


A brief note: life continues to happen! Last week I noted that a solar upgrade was getting in the way. This week a veterinary emergency kept Health Rising off the air more than expected. Everything appears to be resolved but it was a tough couple of days. Find more about it on my Facebook page.
Geoff’s Narration
The GIST
Camille Birch PhD “I was completely blown away by what I saw”.
Six years ago, a startling Solve M.E. presentation from Liz Worthey and Camille Birch suggested that rare genetic variants – which are not uncovered by standard genetic testing – may be impacting energy production in significant numbers of people with ME/CFS.
Then, life happened: the COVID-19 pandemic occurred, there was a maternity leave, a lab move, long COVID popped up, and it took a while for Worthey and Birch to resume their studies. They’re back, though, with their first paper, “Uncovering the genetic architecture of ME/CFS: a precision approach reveals impact of rare monogenic variation“, using an expanded data set.
Liz Worthey has a PhD in Genetics from Imperial College, London and is the Director of the Center for Computational Genomics and Data Science at UAB School of Medicine. She is a pioneer in doing the kind of complex genetic analysis done in this paper. Camille Birch has a PhD in Biomedical Engineering and is a genetic data analyst.

I talked with them in what turned out to be a rather long discussion about their work.
Whole Genome Sequencing Project
First, a look at the whole genome sequencing (WGS) they did. As Liz explained, 6.4 billion nucleotides form the “letters” that make up our DNA. Most genetic studies examine about a million of the nucleotides that most often contain variants. Because of that, they will not pick up the rarer variants that may make the difference for individuals.
Studies like Decode ME can illuminate regions of our genome that are particularly notable in ME/CFS. WGS can identify the specific parts of the genes that may be driving it.
Not surprisingly, the study had personal roots. In 2009, at the University of Wisconsin, Liz Worthey PhD had worked in the first group to use whole genome sequencing to diagnose people with mysterious illnesses. The geneticists would come up with a diagnosis and the doctors would follow up with the appropriate tests. Over time she worked on thousands of cases and was able to find a diagnosis for approximately 40% of them.
Skip forward ten years or so, and both she and Camille Birch, PhD were working on a follow-up NIH-funded project called the Undiagnosed Disease Network (UDN) (“Solving medical mysteries through team science”), which also used extensive genetic testing to provide answers for people with mystery illnesses.

Liz Worthey PhD pioneered using deep genetic analyses to explain mystery illnesses at the University of Wisconsin. Later, she and Camille Birch PhD worked at the Undiagnosed Disease Network to do the same.
Meanwhile, Camille Birch’s mother had been diagnosed with fibromyalgia in 1995. Her story was familiar. There were no answers and they kind of “limped along and hoped for the best”. When Camille began her PhD, she began experiencing the same symptoms as her mother. Only by moving to her parents house, and getting rides to and from school, was she able to complete her PhD.
THE GIST
We all carry pathogenic genes. It takes trained genetic analysts to separate the wheat from the chaff.
“I was completely blown away by what I saw”. Camille Birch PhD

- Six years ago, a startling Solve M.E .presentation from Liz Worthey and Camille Birch suggested that rare genetic variants – which are not uncovered by standard genetic testing – may be impacting energy production in significant numbers of people with ME/CFS.
- Various things, including a pandemic, interfered with their follow-up work, but they’re back with their first paper, “Uncovering the genetic architecture of ME/CFS: a precision approach reveals impact of rare monogenic variation“, using an expanded data set.
- Liz Worthey has a PhD in Genetics from Imperial College, London and is the Director of the Center for Computational Genomics and Data Science at UAB School of Medicine. She is a pioneer in doing the kind of complex genetic analyses done in this paper. Camille Birch has a PhD in Biomedical Engineering and is a genetic data analyst. I talked with them in what turned out to be a rather long discussion about their work. (See the blog for the zoom talk.)
- They employed something called “whole genome sequencing” which, in contrast to the usual kind of genetic analysis which assesses a million or so genetic variants, assess the entire genome which includes billions of genetic sequences. This kind of analysis picks up rare pathogenetic genetic variants – usually very small shifts in our genetic makeup – which can affect how our cells function.
- Our DNA, whether we are healthy or not, contains 2-300 pathogenic variants, most of which are not being expressed. A trained genetic analyst will go through each one see which ones fit the patient’s presentation, and that’s what Camille, whose mother has fibromyalgia, and Liz, who came down with long COVID, did.
- Camille noted that while ME/CFS research has been good at illuminating problems with general biological pathways, it’s been less effective at identifying the mechanistic faults; i.e. the specific gene mutations that may, in some cases, be driving those broken pathways. That’s what they were looking for – and that’s what they found in roughly 40% of the 30 people in the study.
