever been. The number of individual research applications for ME/CFS grants appears to have declined to record lows. (Part of that could be because researchers in the research centers aren’t applying for grants.) That means we’re failing dramatically at getting the most important and biggest source of NIH funding.
Another telling figure is the proportion of the NIH’s budget that it allocates to ME/CFS every year. Even though the NIH is allocating more money to ME/CFS this year than in years past, it is actually allocating a smaller percentage of its budget to ME/CFS than it was from around 1992-1998. Again, this suggests that while funding has increased, it has not increased beyond the historical norms of a disease which Collins agrees has been neglected. ME/CFS was being neglected then and it is being neglected now.
Acceleration Gone
The lies embedded in the “accelerating research” phrase are two-fold. They include the unspoken suggestion that the NIH is doing something unusually meaningful and that it’s currently accelerating research. It’s true that NIH did accelerate research in 2016, but this is 2019, research funding has fallen, and grant applications are probably at historical lows. The NIH has done nothing about either of these. The acceleration, then, is gone and the NIH is now basically standing pat.
Tough Institution to Change
“He (Francis Collins) knows what he has to do. It’s just very hard to do it.” Ron Davis. Nov 2015
When Francis Collins committed to reinvigorating ME/CFS research, we probably should have listened more closely to two of the old hands in the field. Ron Davis said he believed Francis Collins was sincere when he intended to reinvigorate the field but that he had a “hard job” ahead of him. Ian Lipkin said, thanks for all the nice words – but show me the money; he knew those promises were all too easy to make and all too difficult to keep.
“Is it good news for us? Potentially yes…. The function is the budget. Ian Lipkin – reacting to the reinvigoration announcement in Nov 2015
The fact that it took Vicky Whittemore so long to wring the same amount of money (again, adjusted for inflation) that Vivian Pinn in the Office of Research into Women’s Health did in 2006 from the Trans-NIH Working Group suggested that the Working Group may have even hardened itself against ME/CFS over time. When you consider that Whittemore had the public support of the Director of the NIH, the Director of NINDS, the Institute of Medicine report and the Pathways to Prevention report to support her ask, it’s remarkable how stingy the Working Group was.
That told us something about the environment Whittemore is working in. Koroshetz’s claim that Collins’s public stand in support of ME/CFS was courageous evoked ridicule in some quarters, but the fact that he made it indicated something.
Working Group Woes
The Working Group (WG) bashing aside, it should be acknowledged that the WG probably never had a chance. It didn’t make sense twenty years ago and it doesn’t make sense now that the Institutes represented in the group would pony up serious funds for a disease they’re not responsible for. It tells you something that the Working Group – the group responsible for moving ME/CFS forward at the NIH – allowed the 2015 Program Announcement to lapse (PA’s are no longer being done now), didn’t appear to participate in the Fatigue Initiative Whittemore/Koroshetz worked on, and isn’t participating in a panel tasked with providing a way to move this field forward.
A Stuck NIH
The NIH has been treating this disease as an afterthought for over 30 years, is still not serious about it, and could easily continue this way for another twenty or thirty or years.
My guess is that won’t happen: I believe that one or more of our superb researchers is going to come up with a breakthrough that finally captures the NIH’s interest. I think the Nath Intramural study will open doors. Plus, medical technology, thankfully, is moving on at a blistering pace. Even if our current crop of researchers doesn’t have more money than those in the past, they have far more powerful tools to play with. We’re more likely to have a fundamental discovery now than at any time in the past.
Still, the environment of disinterest and neglect that continues to pervade the NIH means that any discovery will take exponentially more time to make a difference.

The NIH has consistently underfunded a group of illnesses that affect millions.
It should be noted that we’re not alone. The culture of neglect that plagues ME/CFS is experienced by every disease it is allied with. Diseases like ME/CFS, migraine, fibromyalgia, POTS, and IBS – which affect large numbers of people, cause pain and fatigue, are largely invisible (don’t produce highly visible signs), don’t produce the mortality rates associated with diseases like heart disease and multiple sclerosis, and affect more women than men – are all being vastly underfunded at the NIH.
Giving Up Not an Option
It appears that we have a few individuals (Whittemore, Koroshetz, Collins) pulling for us in an infrastructure that is pulling the other way. Despite the continuing disappointment that the NIH is, taking the easy route out – giving up or retreating into upset and resignation – is not an option if we want to break the back of this disease in a time frame that’s acceptable to any of us.
