


Did the NIH spend a year getting ready to study long COVID only to miss its last, best chance at doing so?
It seems like an incredible thing to ask but one must now ask if the National Institutes of Health (NIH) is going to miss, yes miss, its best opportunity to study long COVID. There’s a lot riding on the NIH getting this right. For one the amount of money, the NIH has available to study long COVID simply dwarfs other efforts. Its studies will be immensely bigger, better funded, and better organized than any others. Plus, long COVID is just one of many diseases (chronic fatigue syndrome (ME/CFS), fibromyalgia, postural orthostatic tachycardia syndrome, autoimmune diseases) that stand to benefit from this unique opportunity.
Moving at what Director Francis Collins said was lightning speed (for them), the NIH approved awards to build the massive infrastructure needed for the RECOVER (Researching COVID to Enhance Recovery) initiative by June 2021. The main protocols were created by July, and then in Sept., the NIH announced it had provided over $470 million in grants to more than 100 researchers at 30 institutions
So far, so good. The NIH very quickly (for them) put together what appears to be an impressive effort that emphasized similar protocols, patient registries, data collection sites, and biobanks.
In Sept. 2021, Dr. Stuart Katz, a leader of the RECOVER initiative, reported that the effort would in what he called “an unprecedented scale and pace of enrollment” enroll tens of thousands of participants over the next 12 months. With the initiative containing enrollment sites in all 50 states, though, Katz clearly believed it feasible. In an apparent burst of enthusiasm, one NIH rep even stated the NIH hoped to launch treatment trials in the next year to a year and a half. In Nov 2021, Dr. Katz reported that the first phase of adult enrollment had started in October and the next phase would begin in December.

The group seemed to have things well in hand but, in truth, things were starting to get tight. If the NIH was to capture long COVID in the act, it would need to extensively test people as they came down with COVID-19, and then follow them as they came down with long COVID. Only then would they be able to tell exactly what went wrong.
A recent study underlined how complex the situation is. It found that the seeds of long COVID began early in the initial infection. It was able to trace long COVID six months later back to its roots using the data from the original infection. It couldn’t do the opposite, though. Six months after the infection had occurred, everything had become so jumbled there was no telling how everything got started.
It was imperative, then, that at the very least, the NIH got as many samples as possible from people with COVID-19. It didn’t need to do anything with those samples. It didn’t even need to have created the protocols to test them. It simply needed to have large numbers of samples that it could later test.
While the coronavirus – with its big Delta wave and even bigger Omicron wave – was certainly cooperating, it was not as if the virus was going to hang around forever. The NIH, it seemed, though, had lucked out. The fast-moving, highly contagious Omicron variant gave the slow-moving NIH a lifeline to fill its huge cohort of patients, gather their samples, and start following them.
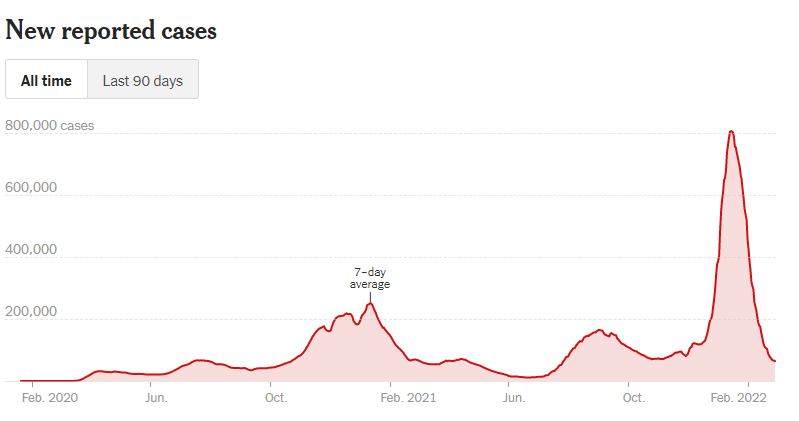
As the Omicron variant quickly fades the RECOVER Long COVID program has only a fraction of the participants it needs. (From the New York Times)
Except the NIH appears to have mostly missed the Omicron wave. With that wave quickly fading away, the NIH last week announced that it had enrolled a grand total of 670 people of its projected 17,680 people long-COVID cohort. Six months after Katz stated he’d hoped the RECOVER initiative would enroll tens of thousands of participants in the first year, it had enrolled less than 700. (We don’t know how many long-COVID patients, healthy controls, or COVID-19 patients are in that group).
