


The ATP Profiles test developed by Dr John McLaren-Howard (and the Mitochondrial Energy Score developed from it) has been a big deal for the chronic fatigue syndrome (ME/CFS) community. The test formed the basis for studies dating back to 2009 by Dr. Myhill, Dr. McLaren and Dr. Booth which asserted that mitochondrial dysfunction plays a major role in chronic fatigue syndrome (ME/CFS).

The ATP Profiles test results seemed to make perfect sense: the mitochondria in people with ME/CFS simply weren’t producing enough energy (ATP). The Tomas paper, however, suggests the test results were wrong.
Mitochondrial dysfunction subsequently became a central theme in Dr. Myhill’s writings, website and treatment protocols. (See – The Central Cause: Mitochondrial Failure) in ME/CFS and her book (Diagnosis and Treatment of Chronic Fatigue Syndrome and Myalgic Encephalitis, 2nd ed.: It’s Mitochondria, Not Hypochondria). Dr. Myhill’s website states that the ATP profiles test she’s used extensively (@ 1000 results) provides an objective test which clearly differentiates ME/CFS from healthy people.
“The joy of the ATP profiles test is that we now have an objective test of chronic fatigue syndrome which clearly shows this illness has a physical basis.”
The studies were like a breath of fresh air which provided hope that a cause which made perfect sense (reduced mitochondrial activity!) and an objective test for ME/CFS had been found. With the emergence of more studies suggesting that problems with energy production were a big deal in ME/CFS, the earlier studies seemed prescient indeed.
Plus, they presented a potentially ground-breaking possibility. If the tests could be validated, the U.K.’s National Health Service could conceivably include them in their list of accepted tests for ME/CFS. Cara Tomas PhD, Dr. Newton MD, PhD and their group reported that it was with that possibility in mind that they attempted to validate the McClaren mitochondrial test.

The Tomas Study
Cara Tomas1, Tiffany A. Lodge2, Michelle Potter2, Joanna L. Elson3,4, Julia L. Newton1,5 Karl J. Morten2. www.nature.com/scientificreports/
Having taken into account a 24 hour delay between blood collection and cell isolation, we have shown decreases in ATP parameters in control cells similar to those seen by the Myhill group in the CFS/ME patients. We suggest that it is potentially the delay between sample collection and cell isolation that is causing the decrease in mitochondrial function previously reported in CFS/ME patients. Tomas et. al. 2019
The test, which employed various factors to assess ATP levels in neutrophils and PBMC’s, failed at all levels. However the samples were tested, ATP concentrations, ATP ratios and ATP to ADP efficiency were the same between healthy controls and ME/CFS patients.
So how did a test which formerly found all 138 ME/CFS patients to have at least some mitochondrial dysfunction apparently get blown up so completely? Tomas believes it came down to a very simple and vexing issue that we’ve come across multiple times before: sample preparation.
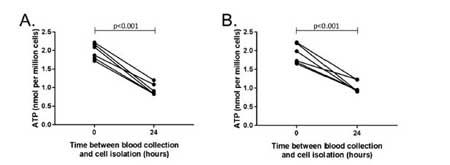
Drops in ATP concentration after samples sat in test tubes for 24 hours
Tomas reported that the 24-72 hours that elapsed between when the blood was taken and the test was done changed things – and suggested that the Myhill group should have expected that it would.
For one, they expected that the neutrophils – the immune cells being assessed in the papers – would become activated and then die. Apparently, once activated, neutrophils survive just a day or two, and they can be activated very easily. Tomas wasn’t worried about a little activation – they were concerned “most of the granulocytes would be lost” in the 24 hour or so delay between sample acquisition and processing. (Neutrophils are a granulocyte.)
Plus, once neutrophils (like all immune cells) get activated, they burn up a lot of energy – thus potentially depleting ATP. (The MyHill studies used neutrophils but in the Acumen lab McClaren switched from using neutrophils to PBMC’s a couple of years ago. No results from that lab have been published.)
Testing fresh blood vs blood that sat for 24 hours made all the difference. Both ME/CFS patient and healthy control blood which sat for a lengthy period of time had lower ATP concentrations. ME/CFS and healthy control blood which was quickly tested, on the other hand, had normal ATP concentrations.
Tomas did more than test the test, however. They tested whether their concerns – that neutrophils would drop out over time – were valid. Using flow cytometry to measure the cell types present in fresh blood and in blood which sat over time, they found evidence that neutrophils – the immune cells being tested for ATP concentrations – were indeed dropping out over time.
Another basic issue – glucose depletion – came to the fore as well. Apparently, unless cells in a test tube are “fed”, their glucose levels are expected to fall over time. Tomas found that glucose levels in the test tubes which sat did indeed drop significantly – and quickly. It took a mere 2 hours for glucose levels – the main fuel for the mitochondria – to become significantly depleted.
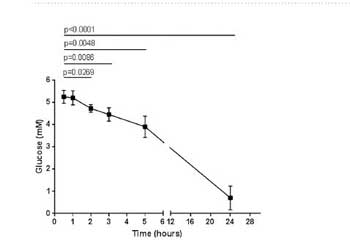
Glucose declines over the 24 hours samples sat in test tubes.
However, these issues didn’t explain why, if MyHill studies were done on both healthy controls (HC) and ME/CFS patients, the HC and ME/CFS samples would be processed differently. It turned out that the ME/CFS samples were sent “through the post and processed between 24–72 hours” later while the healthy control blood samples were collected in the laboratory and processed the same day. The Tomas group believes that this difference in sample processing made all the difference.
Tomas et. al. concluded that the ATP profiles test as now run is inaccurate and should not be used or trusted. They asserted that the test should only be run within an hour of sample collection – something that may not be possible, given how the test is conducted now.
The real blow to the test, though, came when Tomas was able to find no differences in ATP concentrations between the ME/CFS patients and the healthy controls, even when the test was run immediately on the samples. It should be noted that the effectiveness of the Myhill protocol does not hinge on the results of the McClaren test. Even if the test does not show mitochondria problems, the mitochondria could still be dysfunctional.
The study was small (10 patients and 13 healthy controls), but the authors believe it was large enough for them to call for doctors and patients to disregard the results of this test.