Plainly put, there’s no substitute for the NIH. The possibilities that it – with its immense funding capabilities – provides are simply too large for us to turn away from it.
Our goal must be to make the tasks of our allies in the NIH easier by giving them the ammunition they need to wrench the NIH out of its rut. That means getting Congress to push the NIH. The good news is that we have more effective advocacy than at any time in the past.
We have gathered more allies on the Hill than we ever have before. The Solve ME/CFS Initiative and ME Action are more active than ever before. (Check out ME Action’s Facebook feed if you have any doubt how incredibly active the ME/CFS community is.) Democrats, now in control of the House, are believed to be more open to pushing the NIH on health matters. Plus, the NIH’s budget has grown significantly over the past five years. The money is there – we just have to get at it.
In the meantime, we should give ourselves a pat on the back. We’ve done something that no other disease of our ilk or indeed few diseases have done – we’ve more than doubled our funding in a short period of time. ME/CFS now receives substantially more money per patient per year than migraine and fibromyalgia. That’s a tribute to our effective advocacy.
Helping the NIH Help Itself
While the inaction at the NIH is a source of immense frustration and anger, please consider that the kind of people who choose to work at the National Institutes of Health are probably, by and large, people who are, or at least were, committed to doing good works. It’s possible, of course, that the bureaucracy at the NIH has leached that desire out of them. They work in a system, after all, which allows diseases that affect millions of people to be neglected.
Whatever justifications the Institutes or individuals there use for not funding ME/CFS and similar diseases, the fact remains – and they know this – that millions of ill people are being neglected. That fact must drag on those who still remember why they entered the NIH in the first place. I submit that deep down, no matter how well they seem to have covered it up, the fact that so many are not being cared for, must, at some level, bother everyone.
The NIH was not created to be an Institute that awards winners and losers. It was created to safeguard the health of this country. Somewhere along the way, it went astray.
When we push for the NIH to support ME/CFS and similar diseases, we help it to be more like the Institute it was intended to be. I submit that when we succeed, the NIH succeeds, and the people that work there will breathe a sign of relief knowing that they’re not leaving a huge number of people out in the cold. By helping ourselves, we’re helping them and making the NIH a stronger, more effective, more compassionate institution – the kind of institution its founders surely intended it to be.
Bringing About the End of ME/CFS as Quickly as Possible

Bring the end of ME/CFS closer by participating in Lobby Day.
Vicky Whittemore and Walter Koroshetz have created a new group (which includes Jen Brea) that’s tasked with producing a report, due this fall, on how to move ME/CFS forward at the NIH.
That report, as the IOM report was, will likely provide another critical decision point for us. It’s a time we’ll want to bring everything we can to bear on the NIH to make its recommendations a reality. That means politicians slamming the NIH with requests that it honor the report’s recommendations. That starts now – with our enrolling politicians who can provide critical help in the fall.
Join the SMCI, ME Action and hundreds of advocates making a difference on Lobby Day. Find out more here.


Scientific clinical knowledge advances by means of a series of studies that test a series of hypotheses. What are the specific study titles so far organized, by the NIH, to study ME/CFS, if any?
If you go to ProjectReporter –
– you can find the NIH funded projects for ME/CFS.
This is not in fact how science works. The first steps is to observe. Then form testable hypotheses, then test them.
As Ron Davis points out at every opportunity, we don’t have enough data to form hypotheses yet.
Cort. Thanks for the article and I applaud your optimism! As a Veterinarian I always wondered why daily I was literally bombarded by people saying to me “I wish my doctor cared as much about me as you care about my animal.” Now that I’m sick I understand. I think this lack of empathy is pervasive in the Medical Field including the NIH so I am skeptical you are reading too much into lip service- I hope I’m wrong!
I think a lack of empathy is pervasive! I don’t know that its an asset at the NIH actually, and may have been drilled out of some people who work there. I think it’s present in our supporters such as Vicky Whittemore, Walter Koroshetz and Frances Collins. It’s either missing in others or if it’s not then the people with it push it down and probably just throw up their hands and say what can I do? Luckily we’ve found some people who have not thrown up their hands! We need to support them and find more courageous people who are willing to take a stand – say we can’t ignore these people any more – and move forward.
I do think that we are all human beings who deep down do care for one another. That means, at some level, the people at the NIH must be bothered that so many sick people have been neglected. However deeply covered up that feeling is, it is there – I am sure of it.
NIH keeps giving us empty promises because they know it’s a physical illness and want to be able to say in the future: “See? We were serious about this illness. We SAID so.”