Unless the NIH has been banking a lot of samples somewhere – or has access to a lot of samples – which is a possibility – it appears to have missed its best and probably last chance to catch long COVID in the act. It will still be able to intensively study people who have already come down with long COVID but it appears it’s mostly missed or at least blunted its opportunity to get at the early stages of the infection.
There’s no doubt that ramping up a $500 million program of grants for a new disease entity is not a piece of cake, but being able to catch only the tail end of long COVID is surely not what Congress had in mind when it gave the NIH $1.15 billion to study long COVID.
Other less critical things are lagging behind as well. Six months after it awarded almost $500 million in grants, the RECOVER Initiative still has not published what those grants are. After listing the University research sites a couple of months ago, it’s taken them off the website. Six months after Katz talked about enrollment sites across 50 states, none have been listed. The only way to find out about enrolling in a long-COVID study that I can find is to leave your email address and zip code. It’s a big mess



The world hopes that we have seen the end of Covid, and that we can live with it like flu, but it is also possible that we will have another variant with another big wave. The problem then will be that we won’t know if those patients were affected by the Omicron variant. Their covid samples may be affected by previous bouts and won’t give the pure data we would prefer.
Thanks, Cort. Seems like the NIH has got some explaining to do. What is going on, really..?
Fumbling incompetence and inadequacy. Those are a few words that come to mind when thinking of the NIH and their ‘efforts’ on Long Covid and even more so,on ME/CFS.
Wow – “670 people of its projected 17,680 people long-COVID cohort”. I truly hope they are not “slow-walking” their study. If so, it’s so very disappointing.
I wonder what Congress will make of this. Advocacy week will be a good time to find out.
I imagine that Congress expected better
Cort…Thanks for all you do for all of us! A thought….what if we have all missed the point? The saying goes “Follow the money!”. What if the money flows in the opposite direction? What if big pharma is in actuality paying the World Health Organization, NIH, CONGRESS, etc., ALL the other companies claiming to support finding/funding cures for Fibro/ME/CFIDS/Long Term Covid, etc., to NOT find/fund cures? What if, through creative bookkeeping, the funding can be allocated to “other” more desirous (financially more beneficial) studies, cures, medications, etc., that can increase profits in the short term as well as long term for whatever purpose, for whatever program, for whatever is most popular in the political arena at any point in time? WHO can profit the most, for what reason, for how long and what is being done with the funds? After watching the unbelievable occur in the political arena throughout the world in the past several years, especially in these past few months, follow the follies, follow the money, follow the fools, who stands to gain the most ? Thanks for at least considering the questions.
I don’t believe that Pharma is doing all that. When I see the NIH refusing to fund potentially low-cost and effective pain relievers like LDN – which would threaten Pharmas hold – I do wonder what the heck is going on. Since LDN is compounded the NIH is basically the only game in town for funding.
It is a stunning failure.
Nothing will change at NIH until Fauci is gone. Unfortunately his eventual replacement may also be a salesman for vaccines and drugs looking for a disease to treat (remdesivir).
Welcome to the New Dark Ages. As long as the grant money flows, lack of results is irrelevant.
More concerning, their assessment protocol is worse than useless: it includes a 6-minute walk test and as many sit-to-stands as the patient can do in 30 seconds. Not only does it sound like they are trying to cause PEM, they have no assessment of symptoms or objective findings the next day. This is despite the fact that patient advocacy groups specifically warned them against proceeding with these protocols.