Dr. MyHil and John McClaren Respond
Dr. Myhill posted several responses to the paper on her website – none of which, unfortunately, addressed the issues raised in the Tomas paper. She reported that the testing was blinded, that the tests are less expensive than they might have been, that approximately 1000 tests have been run and that the tests are routinely run in quadruplicate, etc.
One statement, “The essence of this paper appears to be that tests of mitochondrial function are not relevant in the assessment of patients with CFS/ME,” is clearly incorrect as the Tomas group has found evidence of mitochondrial issues in ME/CFS and would surely welcome a commercial test that would show that. In fact, in the paper Tomas suggested that, “Other tests of
energetic dysfunction (in ME/CFS) could be developed using the Seahorse extracellular flux assay,” (but advised caution until it was clear what role cellular energy production problems play in ME/CFS).
Dr. Myhill stated that she did offer to take blood from one patient and send samples to both laboratories to be tested the next day. She reported that the Tomas group’s failure to take her up on her offer left her group with, “little confidence in the ability of the Tomas group to replicate the Acumen test.” Research groups, however, often have strict protocols which don’t allow for deviations, and it’s unclear what one paired test would have shown.
Dr. McClaren did respond to the central issue. He reported that during the initial testing he explored the effects that sample storage might have using samples that were processed within minutes and re-tested 6, 12, 24, 48 and 72 hours later. He stated that, provided that the samples were kept in the original “vacutainer” tubes and not subjected to extremes of temperature, there were only minor changes in the test results up to the 48 hour point. After that, some samples began to degrade, and he uses phase-contrast microscopy to separate out samples which have signs of cell damage.
His statement, “Test situations regarding time since venepuncture and storage/delivery methods continue to be explored” suggests, though, that not all the issues regarding sample processing have been explored.
Conclusion

Tomas believes differences in sample processing skewed the ME/CFS patients’ results in the three Myhill studies. John McClaren asserted he tested storage effects but noted that he was continuing to study the matter.
It makes sense that McClaren would assess the effects of storage, as he developed the test, and it’s not clear why the two groups have different findings. Still, with the publication of the Tomas paper, the burden of proof now appears to fall on the Myhill group to find a way to rebut the Tomas finding – probably with a peer-reviewed paper which validates their current testing regimen (using PBMC’s).
That may not be easy. Cara Tomas is a recent PhD who’s been racking up research studies and Julia Newton is a well published researcher. Dr. Myhill, a doctor, and John McClaren, the director of the Acumen lab, are more lay researchers whose output appears limited to their three ME/CFS papers.
Is this the case of well-intentioned efforts gone awry? In retrospect, perhaps the Myhill study results always were a bit too impressive for this heterogeneous disease. Only one of 71 ME/CFS patients in the first study had a normal result and all 138 patients in the second study demonstrated mitochondrial abnormalities which correlated with illness severity to boot.
Efforts to understand the role the mitochondria play in ME/CFS continue, but most recent studies from researchers using the Seahorse machine and other approaches have failed to find evidence of reduced ATP production in ME/CFS when the mitochondria are tested in isolation from the blood. Five studies have found normal ATP production, one has found increased ATP production and one (Tomas) has found reduced ATP production.



The study on mitrochondria with Drs. LIGHTS , in Utah —- was processed immediately. The lab guy sat in the room to take it straight to the lab. Since this was a test with families with ME/CFS, FMS, POTS etc. It was compared to each other and gene mutations and then their function. My sister and I shared at least 50% of mutations on our genes. But despite us sharing some, my function was way, way lower than my sisters. (I was in lowest 20% of all CFS patients in the study.) I also was very tired having traveled 9 hours the day before to get there (and my sister lives there). But was having a bad POTS day too. We were told that if you “push the envelope” and there are mutations with the genes, then likely we both would have shown dysfunction. But I also have all 5 mitrochondrial complex at very, very low function level and my sister did not.
Personally, I feel this is one piece to my puzzle. But not the whole picture.
I think it’s important to emphasize that the mitochondria are very complex and there are quite a few ways to measure them; i.e. if the McClaren test is ineffective it does not in any way mean the mitochondria are not effected in this disease. Tomas pointed that out in their paper. (Nor does it mean, I don’t think, that Dr. Myhill’s approach may not work or help.)
Hi, I also participated in the Light’s study but haven’t gotten all of the results (just a few). Did you hear back recently? I’ve been so excited for this.
Hi there, what does all 5 mitochondrial complex mean exactly? Thanks!
I guess this means I can probably stop my oral ATP supplement. I’ve been taking it for about 4 years and never could really tell if it was helping or not. One less thing to buy and a few less pills to take.
You wrote: Dr. Myhill, a doctor, and John McClaren, the director of the Acumen lab, are more lay researchers whose output appears limited to their three ME/CFS papers.
However, the paper itself was written up by Professor/Doctor Norman Booth, a physicist. While the two researchers are definitely ‘home-grown’, Norman had the correct academic background and I assume he must have looked into all of the results very closely. He would have asked all sorts of questions in order to write it. I am sorry Norman is not still alive to ask questions of the Oxford group, as I know he worked closely with Dr Morten on a few things, and Dr Morten was given much of Norman’s research results on his death.
It is definitely a puzzle.
I know Dr Myhill is disappointed that the Oxford group did not take them up on their offers to provide more help.
Would time lapse make this much of a difference? I don’t know. Are we trying to compare apples with oranges? Only time will tell.
Certainly I value your statement that even if the test is found not to be valid, that does not mean that Dr Myhill’s protocol is invalid. It has worked for many people.
Actually according to PubMed Booth published just five papers over his career – three of them on ME/CFS and two others – if it is same NE Booth – in 2003 and 1990.
Research groups try to limit the variables involved. Adding another sample from another doctor would have possibly introduced another patient type plus there’s the issue the sample processing all over again.
I don’t see any reason to worry about Dr. Newton’s access to ME/CFS patients as she’s an experienced researcher who has done many ME/CFS studies. The Tomas group drew the samples from healthy controls and patients and then immediately began testing them in two different labs over the next 24 hours or so. That was probably the simplest and most effective to do this study.
To be honest I can’t think of any reason to doubt their results.