But we will never get the needed increase in funding while majority of doctors, researchers and the public thinks ME/CFS sufferers are lazy crazy liars.
Look at the comments online. They are horribly insulting to the sufferers.
So why would NIH increase the funding only to get criticized?
NIH funding has always been about the popularity of the illness, not about prevalence or seriousness. They have no reason to increase it and all the reasons not to.
We need to educate people about the seriousness of ME/CFS. We NEED to change the perception.
Only when NIH sees the public sentiment shifting will the funding become decent.
Great points.
NIH is, unfortunately, almost all about the popularity of the illness – for researchers. They don’t seem to have any mechanism that takes into account neglect or need. They simply respond to what researchers want to study. That’s great if you have HIV but horrible for the millions of people with FM, ME/CFS, migraine and others.
I agree that the NIH needs our support for it to change – and that means Congressional pressure. The IOM Report and advocacy did get us nearly a tripling of research funding. That’s pretty darn good! The problem is that we were at such a low level. Now we need to do it again. I hope that our increasingly effective advocacy movement powered by the SMCI and ME Action and actively supported by organizations like the OMF and Mass ME will get us another big boost.
The bad news from Dr. Bateman is that she’s found that the doctors are the very last to get it about ME/CFS.
The good news is that she finds that researchers are usually pretty receptive once they are properly introduced to the illness.
Those who aren’t – the majority of them I’m sure – are another story but I think there’s hope.
The big question for me is why we’re having so much trouble getting researchers to apply for grants…..
Cort, first let me say this is my favorite post of yours ever by far. Thank you! Agree with everything, especially that the key is to get Congress to pressure NIH and CDC to do the right thing.
As to why there are so few research grant applications submitted- I think that’s no mystery. Decades of severe underfunding, combined with high profile researchers like Lipkin, Levy and Davis getting rejected, in addition to all the misinformation put out by CDC, NIH and others about ME, leading researchers to have a distainful attitude toward the disease and those who research it. Under those circumstances, who would want to apply to study ME?
Thanks Justin. Note that the last RFA in 2006 and the Research Centers RFA in 2015 show that all the NIH has to do to get more researchers applying for grants is to lay some money on the table….Very simple!
I’m holding out hope that this NINDS working group is going to be a turning point for us. If not them I don’t know who.
What Justin said plus:
If you are a young graduated medical professional and do a Phd now on ME/FM, what are your career opportunities in 6 years?
How does it compare to your career opportunities when you do a Phd on hart surgery?
There is money in treating people when your Phd adds to your resume. Surgery pays well. With ME you’re not even sure you’ll be able to prescribe drugs within 6 years or that any of the patients insurance will cover your fees :-(.
You can talk about the few big names in our field. But they are overbooked as they are already. In order to apply for funding they need both good chances at getting that funding and finding and being able to keep the young talent for doing the actual research.
Yes, and then there’s Jarred Younger who’s focusing on ME/CFS and fibromyalgia and has his own lab at a major University and has been successful in getting NIH grants.
He’s showing that it can be done.
Thanks for the data, Cort. It is really sad that only about $3 out of every $10,000 of the NIH budget is for ME/CFS.
I think you might be giving Francis Collins too much credit. Talk is cheap. He has headed the NIH since mid-2009. Eyeballing your own chart, the share of the NIH budget that has gone to ME/CFS research during his tenure has been lower on average than during the prior 20 years.
In my mind, when it comes to ME/CFS and its human cost in suffering, Collins is like an NRA-funded politician who offers “thoughts and prayers” after a mass shooting.
It’s possible but the people who know him say that he really is compassionate and he does care. Plus he apparently has a tough job! I’m holding our hope for Francis! Let’s speak to that compassionate nature which he appears to have (he’s apparently a devout Christian) and at the same time make it impossible for the NIH to ignore us with our advocacy work. 🙂
“and at the same time make it impossible for the NIH to ignore us with our advocacy work.”
When I was at my worst:
* I felt more exhaustion then I ever imagined could exist when healthy.
* I felt more pain then I ever imagined could exist when healthy.
* I felt a sort of “dread”, a horrible undefinable feeling, I didn’t even knew existed when healthy.
* I felt like life all but left me, like being in the constant process of dying yet not just yet.
* I had numerous problems like brain fog, trouble speaking, walking very short distances, chewing, short lasting partial paralysis… in various amounts and mixes
And all of the above was combined in the worst days of which the longest period lasted 10 days before relief.