Situps? What in the world? They have a lot to learn. I do see that cardiopulmonary exercise tests and tilt table tests are included. A big question , though, would be if they’re going to do 2-day exercise tests as one-day test results can be misleading.
ME/CFS and long Covid are the same virus reactivated Epstein Bar Virus which does not show up in EBV serology. The NIH and the medical establishment have been covering up the cause of these diseases as for years the treatment for all the inflammatory autoimmune diseases has been corticosteroids which interfere with the immune system and the virus gets stronger. They are not about to admit they have been harming patients for years. This is why they confuse people with all sorts of studies and tests which get nowhere and have the desired effect of confusion. The evidence is out there if you look at reactivated Epstein Bar Virus which also reactivates during Covid infection.
In case anyone is interested, here’s a pdf of the slides that Steven Deeks of UCSF used yesterday on the RECOVED webinar. The first few slides address this cohort issue. The video should be posted soon to the RECOVER web site. He was quite candid, refreshingly candid I thought, about many aspects of the project (esp re: establishing the cohorts).
https://drive.google.com/file/d/1e7-PLsVC5MV37Q55ynyxrCKkDfpo6qTz/view?usp=drivesdk
Perfect – thanks Michael and glad to hear that Deeks is being candid. Always a good sign.
Michael would you mind posting Dr Deeks website? I’m not finding it by searching.
Nevermind, found this article: https://magazine.ucsf.edu/long-haul
Clinical site: https://www.liincstudy.org/en/team
Not only is EBV serology inaccurate CMV and HHV6 serology is also not accurate the only way to test is PCR DNA test.
Denis Copeland,
Could you give references for cmv hhv6 as this may be useful for doc?
I saw this news and thought it was very interesting…
‘Bill introduced to aid with long COVID’
‘U.S. Senator Tim Kaine led the introduction of the Comprehensive Access to Resources and Education (CARE) for Long COVID Act, legislation to help people living with long-term COVID-19 symptoms. This bill would improve research on long COVID as well as provide resources for people with long COVID. U.S. Senators Ed Markey (D-MA) and Tammy Duckworth (D-IL) are also helping introduce this legislation.’
https://nrvnews.com/bill-introduced-to-aid-with-long-covid/
I’d like to insert some good news on the research front. Note about midway down there is a crash survival guide. It was recently developed by the BHC and can be utilized in a variety of situations. They have encouraged sharing it and I thought this would be a great place to do that!
Here’s their recent newsletter:
At a time when the world is reeling from conflict, anger and disillusion, we may be hesitant to trust the light on our COVID-19 horizon, but I’d like to share hopeful news. For COVID long haulers: there is an ever-growing scientific and medical response to your situation. For everyone else who has long been invisible and abandoned with ME/CFS (plus other post-viral and related conditions): there is an ever-growing awareness in our society that you exist and matter. With a persistent and unified message we can translate that into scientific and medical progress for all of the forgotten.
It has been my life’s work to raise awareness of ME/CFS. In 2000, I typed out “raise awareness of CFS and FM” in large font on a piece of paper and placed it under the glass of my desktop. Without a doubt, there was consistent slow progress over time, but now it has become exponential growth.
Journalists have been interviewing Dr. Yellman and me regarding Long COVID and its relevance to ME/CFS. Recent news stories have appeared in USA Today, National Geographic, Yahoo News, Google News, Vox, and North Jersey News. Journalists are asking more informed questions and articulating these long overlooked and understudied areas of science and medicine. We must all keep the conversations going in every arena. I admire and thank the patients who have shown the courage to speak out.