Cort, we have done many experiments using cells from mice, and had found using the fire fly assay (the same method Tomas used) that ATP degrades at the rate described in Tomas’ humun cell samples. However, a colleague of mine recently tested degradation rates in mice cells using HPLC and found no degradation over 24 hours. Another colleague here measured the loss of ATP function in neurons known to respond to ATP and found no decreases over 2 days. The later may be explained by the use of very high ATP levels, but we cannot figure out why the HPLC showed no degradation. It could be there is a problem with the fire fly assay, or that something in our culture medium is the cause. At any rate, we are still trying to figure it out. Sometimes what you thought you knew and should be well known isn’t.
Also, we have just finished all patient and control collection and sequencing in our NIH ME/CFS project and will soon start the long hard analysis of our large samples of ME, FMS, vs. well, frequent migraine, and depression patients. As Issie indicated, our large samples included families.
Thanks so much for the info Alan. I wish this was all clearer! It does seem there is some gray area and McClaren reported he’d assessed the effects of sample storage – as one would suspect he would. Once again, and I’m sure not for the last time, we have a bit of a conundrum.
Good luck with the analysis. Always so glad to hear of large sample sets with other diseases in them!
Here is the response of Dr Myhill and Dr Mclaren-Howard.
https://www.drmyhill.co.uk/wiki/Response_to_the_paper_%27Assessing_cellular_energy_dysfunction_in_CFS/ME_using_a_commercially_available_laboratory_test%27_by_Cara_Tomas_et_al?fbclid=IwAR2DlP8Lr5jyfeqYv3LCWIOJycczLssImSt2F4rdWWtkJNz0Fg6WyGP4lDU
Would love for you to cover the US based MitoSwab test, which is 85% correlated with muscle biopsy.
I have used it, in concert with HDRI NO and nitrotyrosine tests and a Genova Diagnostics NutrEval, to track my progress. The MitoSwab showed abnitmally low mito content, impaired Complex I, and overactivity of other complexes throwing off huge amounts of free radicals, matching the huge oxidative stress and high nitrotyrosine on the other tests.
Working these issues, by repairing damaged mitochondrial membranes and feeding mitos the nutrients they need has helped reduce the oxidative and nitrosative stress, which multiple researchers have found in ME/CFD, and increased my energy and activity levels.
The MitoSwab is a useful test.
Hi Learner.
That is interesting about the MitoSwab test and your finding of impaired complex 1 activity and increased activity on all other complexes. This correlates with Lawson’s finding that, paradoxically, our mitochondria are working harder and the cristae are more condensed. This also ties in with evidence of an over-activated sympathetic nervous system and increased flux across all energy producing systems and the one carbon / methylation system (particularly for the Cortene and Klimas models which assume a brain driver). Yet, sympathetic activation is hardly unique and our HPA axis findings are mixed. I can’t help but wonder what sets us apart from other medical conditions that are also marked by increased sympathetic tone when our physical function is so extremely affected?
I note that the co-factor for electron chain 1 is NAD (along with coQ10), which is an output from the kyneurinine pathway that Stanford are looking at. If NAD is low then GSSG to GSH conversion will also be impacted, GSSG concentrations will increase and GSSG will leach in urine leaving an imbalance between increased oxidative stress and GSH. I think this is significant problem for me personally.
Is NAD one of the substances you have targeted and managed to increase? If so, how? I see reservatrol is meant to increase NAD enzyme activity. I have had enormous success with mito nutrients and extra B2 (riboflavin) and B12.
On a more general note, I don’t think that the McLaren Myhill Booth work is wasted or their legacy tarnished. This team were one of the first to highlight the potential role that mitochondria play in this illness and many of the metabolomic and other studies that have followed in their footsteps have found issues with energy production. Is great to have scientific rigor.
To me the key content here is: “have failed to find evidence of reduced ATP production in ME/CFS when the mitochondria are tested in isolation from the blood.”
The ‘Swap Test’ done by Ron Davis’ group showed that the nanoneedle cell stress signature followed the ME/CFS patient plasma. ME cells in healthy plasma = no stress signal. Healthy cells in ME plasma = stress signal.
IMHO, Dr. Davis’s finding makes any testing of cells “in isolation from the blood” potentially inaccurate.
Well done for putting their response here Diane. The mitochondrial test saved my life and I will be eternally grateful to all concerned for the test and subsequent treatment.
Cort, you knew or should have known that they had responded to this research. Please publish balanced articles here in future. It could be disastrous for people to stop their mitochondrial support.
Just so you know I contacted the Myhill Clinic to see if they had a response and they provided a link to it. I think you missed the last part of the blog where I put the relevant parts of Myhill’s and McClaren’s response. It starts under the heading “Dr. MyHil and John McClaren Respond” :). and linked to it.
(I didn’t put the entire response on the blog because most of it didn’t address the Issues Tomas uncovered in their study. )
My apologies Cort, I read the first part and got rather annoyed! As you can appreciate the fact Dr Myhill’s mitochondrial treatment got me out of severe heart failure and being bed pbound for many years, it doesn’t take a lot to annoy me when it comes to any criticism of the test.
I hope that the journal who published this study allow Dr Myhill’s reply, as so far they have not published her response, which has been offered three times.
I think one problem with Dr. Myhill’s reply may be that she did not directly respond to the issue of sample storage times. IMcClaren did – he reported that he’d assessed the effects of sample storage on testing.
I was thinking the same thing in regards to Davis’ findings. Another good reason for the Myhill group to address these published concerns.
And as an analytical chemist myself, a complicated test that cannot be replicated in a different (and reputable) lab absolutely needs to be questioned. A critical part of any rigorous test method validation is having a different person run the same samples (if possible) on a different instrument, without the direct involment of the 1st analyst. They must get equivalent results. A method that has not gone through VIGOROUS validation is nothing to hang your hat on, ever.
How can person get Swap test done?
I live in the UK and was probably one of the first to have Dr Myhill’s test done in 2007 and some of the follow up ones too. I also had another ATP done with her a few years later.
They both showed low ATP and it was rapidly used up and I also had a partial blockage in my energy production but they gave different reasons. The first was stated as being due to viral blockage and the second one was said to be due to nickel blocking ATP production which I thought was odd.
I also know of some other patients here in the UK who have had a few ATP tests run through Acumen and managed to get a greatly improved score but they stated this did not correspond in any way to an improvement in their health. They remained very sick so once I heard this I didn’t feel it could be a useful test after all.
So all I’ve those ATP supplements do nothing?
I think you just have to judge for yourself whether they are working or not.