Now that I slowly get better, I can barely imagine it myself. I can put it under words that fail to describe it in full depth. But remembering it to the full extend? No. My brain can’t hold such intense memories, just like an old cheap analog photo camera can’t hold a clear picture of a person and the full sun next to it. It just has not the needed qualities to capture such intense moments.
Therefore, I cannot expect that people can truly understand the deep agony this disease is. I didn’t look healthy, but how I looked paled into comparison as to how I felt. Add to it that this disease seems to conflict with so much doctors take for granted and you know it takes quite a leap of faith to even accept the little evidence their is to how severe this disease is.
We do not need more advocating. We need a way to point them to clear medical evidence and pathways that changes the question “are they really that sick or sick at all” to “how on earth can they even be alive when such elementary things go that badly wrong?”
The latter may be the true question we need to raise. I feel in part they disbelieve the illness is real and that severe because it would require things to go badly wrong that are supposed to be fatal, not something ones body can survive for decades. Think about patients with the lowest blood volumes. Most should be dead by noon. Think about the disease resembling sepsis the most. Patients should drop like flies if it resembled sepsis enough. Nobody can even survive a quarter of a normal sepsis for years…
Yet future may learn that we do live by and survive many things supposed impossible to survive for a meaningful time. We need to make this disease possible, that is possible in the minds of doctors.
Great analysis
“Therefore, I cannot expect that people can truly understand the deep agony this disease is. I didn’t look healthy, but how I looked paled into comparison as to how I felt. Add to it that this disease seems to conflict with so much doctors take for granted and you know it takes quite a leap of faith to even accept the little evidence their is to how severe this disease is.”
Plus there’s the fact that some people with ME/CFS get soooo sick – far less functional than people with cancer or other major diseases. We’re a big puzzle and I imagine that many in the medical profession – not particularly interested in big puzzles = just throw up their hands and move on. It’s a special kind of person to approach a mystery….
I will be filing a large Lawsuit under Uniform Commercial Cod Laws a monetary Lien including CDC & G7 Countries combined I am now working with a top Team involved with filing these kinds of Liens under UCC
Laws it will be in the hundred of Millions I will seize their assets also a copy will be sent to all Credit Bureau Agencies worldwide including numerous Bank Head Offices I will also seize their Liability
Bonds as well…After 90 days once Final Notices are served I will turn this Lawsuit Lien into monetary Bonds & use the Funds for serious Research. Also, the Mayor of each City filing will also be liable &
sued as well…Enough is Enough I will teach them all what Commerce is all about they will not be allowed to be Bonded for any liabilities unless the Lien is satisfied & Paid in full…
hey Adian,
what do you mean? speek normally dutsh so do not understand allyou write, live in belgium where it is even worse.
I walked out of Dr Cheney’s office after he told me the CDC had buckled under to our evidence, and was going to create “a new syndrome”
wondering how things were going to be.
Would the medical profession “step up” and act with honor and integrity?
Or would this be another sad and sorry repetition of their miserable failures of the past.
Guess we sure got the answer to that one!
Not enough of us die – we’re only disabled – if we can prove it. I became ill in 1994 and will turn 80 later this year. I will never live to see anything change from what it was in the 90s. I wish you all well and hope for that elusive breakthru. I still think Dr. Bell’s book about CFS was the best ever written for patients and their family/friends who believed and cared. And whatever is said, CFS and ME are the same thing. The question is whether someone “really” has CFS.
Exactly – for some reason the NIH doesn’t seem to think it should invest its money in people who, in the prime of their productive lives, get ill and become disabled but do not die. I would bet that the economic losses due to someone becoming ill with ME/CFS and staying ill for decades far exceed the losses of someone who gets cancer when they’re 65.
I got sick with I was about 20. I was lucky relative to others _ I was never as bad off – but I received financial support for decades from my family, never had a good salary, never accumulated money for retirement….and I was one of the lucky ones. Multiple that by a million and then quadruple it because I was one of the lucky ones. Isn’t that worth consideration from the NIH?
The problem is that they don’t take economic losses or need into account. All they seem to really care about is who is pumping in the most grants….
I do not believe the NIH is interested in ME/cfs.They could have easyly sponsored all the questions for centers off excellence. And could give them each more money to work with. The only one who stood up at a video I saw was Ian Lipkin who repeatedly said and asked for more money and that so litlle off money was not workable.
And there are researchers enough but if you ask for a grant, all the work you must do for it and time you put in it, and are turned down again and again, you think a 1000 times before you ask for a grant again.