- They used an extensive questionnaire to determine if the pathogenic variants found matched the patients’ symptoms.
- Camille expected that they would mostly find very rare genetic variants which little was known about. Instead, they often found rare, but clearly pathogenic variants which had been associated with one disease or another. Note that the pathogenic variants had to meet strict criteria to be considered in the study.
- One possible hitch was that the pathogenic variants found were usually heterogzygous – meaning that the individuals with them also carried a normal variant of the gene. The normal variant of the gene is usually the one that is expressed, but in many cases, illness, stress, toxins, or perhaps just time, can cause the pathogenic variant to be expressed – and this is what they think happened.
- Interestingly, the gene variants – all of which varied from person to person – converged on three main themes: impaired energy production, reduced stress resilience, and vulnerability to metabolic failure.
- Examples included people with pathogenic variants that affected ATP production, fatty acid metabolism, glycolysis, vit. B12 processing, ion transport, red blood cell formation and others. You can read about these case studies in the blog.
- Their findings could be validated by gene expression analyses, metabolomics, proteomics and/or laboratory tests to see if the pathogenic variant was having the effect the authors believe it is having.
- The authors believe that, given the variety of pathogenic gene variants found, personalized testing which does a deep dive into patients’ genome is going to be necessary to figuring out a substantial number of people with ME/CFS.
- Liz and Camille have been able to slowly increase the number of genetic analyses that have been done (they’re up to about 50) and are looking for more funding to do large-scale analyses. In their analyses, they build reports, send them to doctors, and interact with them to help them do confirmatory tests and try the correct treatments at the right dose, etc.
- While they don’t have the capacity right now to increase their rate of analyses, people who are interested in providing their whole genome sequence to them and have their analyses done can reach out to them. Plus, if they can get funding, and you’re interested in being in a study, you can reach out to them as well (eaworthey@uabmc.edu, clbirch@uabmc.edu).
- Finally, when researchers come across outliers – people whose test results really stuck out – they’d be interested in analyzing their genome.
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit
Weird Pushback
As she began doing the genetics work, she began asking: why not sequence her mother? Why not look into fibromyalgia/ME/CFS? They’re mysterious diseases with no answers. She got the kind of weird pushback that just makes you shake your head: “We don’t do ME/CFS/FM because we don’t know what causes it”. (Huh???)
Walking into Liz Worthey’s office, she said, if I can get some money, can we study it? The answer was yes, and a Solve M.E. Ramsay award provided some money. A walk across the University of Alabama campus to Jarred Younger’s office got them patients. Meanwhile, Liz’s connection to these diseases got more personal when she came down with a nasty case of COVID-19 and ultimately, long COVID.
Camille’s first run through of the data revealed little. Not until she discarded all her prior conceptions about ME/CFS and literally went through the data chromosome by chromosome – and included an extensive questionnaire – did things start to pop. It was often the tiny details and weird symptoms that provided the most important clues. Liz Worthey talked about the “little tells” that their questionnaires revealed which turned out to be important clues, some of which showed up before patients actually came down with ME/CFS/FM.
We all carry pathogenic genes. It takes trained genetic analysts to separate the wheat from the chaff.
Our DNA, whether we are healthy or not, contains 2-300 pathogenic variants, most of which are not being expressed. A trained genetic analyst will go through each one to see which ones fit the patient’s presentation.
Camille noted that while ME/CFS research has been good at illuminating problems with general biological pathways, it’s been less effective at identifying the mechanistic faults that are driving those broken pathways.
Take the mitochondria. Something clearly appears to be affecting the mitochondria in some people but we don’t know what. We have a bunch of possibilities but no clear answers. In our talk, Camille described her excitement at finding distinct genetic anomalies that could be affecting the mitochondria in different ways in different patients.
The Study
The study involved 38 people including 31 affected participants and 7 healthy first-degree relatives. Machine-learning and expert review identified pathogenic, or likely pathogenic, variants in 8 of 25 affected probands (the first person affected in a family) (32%) and 12 of 31 affected individuals (39%).
First, they took all the symptoms found in the Carruthers ME/CFS Canadian criteria and produced every symptom-combination that would still satisfy a diagnosis of ME/CFS. Each combination that could do that is called an avatar. They created these avatars in order to use machine learning.
Next they compared the “avatars” to symptom sets present in OMIM-curated Mendelian disorders. These are Mendelian (genetic) disorders caused by variants (mutations) in single genes, and thousands of them exist. They found a hundred and thirty-five genetic disorders which had similar symptoms to those found in the ME/CFS avatars.
The genetic diseases looked very familiar, as they impacted many areas of interest in ME/CFS, fibromyalgia and long COVID. They included disorders of thyroid hormone metabolism, mitochondrial DNA depletion and inhibited oxidative phosphorylation (energy production), fatty acid oxidation (energy production again), muscle excitation–contraction coupling and myopathies (muscle functioning); myasthenic syndromes (muscle weakness disease), kidney functioning, and autoinflammatory or immunodeficiency syndromes.