Because the McClaren test is just one of many tests used to assess mitochondrial functioning, its accuracy or inaccuracy doesn’t necessarily, I don’t think, mean the mitochondria are functioning well or not. I imagine that another test that tested another aspect of mitochondrial functioning could still be abnormal.
This issue about the test doesn’t necessarily, I don’t think, tell us anything about the success of Dr. MyHill’s protocol.
Learner1, I got curious about your test, MitoSwab, so looked it up; https://www.mitoswab.com/index.php
Nowhere did I see a price and on the order form it looks like one would need a doctor’s assistance/approval to apply. Probably a bit pricey and most likely not covered by Medicare! But maybe… Care to share?
My thoughts on this echo Birdie’s when I recalled Ron Davis positing that ‘it’ might be something in the plasma and not the mitochondria themselves. Truly, the complexity of the situation would give pause to folks trying to hold on to ‘pet’ theories’ to prove they are correct. Results that don’t agree should spur further excitement and questions (as well as frustrations).
Cort, I’m all into sharing what treatments have helped people. Is there a column that I have missed where there is input from everyone about the treatments they have tried and if they have helped or hurt–a sort of grand list of submissions (all in one place)? I would really like that!
And thanks again!
Thanks Nancy we hope to have something like that soon 🙂
Is this the same Dr. Myhill who has had several malpractice cases put against her. If so I’ve found her to be a person who blends her commonsense with speculation, and then narrowly believes it as fact. That’s not a good thing in science. So I’m not surprised with this finding.
I also think her advice on diet is dangerous as she again has put too much faith in a hypothesis. Also stating high fat intake is safe. Yet the meta analysis on this was studies cheery picked by scientists paid by the dairy and meat industries. There’s plenty of other meta analysis studies done that show high fat intake isn’t good for long term health. Although the fat argument is slightly different for ME/CFS patients due to ATP production issues (or is it now?)
Another speculation is in saying only to eat seasonal fruits and vegetables. Yet humans evolved on and around the equator where fruit grows all year around.
I believe she means well and I know some ME/CFS patients have improved, but some improve anyway. I followed the Myhill protocol with no improvement.
I think people should be a little wary of of her claims.
“Blends her commonsense with speculation, and then narrowly believes it as fact…she again has put too much faith in a hypothesis” – this is EXACTLY my thoughts on her approach, which she very often oddly calls the “correct way”.
Her whole evolutationary keto thing is just completely made up from thin air, and there are so many pieces of evidence completely contradicting it that she simply never bothers to address.
Actually, what I see as the big problem with the Myhill test is that it can only be done by McLaren-Howard. He is retired and does this test out of passion. What happens when he can no longer test? I see it, as it stands, as having a limited life, unfortunately.
It’s amazing how much energy, time and money has been wasted in this disease on the immune system, mitichondria etc. I am sure Myhill was well meaning.
Jay Goldstein was looking to the brain/CNS 25 years ago and that’s where efforts should have gone. That’s where the answer lies.
Please no more wasted energy on the immune system, ampligen etc etc.
Exactly my thoughts too. Brain brain brain & inflammation …
https://www.youtube.com/watch?v=nIwI-NQ3em8
41:00 Minute mark, in relation to ATP. ATP should not be outside of the cell (Blood).
The entire video is great, if you are familiar with Dr. Klinghardt.
Thanks for the link to this fantastic video — an amazing introduction to autoimmune conditons produced by the “Cell danger response”, the role of retrovirals & how to fight them, by an evident expert. Have seen Dr Klinghardt previously in a Sophia Education Health Talks Online Summit, hope to find more from him.
The link between CFS and Xenotropic Murine Leukemia Virus (XMRV) as a “distinct inflammatory signature” using Luminex multi-analytic profiling, will be one subject to explore further.
Plus the role generally of endogenous human retroviruses (HERV) in Lupus, Rheumatoid Arthritis, Multiple Sclerosis, and Epstein-Barr infections: noting that memory B cells are the “reservoir” of EBV infection — having read somewhere else about the effectiveness of Rituximab. But even better, Klinghardt cites OSR (which is what? — now called Erminex) and a wealth of better, natural remedies for treatment. Other terms in connection with OSR were Emeramide, and “IRB Certified”. So a great deal to look up.
On OSR, one of his slides referred to ……. Boyd Haley Ph.D., a 2010 IAOMT YouTube video: in connection with the effects of wifi exposure in causing Calcium release into brain cells, with the resulting relese of Peroxynitrite.
And on diagnosing retroviral activity, Klinghardt recommends CD26 and Nagalase lab tests and RANTES for inflammatory markers, each available in the USA for c. $60.
The range of treatments he cites is extensive: BioPure (Germany) for anti-Purinergic therapy; N-acetyl Cysteine (NAC) and Glutathione; R-Lipoic acid; high dose (300mg/day) transdermal melatonin (N-acetyl-5-methoxytryptamine) available from Vitahealth New York pharmacy, and DHEA (Dihydroxyepiandrosterone);
The general idea of “Cell Danger Response” as a reaction to a host of environmental pollutants (including heavy metals and wifi) and pathogens, and of “Anti-Purinergic Therapy” as effective treatment fits well the observation that, far from mitochondrial deficiency in ATP production in CFS / FMS / MCS etc, mitochondria are working overtime to meet the high energy demands of pathogens stimulated by a range of pollutants and nutritional deficiencies.
Fortunately Klinghardt provides a wide range of natural remedies and their functions in combating these disease-promoting conditons. Polyphenols from Teas including particularly Cistus tea (Cistus incanas (Ci)) whole leaf extract (BioPureUS.com); Stevia Rebaudina whole leaf extract (to get rid of eg Borrellia Burgdorferi); Mushroom (Ganoderma lucidum); Nettle (Cymbidium hybrid, Epipactis helleborine, Urticadioica); Olive; Bitter Melon; Seeds of the bitter gourd.
And other powerful antioxidants: eg Broccoli sprouts when 2″ long. CBD oil (Cannabidiol) or THC (Tetrahydrocannabinol) if necessary — while they rmeain on sale, before the pharmaceutical industry produ es synthetic versions and the natural ones disappear.
Vitamin B5 to “silence the virus”; Pantethine; Palmitoylethanolamide (PEA) to control neuro-inflammation, and Luteinol (Lut) combined as co-ultra PEALut “Glia Lia” from Italy; Brown algae — marine micro algae from the coast of Korea (www.BioPureUS.com).