And the ceters for excellence, they take only the sudden inflamatory onset group I thought. And, I am severelly bedbound, if I could do all the tests they have to do in 1 weak, I would call myself cured!
And how more centers off excellence could the nih be sponsering!?
And what was it, the stopping of the advisory board off specialists and patients, the CIFSAC? They even never listened to them!
How long did it took before graded excercice was removed?
And still, it is “better” then here in Belgium where you are psychosomatich, psychiatry is an open door, GET AND CBT rules,and so on.
And wahat does the nih for the severelly ill ones. we can rot in hell just like I am doing here in belgium.
To many promises! no serious money!
and yes, medicine and technology is going fast forwards. but it is in other deseases. How could it be in ME/cfs if there is no money to research it there or do trials for me/cfs.
When I read all the frustrated commentary I can’t help but think about the ‘ACT UP’ movement which was instigated by AIDS/HIV patients who were also frustrated by research neglect. People thought, “Oh, it’s just affecting a small group of the population–the homosexuals (which often came with unspoken disapproval).
Eventually they got noticed!
Then I think about so many of us confined to our beds or homes… too tired to ‘act up’ in order to get noticed…
I suppose in addition to our own donations, we all need to find at least some small ways to ‘act up.’
It is more difficult for us. The HIV movement had plenty of healthy people who knew they were facing death and got out there and acted up. We have trouble getting family and friends to support us.
We do have a full-time advocate though at the SMCI and both the SMCI and ME Action are really rocking and rolling.
After 31 years of illness And getting worse and worse, I have no husband anymore and in fact no friends. To long to ill. And if possible, the few contacts I still have (also) family, they have never done anything for me/cfs. even not the support of donating 1 dollar. I am just forgotten.Neglected.
We need a true research breakthrough. Until we get something that really fully explains fhis illness, I think people will be skeptical.l, and funding will be suboptimal.
I am sure I speak for all people with CFS that I am beyond frustrated at the lack of an answer….sure there’s lots of interesting research but it really does feel a bit like it’s going around in circles.
We need a much more definitive answer. If not a virus (like HIV), then at least a clear biochemical explanation.
Just think what the USA could do with CFS and other diseases if it trimmed its military and space agency budget by even 10%…. space is interesting, but we have millions of suffering people here on earth!!!!!
A totally forlorn wish, of course!
yes, it would be incredible! even here in belgium. but ofcourse the money would not go to me/cfs but to other deseases 🙁
Thank you Cort, for this timely blog. Michigan ME’ers have a meeting with our congressman at the end of the month. This will help him understand the funding landscape of ME/CFS. Your reporting is always excellent, but I believe this is your best investigating reporting yet. Sure hope Collins and NIH live up to their words and significantly fund ME. You are appreciated!
🙂 Pandora is doing some great work 🙂
Hi Cort. This is a great article, as always. We need something similar for Europe. The European Commission has provided at least 33.9 million euros for research into Lyme disease in the last 10 years (last figures I have are a couple of years out of date). ME got zero funding.
Basically the European Commission (research funding allocation body) has issued specific calls for grants for Lyme disease – x million for the development of a diagnostic test. However, the European Commission has not issued any specific calls for grants for ME.
The Commission is very good at covering up; “anyone can apply” for funding i.e. ME researchers can apply. However, the reality is some things are favoured i.e. by issuing specific research calls for these areas (Lyme) and others are not (ME). I’m currently trying to do some lobbying for funding for ME research in Europe; I’d be grateful if people with knowledge of how the funding system in Europe works would contact me.
Cort,
I am happy that you stayed with this work of eyeballing NIH funding for ME/CFS. The story shows in your charts. It has to be told over and over again until NIH personnel are ready to listen. I have hope, too, but it may not come in time for me and many others from the early years.
Hi Cort and fellow CFS victims. The timing of your posting of this article was some kind of karma for me. For no particular reason other than wanting a sense of history, I have just finished re-reading Osler’s Web. Wow, how some things never seem to change. A good portion of what we know today was known in 1996, when the book was originally published. I read it in 1996, but appreciated far more the politics, the sabatage, and the OVERWHELMING denial of the exisistence of CFS as it emerged. We were scorned by the CDC and NIH officials and most doctors. Research was not funded, most treatment for patients was based on psychological problems, patients told “it’s all in your head,” just pull yourself together, exercise more,” etc. How a few dedicated doctors and scientists fought bravely on for victims against massive and systemic resistance.