The close match between the ME/CFS symptom sets and the genetic disorders with pathologies similar to those that are showing up ME/CFS, FM and long-COVID studies was a good sign.
Clear Potential Genetic Causes…
It got better, though. They found what they considered to be a clear genetic cause to their illness in between 30-40% of individuals; i.e. they were confident that the specific gene variations mutations they found were causing the person’s illness.
The gene variants had to pass two tests of pathogenicity to be assessed.
In five more people they identified heterozygous pathogenic variants in genes associated with recessive disorders which may have contributed to the disease. All in all, the whole genome analysis uncovered potentially significant genetic contributions in no less than 55% of the cohort.
Their confidence wasn’t simply based on intuition. In order to be considered possibly causal, the gene variants had to pass two tests. First, they had to meet strict international guidelines called the ACMG criteria, which are used by geneticists to decide if a mutation is actually harmful (pathogenic). Plus, they had to show up in a global database called ClinVar which contains genetic variants that are recognized by the scientific community to be linked to known diseases.
Next, they had to pass muster with expert genetic analysts. The patient questionnaires and narrative histories the authors had the participants take helped the analysts determine if a pathogenic variant was a match for each patient’s symptoms.
Possible Core Dysfunctions Pop Up
As with the avatar analysis, the genetic variants made sense with what we know about ME/CFS and with what patients experience.
Genetic variants that affected energy production and metabolism (ENO3, HADHA, ACADM, MMACHC) and disrupted mitochondrial function, glycolysis, and fatty acid oxidation were found. These variants have been shown to produce PEM, chronic fatigue, muscle pain, weakness, and cognitive dysfunction.
Symptom profiles plus molecular findings. Note how core symptoms (fatigue, exercise intolerance, mental functioning, digestive problems, pain) showed up equally in the different molecular groups – hence the need to do more personalized testing. People in the red blood cell subset had more immune involvement; people in the solute and ion transport subset had more metabolic issues, and people in the energy production subset had more immune and less cardiovascular and headache findings.
Variants that impact solute transport and ion homeostasis (KCNJ18, SLC12A3) impair electrolyte balance, nerve signaling, and vascular tone have been shown to produce exercise-induced fatigue, muscle cramps and weakness, cognitive issues, and orthostatic intolerance.
Variants in red blood cell membrane genes (SPTA1, SLC4A1) have been shown to impair red blood cell functioning, blood perfusion into the tissues, microvascular blood flows and oxygen delivery. They have been associated with chronic and exertion-induced fatigue, muscle pain, cognitive dysfunction, anemia, and pain.
Note that these genetic variants appear to converge on three main themes: impaired energy production, reduced stress resilience, and vulnerability to metabolic failure. Many overt immune findings didn’t show up in this pilot study. Instead, a fundamental problem that could undermine the immune or any other system did.
Indeed, in illnesses that affect many different systems like ME/CFS and long COVID, we’re looking for fundamental problems that could explain all of it, and that’s what these findings seemed to uncover.
A Hitch (or Logical Explanation)? Heterozygous Genes Dominate
There is a potential hitch, though. The authors generally did not uncover pathogenic homozygous variants; i.e. variants which affected both “sides” or alleles of the chromosomes.
Each of our genes feature two branches or alleles. If both branches contain the same gene variant, the gene is homozygous – and we know what it will produce when activated. If both alleles contain different gene variants, the gene is considered heterozygous, and the answer is more complicated.
.svg)
Most of the pathogenic gene variants were heterozygous; i.e. one branch of the gene carries a normal gene while the other carried a pathogenic variant. (image from Ryan Kissinger, courtesy of NIAID, Public domain, via Wikimedia Commons)
Often one variant is considered dominant and the other recessive. In that case, the dominant gene variant will usually carry the day. Other times, there will not be a clearly dominant gene.
In general, though, the recessive gene variant is not expressed. In several of the gene variants, it was clear why some homozygous pathogenic genes were not found – people with both variants become ill or die very young. (Two of my gene variants were of this type.)
In most cases, it was a heterozygous, recessive (not usually expressed) gene variant that showed up in the ME/CFS patients. So, why would these authors argue that they are being expressed and are contributing to ME/CFS patients’ illnesses?
Because infections, illness, toxins, stress and other factors can sometimes result in these heterozygous recessive genes being expressed. Plus, the fact that the impact of these recessive genes can show up more and more over time could fit later stage illnesses.
Plus, while it’s easy to identify the effects of homozygous variants when a child with them is ill or dies young, it’s more difficult to identify heterozygous variants whose impacts show up decades later. In some people, ME/CFS may be a genetic disorder which takes: a) decades to show up; and/or b) requires a stressor to be manifested.