Skullcap root (Scutalaria); Hypericin and pseudohypericin (something-wort — rest of the word offscreen). Plus “old malaria remedies”: Quinacrine (in small doses), and Suramin.
These are the scrappiest of notes: there is no substitute for watching this video with a huge wealth of information.
Hi Gabriel,
You really hit the nail on the head with your synopsis of the video. I still believe there are a lot of nay-sayars when it comes to EMF. (I dont know why…)
Its a shame, Irminix (Emeramide) is not for sale on shelves. It is a natural compound. The FDA changed the rules as soon as they learned this product was chelating mercury out of the body, and helping Autistic children, unbelievable:
From Dr. Mercola’s Website:
Haley’s first product, developed in 2006 and sold between 2008 and 2010 under the name Oxidative Stress Relief (OSR), was shut down by the FDA in 2010 after a complaint was filed. Haley explains the circumstances:
“When they shut me down, [my attorney, an FDA expert] told me, ‘Dr. Haley, this is silly. The compound has in-structure, dicarboxyl benzoate, which is found in cranberries and cystamine, which is on the terminal end of coenzyme A. It’s just cysteine without the carboxylic acid group. It’s a natural product.
Two natural products [combined], just like slow-release niacin and n-acetyl cysteine … It can be [sold as] a natural product and a supplement if it contains any one of a natural product or any combination of two’ …
That’s what [the FDA rules] said. And then they changed that. We call it the Boyd Haley rule now. [The FDA] said, ‘Not if you put [two natural products] together chemically’ …”
I have no words for that, I just shake my head….Nine years later, the compound is Still not available for the public. Unbelievable. The great thing about this compound is that it binds all toxic metals safely out of the body!
It seems like it would be really easy to solve the mystery as to whether or not delayed processing of the samples affect the result! Are you kidding me!
I also posted some information on the:
Is the Brain Causing the Small Fiber Neuropathy in Fibromyalgia (and ME/CFS?)
article if anyone is interested,
Dan
Brilliant article. Thank you Cort. Its undeniable that Dr Myhill is a strong minded, controversial figure here in the UK, and moving further away from the mainstream. I would hold reservations about any clinician who evades or rejects critique or findings that disagree with their established position. She’s built her reputation and private business on that test. Negative or conflicting findings are things to be welcomed and drive further knowledge and exploration. Closed mindedness, ego and conflict of interest are all so very dangerous in the behaviour they generate. It is exactly the same mentality challenge we battle against in the entrenched persistance of the psychosocial model in the current abysmal UK nhs clinical practice, and we need to guard against it within our patient community too and remember our own medical diversity and the illnesses’ complexity means our individual experience does not mean anything hing is an automatic given to be automatically defended or attacked. I always worry when ego led confirmation bias behaviours pop up in the ME research world, with its scant research resources. And there is no question watching her videos that Dr Myhill has it in spades, perhaps the same strong mindedness that led her to enter the field and work so hard for patients for so long is working against her now. In contrast it was great to hear Dr Younger explicitly talk about being open to findings that disprove his neuro inflammation hypothesis and also that further explore root causes in his recent video. More broadly I worry about the issues you mention regarding the heterogeneous nature of M. E. Particularly when lumped together with the broader CFS umbrella. With so much research being done on tiny sample sizes (let alone preparation) surely it doesnt seem to have to have taken much to have sent us down rabbit holes or to have potentially misssed or seemingly passed by something potentially of massive significance. But somehow we need to join up all these dots and figure out which are red herrings. Bigger more accessible sample cohorts, robustly diagnosed with tight criteria and well segmented feels vital to moving forward now we have demonstrated biomedical abnormalities. It feels at times like we are still fighting just to get into the starting blocks. Hopefully things like the Canada initiative the US centres and UK Biobank are finally starting to give us that solid foundation to launch from. Thank you for your incisive blog. It continues to bring hope to hear the dedicated work going on
I was waiting to see if someone posted about SFN, which I had confirmed after my skin biopsies were sent to Corinthian Labs in TX about 2010. It was the first tangible evidence I had of my disease (along with elevated EBV titers during flares). Thanks for posting this.
There is a difference between cellular energy and “energy”/fatigue. In ME/CFS people experience severe fatigue but I do not think that ATP deficit is the cause of the fatigue/energy drop. As you are aware my “hypothesis” is that both ME and FM (and MCS) are all sensitivity illnesses. (first mooted by Mohammad Yunus)..
Nociceptors are well understood and we now know that the pain thresholds in FM are affected by an IGg mediated auto-immune interaction on the nociceptor.
We know that the distribution of chemo-receptors are extensive in the respiratory and digestive tracts and we know that many of these receptors are of the same ion-channel group as the TRPM3 nociceptors, which are the suspected ion channels affected in FM. So I think we might get closer to understanding MCS as an auto-immune illness as well. Way back in 2000 Dr. Chaudhuri wrote about ion-channelopathy in ME in Medical Hypotheses:
https://www.sciencedirect.com/science/article/abs/pii/S0306987798908222
(Sorry I cannot give the full paper but I have it myself)
The difficult one is M.E. because we do not fully understand how fatigue is generated in illness. We know that it is; because in many common illnesses/infections energy levels crash at certain points during the illness. The list of illnesses generating fatigue is long.
https://www.mayoclinic.org/symptoms/fatigue/basics/causes/sym-20050894
Of course in these illnesses the fatigue is most often resolved but in some, like MS it returns cyclically.
I do not think this fatigue/energy deficit in these ME, FM or MCS is due to mitochondrial dysfunction. I am not saying that mitochodrial function is not affected in ME, FM or MCS but that it is not producing the severe fatigue. We have to look elsewhere than the “obvious” mitochodrial ATP synthesis.
Some people’s energy levels are severely affected by the flu, other people not so much. We know is most auto-immune diseases energy levels can be affected at various point in the cycle of symptoms.
Energy drop/fatigue may be an adaptive response to disease – a necessary response to keep the animal from over exerting and putting themselves at risk while in a “compromised” state. So I assume that we have a system that controls this. Just like we have a system of pain generation. It is a system we do not fully understand. The ion-channel hypothesis is current as we have seen from the research by Staines, Cabanas and Marshall in Australia.
https://www.abc.net.au/triplej/programs/hack/breakthrough-in-diagnosis-of-chronic-fatigue-syndrome/10188210
https://www.ncbi.nlm.nih.gov/pubmed/31014226
We can see this in the natural killer cells but lets look further!