I have had this disease for 40+ years. My wonderful primary car dr. Of 30 years retired last year, and i had an interesting journey trying to fill her shoes. Here we are in 2019, and in the last 6 months, i was told, “just take a cold shower in the morning, that will get you going,”get a nice new hair do dear, and you will feel better, and “you’ve got to exercise more!!!” I could not get any of these MDs to write me a prescription for LDN, look at my lab results re high viral load and low killer cells. Multiple times I tried to share printed out research on PEM, which was just handed back to me, on and on, and on.
The point being, we are not so far from 1996, and what treatments do help are denied because the docs know nothing about CFS. Can’t tell you how many times I heard, “there are lots of reasons for fatigue.
I hope Cort is right, and the NIH is truly going to fund research for CFS. Personally, I doubt research will help me in my lifetime. I think what would help patients are mandatory CEUS for all licensed medical practioners. I have forwarded i fo on the Conference to many.
i hope 1 or 2 won’t delete it. May e mandary CFS trauning is something patient groups could advocate for. There have been lots of breakthroughs, but access to new treatments is hard to access. Most doctors still don’t recognise CFS as a disease. ?
Keep up the good work, Cort. You are a lifeline of validation and hope for all oatients!
Thanks for the analysis Cort.
To be frank I think it is unfathomable why not one of the CFS/ME national charities saw fit to systematically collect data like this and publish it each year so that the CFS/ME community could at least understand what was really going on.
What is the point of advocay if you are not willing to honestly measure the impact of your efforts? Instead we got a bunch of self serving happy talk about how much progress we were making.
I hope someone will make an effort to continue collecting this data and produce yearly updates to this analysis so we can have a realistic sense of what is actually happening.
I think it’s a good idea. Jennie Spotila at OccupyME – http://occupyme.net/ is a great place to get analyses of NIH funding. She’s a personal blogger like me.
I suggested to IACFS/ME that they do analyses and provide grades every year to the NIH and CDC of how well they are filling the gaps. How great would be a scorecard every year! They didn’t take me up on it though.
That said I think SMCI and ME Action are doing great work :).
That’s great Cort! Very nice prospect.
You have been one of the best advocates we have for so many years. Thanks for everything you do!
Francis Collins makes us beg. And we don’t even get much for our begging.
Why doesn’t Francis Collins use his discretionary funds to help us? If he leads the way, role modeling that this disease should be taken seriously, the various institutes will follow.
Thank you for this blog post, Cort. NIH needs to be held accountable for their dismissal of 1-2.5 million disabled Americans, a quarter of whom have spent years (even decades) barely able to care for themselves,
Decades! That’s how long you and I and others have been asking and prodding and hoping that the NIH will do something significant. Again and again and again we get the nice words, the false concern and nothing really gets done. It’s past time for the NIH to wake up To the cost of its neglect, the decades of lost lives, the enormous productivity costs. I wonder if they realize what a cruel organization the ME/CFS community believes them to be. Do they really want to be perceived this way?
The dems are altruistic do-gooders. Have the desire but no followup or accountability skills. I live in Seattle. The liberal hornets nest. Good at throwing money at projects or planning to. What we really need is a high profile spokesperson. The NIH needs to be de-funded and eliminated because of the good ol’ boys club it appears to be. Look at how quickly they got HIV research off the ground. They know how it is spread. Are they still researhing. I do not wish any illness on anyone, but seriously – when there is a treatment or they know how it is transmitted how about focusing on a disease that nothing is known about. But we have NOTHING. No spokesperson. This is so neglected and I always feel they are researching other diseases to death. And do not forget big pharm. If there was a glimmer of hope they would be all over something they could make money on. The govt does not need to be involved in everything. Too much into special interest groups and lobbyists. Don’t we have any lobbyists??? I am furious. I am 71 and I had plans for my life and relocation to the Pac NW. I have put up with this for many many years. I have a nice car – BMW Z3 – that I really enjoy driving, the rare days I am able. My eyes have almost been ruined. I have a neurological permanent handicapped plate because of dizziness. I wanted to hike and volunteer. I have grandchildren. I have no social life. And I am angry and I get very depressed. But good ol’ Kaiser is on a mission to keep legitimate patients from meds that help them, yet feeding meth to young children because of poor parenting skills and enabling drug abusers. The innocent people who follow the straight and narrow are the people suffering in this country and I am sick to death of it. And that is where the NIH stands. They simply do not care about giving a leg up to those who need it. Just keep hammering away at the same old high profile diseases.