I continue as a faculty resource for the CDC-funded ECHO telemedicine project called “Long COVID and Fatiguing Illness Recovery Program.” The agenda strategically combines lectures on ME/CFS with Long COVID and related conditions for medical providers. The 2-year program provides weekly medical education sessions to a group of designated primary care providers in California, and also an open and nationally available ECHO webinar each month. The quality of these educational programs is very high, drawing from clinical experts around the country, and the content will be available as recorded sessions for other health professionals. It is certainly a different experience for me to be engaged in high level medical discussions with experts who now completely embrace and appreciate the significance of ME/CFS and its relationship to what we are seeing in COVID Long Haulers. This is progress that can’t be reversed.
The NIH-funded ME/CFS Collaborative Centers 5-year grant period ends soon. Centers are submitting their research for publication. The NIH has opened the grant application process for the next cycle. Could it be better funded? Yes. But I want to remind everyone there are many ways to push for progress. This includes educating medical providers, engaging the media, and making a constant effort to inform our politicians who fund the NIH. We will continue to use every resource and lesson from Long COVID to benefit all with the underserved chronic illness conditions that fall within the mission of BHC.
Before I close, I must say how proud I am of our BHC team that produced the “ME/CFS Crash Survival Guidebook.” Since the online introduction of the guidebook on February 3rd, there have been more than 18,000 webpage views and thousands reached on Twitter and Facebook. Feedback to BHC, especially from the severely ill, has warmed our hearts. Please share widely with anyone who may benefit.
Thank you for your trust and support.
Lucinda Bateman, MD, Founder and Medical Director
Education & Outreach
ME/CFS Crash Care Kit Essentials
Just as every well-stocked home has a first-aid kit, every home with a person with ME/CFS should have a “Crash Care Kit.” Page 30 of the ME/CFS Crash Survival Guidebook provides recommendations for items to include in your kits. We suggest keeping a few in areas of your home that you frequent, and to have a “go kit” ready for when you leave home. Click here to download the ME/CFS Crash Survival Guidebook.
BHC Collaborates with New Organization: LiveOn.org
LiveOn.org is a non-profit community established to support the millions of chronically ill who suffer from post-infectious diseases, such as ME/CFS, Long COVID, POTS, EDS, MCAS, NCS, Chronic Lyme/MSIDS, among others. Through disease awareness, education, personal stories, and digital connection, they are striving to help the chronically ill, their caregivers, and the healthcare community come together to support, to encourage, and to find solutions that shorten the journey to a better quality of life.
Research
ME/CFS and Long COVID Research Opportunity
BHC is simultaneously conducting a study on endothelial function, upright activity, and cognition in pw ME/CFS and Long COVID. The study will require a 2-hour in-person visit at BHC and then will continue for 7 days with tests and surveys that are done from your home. Learn more about the study requirements here.
In the News
Dr. Bateman Interviewed by National Geographic
How COVID-19 Can Harm Pregnancy and Reproductive Health
Women are experiencing a range of changes in their reproductive health as a result of COVID-19 infection. “One of the reasons may be that the female immune system is deeply interlinked with hormones, particularly estrogen. So, understanding the virus means understanding how the immune system responds to this pathogen.” Read the full article here.
Dr. Yellman Interviewed by Yahoo News
COVID Could Launch an Epidemic of Chronic Fatigue Syndrome, Doctors Warn Journalist Gene Myers covers hot topics in his article about the overlap of Long COVID and ME/CFS. He shares what ME/CFS advocates already knew about post-viral illness before COVID-19 came along, the pulse on research funding, and scarcity of medical providers. Read the full article here.
Dr. Yellman Interviewed by North Jersey News
Fight It? How Not to Handle, Distinctive, Debilitating Crash from Chronic Fatigue Syndrome
In this recent article, Dr. Yellman encourages pw ME/CFS or Long COVID, their support network, and medical providers to understand the dangers of “pushing through” when the patient is experiencing PEM. Read the full article here.
Dr. Yellman Interviewed by USA Today
Trapped in the dark: How chronic fatigue syndrome derailed a NJ musician’s life
James Strazza has severe ME/CFS and his mother is his full-time caregiver. This article sheds light on the plight of individuals experiencing severe ME/CFS and the need for research and medical education. Read the full article here.