Thats great information Dr. Hodgson,
I will also further state that Chornic Fatigue Syndrome may not be an exclusively autoimmune disease, but rather a detoxification issue as it relates to to poor liver metabolism and the inability to neutralize toxic substances. This is where herbal therapy can be of the upmost assistance.
I do agree – in part. In FM we see chronic peripheral pain causing significant brain changes including neuro-inflammation in many regions of the brain and microglial activation possibly also mediated by dysfunctional DRG modulation. i.e. brain changes which are distant (physiologically) from the nociceptor function. Hard to imagine at first but it seems to be what is happening.
There is a parallel in ME/CFS.
In the chronic fatigue state we see extensive metabolomic and biotransformational changes. (detoxification as you say) Some of which relate to genetic SNPs which are idiopathic. Now I am proposing that in the fatigue state we see a similar relationship between the pain and brain changes and the fatigue and the biotransformational abnormalities. In this case via the gut function. Ion-channelopathy in the gut will “reek havoc” on biotransformation – this why we see so much “damage” in ME/CFS.
I will add further that hidden infections such as Ischemic Osteonecrosis in the Jawbone (Prior wisdom tooth removal) and Root Canals are major factors in chronic fatigue and MCS, and need to be addressed and/or ruled out for the immune system to not be chronically suppressed and the nervous system to not be in constant fight or flight. These kinds of infections are hidden, and only perpetuate illness, and wreak chronic havoc on the body. Couple that with an improper diet, you are literally on a fools errand for most of a lifetime, with more and more symptoms and less relief.
https://iaomt.org/
A good starting point is learning about Blood Type and the proper foods that help the body achieve optimal results. Blood type is a major factor when it comes to dietary lectins in foods and stress responses. One man or woman’s food can be anothers poison. In addition, Secretor-Status of the Blood type antigen is integral in relation to disease and symptom Susceptibility.
http://www.dadamo.com
Best,
Dan
Sorry Dan, too complicated and probably downstream.
I disagree, respectfully of course!
Theres really nothing too complicated about Osteonecrosis in the jawbone, as it is quite common in relation to wisdom tooth extraction. As far as root canals are concerned, the tubules connected to the root of the tooth are infected. This is why many holistic dentists will refuse to perform a root canal, and simply just pull the tooth.
In relation to Blood Type and the individual, it is of extreme integral value as a health paradigm. Secretor Status is a SNP, whether or not the individual produces both the bound and unbound form of their blood type antigen, where the unbound form is produced in digestive juices and mucus membranes which the majority of people do, (however many dont) matters in relation to overall health and disease susceptibility. This is just one of many factors, but a big one. The stress response in blood types differs as well. The immune system differs, everything is different. The blood matters and it is not pseudoscience by any stretch of the imagination!
Riddle me this, why can every other bone infection been shown on a normal x-ray, CT scan yet jaw bone Osteonecrosis “cavitations” cant?
How does an infection that cant be treated by antibiotics because “theres no blood supply” stimulate the immune system? well if we are going to go with the idea that these cavitations have no open oxygen supply then they have to be anaerobic bacteria, and then for the most part be considered gram negative bacteria as they make up most anaerobic bacteria then what would be stimulating this immune response would be endotoxins like Lipopolysaccharides, but wait theres no blood supply for antibiotics so these endotoxins would have a hard time getting out of the bone into the blood stream stimulating this immune response causing such a drastic state of fatigue. i remember when the so called experts on this conditions realised this issue in their hypothesis they then blamed small molecule gases that “leaked out of the bone’ such as hydrogen sulfide acting as a “neurotoxin” yet you’d only have to smell a dogs fart and get more hydrogen sulfide. Not to mention the mouth is fully of bacteria and can never been seen as steril, even these so called cleaning out cavitations would only allow more bacteria entering the bone “hole” whilst doing this. Infection causes illness in relation to the immune systems level of activation or when hidden from immune response by the level of how systemic they are and how many organs they are affecting. which sooner or later becomes very evident when organs start crashing. I’m open to any idea and never fully rule out another means in which an idea might cause illness via different route . I think more common sense has to be applied to all these hypothesises being constantly made.
Thank God for your honest reporting Cort!
It took a long and painful journey for me to realize that popular energy protocols (supplements, low-carb diets etc.) don’t work for me and may be overrated in general. I have classic post-infectious ME/CFS, yet every single one of such protocols has made my condition worse. I persevered longer than I should have, largely because the functionalists who prescribed them, informed by their mitochondrial theories, were adamant that they would help. They were so confident, in fact, that they led me to question my own symptom experience and treatment compliance.
Perhaps I wasn’t a bad patient. Perhaps it’s just bad science.
A diagnosis of ME/CFS is one thing, but to be able to rule out causative factors is integral. It varies individual to individual, there is no one size fits all approach to this.
I agree, general supplements probably arent going to “fix” this. A low-carb diet, I mean…..that doesnt fix anything.
“Class Post-Infectious” would mean that your immune system is currently compromised in some degree.
Are there any factors that are contributing to your symptoms that you are aware of? Physically, anatomically, psychologically? I mean, thats the thing about this kind of condition, its a survival technique in the body more than anything, and thats how symptoms result.
Please when you have the time, look into Jaw dysfunction, hidden infections from wisdom teeth extraction, root canals, amalgam fillings. Think about any heavy metal exposures in your lifetime, including amalgams. Do look into your blood type and see what foods contribute to hormonal imbalances and agglutination of your red blood cells that interfere with energy metabolism and create intestinal permeability.
Im not trying to lecture you at all, just explaining that the paradigm of this chronic fatigue is larger than most physicians realize.
Dont give up!
Best,
Dan
Hi Dan, I know this is an old thread I’m jumping into but I’m really interested in what you’ve written about the jaw. I have been suffering with moderate ME/CFS for a year now after several years of mild symptoms. I had both upper wisdom teeth removed under local anaesthetic about 10 years ago. They seemed to heal quickly at the time and it wouldn’t have occurred to me there could be any problem there until reading your post. When you say it’s a hidden infection does that mean there might not be pain at the actual site? Or any other signs of an infection there? I do get sinus pain and pain from my temples extending down the side of my face, but hadn’t associated this with my jaw or teeth before, but perhaps it is. I’d be very grateful if you could point me in the direction of reliable information on this. I’m in the UK, so don’t know if it’s something that it looked into here or not.
Many thanks,
Andrea
Hi jpw,
You bring up some good questions, Ill do my best to answer them. First, a jawbone cavitation is nothing new, along with proof of necrotic bone. Since the cavitation is small and hollow in a jawbone, the best way to locate one at the present time is with ultrasound technology, where the best version of this machine is being used in Europe, with the older one or whats left of them in the United States. Its very easy to locate a cavitation in the jawbone. You have to understand with a cavitation, the location of it is what will determine what types of symptoms an individual may or may not present with. Left side of the body will involve all the organs and meridians of those meridians. Its is a significant energy blocker, it interferes with the bodys healing system and nervous system. The root canals much more affect the immune system, but a caviation in the jawbone will have an impact but not necessarily have a direct effect in the blood.
These arent hypothesis by any stretch of the imagination, maybe you need to speak to those who have had them cleaned out! A jawbone incision, and appropriate cleaning methods were used so that the body can naturally heal itsself like it was originally supposed to post surgery. The oral surgeons generally use anesthetics that inhibit the blood clotting properly, in addition the periodontal membrane is usually just left their as well. The cavitation will then form. This is not a hypothesis, this is a fact. Its not that difficult to recognize. Its common sense that after a tooth is removed, of course the blood has to clot for healing to begin. If that doesnt happen, a cavitation results. And when that results, maybe I used the term “hidden infection” inappropriately, it is much more of an interference field, where all kinds of bacteria and viruses that were already present in the body are able to stay and cause interference in the body to a substantial degree. One has to couple this with all the other interfering mechanisms in the body, a good example would be electromagnetic frequencies. Again, these electromagnetic frequencies will have more of an impact on an individual depending on the amount of metals inside the cells of ones body, as they act as an antennae. The jawbone is notorious for storing heavy metal such as mercury.
Sure a hypothesis can be made based on the clinical evidence but it is not confirmed until the surgeon makes the incision into the jawbone and can actually see what has taken place, and can actually see where bone has not developed. This is not pseudoscience, you seem very taken a back by the fact that people develop a cavitation when they are in fact common. What determines the detriment it has on the body, mental or physical, is going to vary from individual to individual.
Im not sure what you do or dont believe, speak with a holistic dentist or any patient, they can tell you how ridding the body of disease is beneficial. A cavitation is a disease that formed because the bodys healing mechanism didnt have the opportunity to perform, because the blood not being able to clot in that area. Maybe you have some concern of how one locates one, but believe me, when one has significant psychical and mental symptoms and for years doesnt know why, they are thrilled to locate a causative factor and are willing to have performed a low risk procedure where the wisdom teeth more likely than not didnt have to be removed in the first place. The only reason why this is a common procedure is because under-developed jaws dont have enough room for the wisdom teeth to erupt sustainably. If the jaw wasnt under-developed, this was not be an issue. But it is. It has nothing to do with the teeth itself, the wisdom teeth are not the problem.
You stated:
“Infection causes illness in relation to the immune systems level of activation or when hidden from immune response by the level of how systemic they are and how many organs they are affecting. which sooner or later becomes very evident when organs start crashing.”
Thats correct. And a hole in the jawbone that acts as a strong energetic deterrent can accomplish this over time. Not everyone’s jaw is in an ideal position either, along with the symmetry of the joints. Everything plays a factor, and root canals are just as dangerous.
Best,
Dan
Think about your sleep as well, many people are undiagnosed with sleep apnea, you do not have to snore to be diagnosed with Sleep Apnea. The cause of sleep apnea? A narrow airway way due to an under-developed jaw. What is a prominent, perhaps the number one symptom of sleep apnea? Chronic Fatigue. The body and the brain simply are not getting enough oxygen to fulfill its requirements, resulting in stress that you may not even have realized was taking place.
Is a sleep apena machine going to fix the airway? Absolutely not, which is why an oral appliance called the DNA appliance was created. It is worth looking into.
Okay, I assure you I will not bring up the Jaw any more, unless anyone has further questions. I think I have made my point, and hope that Im not offending anyone here as a new contributor.
Best,
Dan
Here is a simple outline of my channelopathy hypothesis.
The main consideration in non metabolic fatigue is the relationship between nerve signalling and calcium release. Muscle fatigue is the decline in ability of a muscle to generate force. There are two main causes of muscle fatigue: the limitations of a nerve’s ability to generate a sustained signal (call it neural fatigue); and the reduced ability of the muscle fiber to contract.
nerve signal weakening, can be a limiting factor. The nerve signal can be weakened by ion-channel dysfunction.
Though not universally used, ‘metabolic fatigue’ is a common term for the reduction in contractile force due to the direct or indirect effects of two main factors:
1. Shortage of fuel (substrates) within the muscle fiber. Hence the idea that ATP production is deprecated.
2. Accumulation of substances (metabolites) within the muscle fiber, which interfere either with the release of calcium (Ca2+) or with the ability of calcium to stimulate muscle contraction. ROS production and/or poor blood perfusion.
Over-simplifying: In some ways FM is an afferent problem ie. lowered nociceptor thresholds produce higher than “normal signals” which are unmodulated by the DRG. The brain receives these signals as significant or high pain. The resulting brain changes help to produce the many other symptoms (brain fog etc.) (Of course the ion-channels on the nociceptors are in other tissue besides nociceptors).
ME/CFS is an efferent problem: weakened neural signals into the muscle fibers (the brain may be generating appropriate signal strength) fail to generate sufficient muscle contraction/power and more neural energy is required to “force the contraction and results in sensations of extreme fatigue. The more exertion that is applied the more the neural energy fails to elicit sustained work and extreme fatigue results. The fatigue is both muscular and mental.
Both of these pathologies are the result of calcium channelopathy. One being mostly afferent and the other being mostly efferent. Of course a person can have both pathologies and I would say everyone with FM and ME have both to varying degrees.
I am over simplifying this as calcium ion channels influence other TRPs such as sodium and potassium channels. In particular TRPM3. This the ion-channel identified by Staines, Marshall and Cabanas et al.
People with FM often suffer from intractable myoclonus, muscle cramp and spasms. It may be that the intracellular chloride which partially inhibits the contraction of muscles and prevents muscles from contracting due to “false alarms”, (small stimuli which may cause them to contract) is affected by the calcium ion channelopathy because these chloride channels are mostly calcium activated chloride channels.
The two main Voltage-Gated Calcium Channel discrepancies I’m aware of inside of the brain are Glutamate Excitoxicity and Electromagnetic frequencies, both are scientifically proven. (The pulsation of the frequency) Again, depending on an enormous multitude of factors, (SNPs of GAD1, DAO for example), heavy metals inside the cells, particularly Mercury and Aluminum, this is more discussed with diseases such as Alzheimer’s and Parkinson’s, but if your talking about Calcium Channel issues, these two actions act upon the cell to provide increased calcium, eventually forming to apoptosis. Of course this is going to affect ATP inside the cell also.
The bottom line is, there is no one size fits all cure, the cells are a product of their environment.Only treating the individual and ruling out causative factors can there be success. Trying to find a link between an issue with ATP an thinking its groundbreaking research atleast to me, for me personally, is not the way to solve a burdened body. The human condition is at stake mainly becasue of unwanted exposures to the body, with EMF playing a huge role in fatigue for sure. For years this was looked at as pseudoscience, but thats a falsehood. If you dont believe me, look at the research of Martin Pall, PhD. People like to say Wi-Fi and Cell Phone pose no threat, but thats ridiculous if you look at the science. Its the pulsation of the frequencies, the power is irrelevant when talking about these kinds of frequencies. Just because its “non-ionizing” doesnt mean were off the hook, especially if the burden of heavy metals inside the body which act as an antennae are present. Not to mention, knee and hip replacements, where biofilms are also able to invade those sites. Couple that with exposure to non-ionizing radiation, yeah your going to feel it at some point.
Im just saying, who cares about ATP in the blood, that doesnt lead patients to a successful outcome. Making a silly distinction and trying to show that CFS people are “different” based on a blood test. I encourage everyone to do their own research, and dont be fooled by functional experts, a lot of the times they dont know what they are doing either. Its tough business, but I hope all success, I really do in finding out underlying causes and perpetuating factors in their illnesses.
Best,
Dan
One of the things that Klinghardt refers to in the YouTube video you provide a link to above) is the prevalent heavy metal toxicity of virtually all of us now, from multiple sources. He argues that it is the presence of heavy metal pollutants in our bodies and brains that makes us particularly susceptible to EMF pollution: with pulsed microwave radiation from cellphones, DECT phones, wifi, smart meters etc — at 7.q million times any “safe” level according to Dr Martin Pall, research biochemist — as well as EMFs from “dirty” electricity in domestic etc wiring circuits.
Klinghardt cites environmental sources of aluminium as including geo-engineering using aluminium nano-particles (in an attempt to cool the atmosphere) showing two NASA photos of the Earth as evidence. This might be disputed, but the presence of aluminium (as a highly reactive metal) in cooking pans, deodorants, food cans and many other forms cannot be disputed.
Pall emphasises that it is the pulsed nature of microwave radiation that makes it so dangerous at a cellular level: activating not only voltage gated calcium channels but also sodium, potassium etc channels — ie wreaking general havoc. And while exposure to high amplitude radiation is dangerous in itself, even very low amplitude microwave radiation can be just as dangerous, since the human body operates at microvoltages which can be easily disrupted.
So cleaning up one’s environment — eg substituting wired connections for wifi is better than, at least, switching if off when not in use — is just as important as detoxing the body.
As a lay person, who has suffered with CFS/ME for 3 years, I’m amazed, and slightly appalled, at how many of you are patting yourselves and those that ran this study, on the backs for possibly putting a spanner in the works of Myhill’s regimes, beliefs re: this illness. Great, so her tests may not be all that accurate and it may prove that ATP/mitochondrial supplementation is a bit pointless.
Rather than putting so much time into proving one another wrong (and I understand that that is also important in moving forward in any illness), maybe put the same energy into finding the causes/root of this awful illness and actually help people like myself who are literally at the mercy of a health service that diagnoses us and then pushes us off into the dark cellar and hopes we don’t have the energy to come back out again.
You’re all so sure you know the answer, but I’ve yet to see any of your findings prove to be in any way beneficial to more than a handful and yet people with CFS/ME are still being treated as if this is all one form of the same illness and not subsets of the same illness with different causes/presentations. Which is way the only treatment that is currently available to us on the NHS is the same, barely useful pacing advice.
The one thing Myhill has done, which is something few others I’ve seen or read have done, is listen to patients, hear their stories and views on this, what has and hasn’t helped them and work with them. I saw somebody further up in the comments talking about research into wisdom tooth extraction – how are these sorts of tangents helping anybody?
I’ve tentatively started Myhill’s regime, with little obvious improvement, I’m only a few weeks in and I’m not particularly hopeful So I’m not biased in that way, I’m just appreciative of the fact that she’s attempted/attempting to find answers. Whether she’s eventually proven wrong re: mitochondrial function being the cause of ME, or not. I know others who have seen great improvement, others who have gotten worse. It may be wise to heed the reason why so many patients are keen to give her views so much credence though – she listens to them, and is actually trying to help. Whether she’s ultimately right or wrong, whether she’s making money out of this, it’s clear from the hundreds of CFS/ME sufferers she’s personally seen: she wants to help them and is at least trying.
Similarly, others have seen improvement by changing diet, seeing an osteopath, leaving work, staying in bed all day, increasing exercise/decreasing exercise. I’m sure you’re all aware what a complex disease this is, but suggesting ‘it’s all in the brain/CNS’ or other such all-encompassing responses is nonsense – you’re being as single-minded as Myhill herself. The only way these questions get successfully answered is with a multi-disciplinary approach, with a massive sample size of patients – with the patients involved all the way. I’m just seeing above, so many views of ‘what it definitely isn’t’ with few explanations or ideas (or interest, desire?) to find out what it is.
So rather than celebrating this little victory over somebody who seems to be considered an outsider by the medical community, put the same enthusiastic energy into finding us some bl**dy answers. Please.
Yours,
A supremely frustrated and angry ME sufferer.
Yes, whether the test works or not (and right now it doesn’t appear to) doesn’t have anything to do with the effectiveness of Dr. Myhill’s treatment regimen – and here’s to more research – we all need many more answers.