Camille pointed to a disease called Charcot-Marie-Tooth which contain hundreds of different genetic subtypes. In the more severe forms, children lose their myelin, their ability to walk, by the time they are ten, and can die. In other genetic subtypes, people can retain their ability to walk until their 70s or 80s.
The medical field has been very good at investigating catastrophic genetic variants but not so good at understanding the impact of less catastrophic variants. Despite the fact that the parents contribute the genes that cause these catastrophic illnesses in children, genetic studies often don’t examine the effect they might be having on the parents. Do they have fatigue or pain or other problem?
Case Studies
It’s important to note that Camille and Liz were constrained by our knowledge of pathogenic variants. Some of the variants that may be operating in ME/CFS patients simply haven’t been studied enough for us to know they’re pathogenic. (The authors provided a list of them in the paper.) Camille initially thought these rare, largely unstudied variants would make up the bulk of their findings, but said she was blown away by how many well-established pathogenic variants they could match to the symptoms the patients were reporting.
Check out some of the gene variants they found. Note that validating the authors’ findings would require doing gene expression/proteomics studies and/or lab tests to determine if the pathogenic variant is having the suspected effect. (Even then the lab tests may not be decisive if the gene variant is doing something a bit different in ME/CFS.)
This, in fact, is what the authors wish to ultimately accomplish. They want to generate genetic reports that patients can give to their doctors which then suggest tests that can be used to verify the findings, and, suggest treatments.
Cellular Engine Offline
Participant 5 carried a “pathogenic frameshift variant” in ENO3 (β-enolase). A pathogenic frameshift variant is a genetic variant which shifts the protein’s “reading frame” in such as a way as the cell produces an incomplete protein. In this case, a glycolytic enzyme that affects mainly the muscles was becoming shortened. This genetic mutation prevents the glycolytic cycle from producing a high-energy factor called PEP that’s needed to produce ATP.
This pathogenic variant affected ATP production.
When this happens, ATP production falls and is particularly impacted during strenuous exertion. It’s like operating an engine with a cylinder that fails when its put under stress. The result is pain/cramps, early fatigue, muscle damage, weakness (especially with intense/anaerobic bursts).
The fact that this patient reported prolonged post-exertional fatigue, weakness, pain, cramps, spasms, and tenderness indicated that her symptoms were largely a match for this genetic variant. Notice that muscle cramps are not always found in ME/CFS.
The gene in this case was heterozygous and recessive; i.e. it carried two alleles, one of which was normal and is usually dominant. As we’ll see with some other variants, the authors noted that the recessive pathogenic gene can show up after illness or stress. Potentially, it could produce partial reductions in glycolytic reserve and set the stage for exertional intolerance and PEM. Plus, this gene’s high CADD score (35) suggests that this genetic variant has the potential to be particularly dangerous.
A follow-up lab study would look for elevated creatine kinase (CK) and myoglobinuria and decreased ENO3 activity.
MCADD (Not MCAS) Shows Up in Mother and Son
Participants 7 and 8 (mother–son) shared a pathogenic ACADM missense variant called ACADM p.Leu84Phe. (A missense variant changes one amino acid in the resulting protein. In this case, the 84th amino acid in the protein is changed from Leucine → Phenylalanine.)
This variant affects a different part of the energy production process – fatty acid oxidation – and can produce something called medium-chain acyl-CoA dehydrogenase deficiency (MCADD). Fatty acid oxidation problems have shown up repeatedly in ME/CFS metabolomics studies.
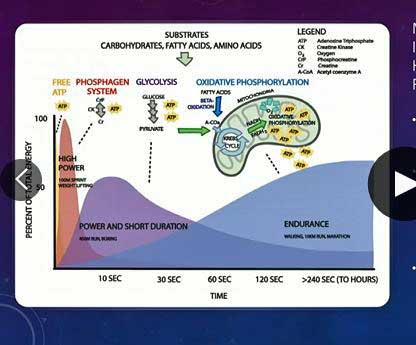
Cells should switch to breaking down fatty acids for energy during exercise. This pathogenic variant inhibited that from happening.
In fatty acid oxidation, fats (triglycerides) are broken down into acetyl‑CoA which then feeds the TCA cycle. This cycle provides the electrons needed to run the electron transport chain and produce ATP. In MCADD, the body can’t reliably break down medium-chain fats for energy. When an MCADD deficiency is present, people have trouble switching to using fats as fuel, and so lose an important energy source.
Because fatty acids are the body’s most efficient long-term fuel source (they provide more ATP per gram than any other fuel), MCADD can produce episodes of fatigue, weakness and exercise intolerance. These episodes are often triggered by illness, prolonged exertion and fasting.
This variant was again heterozygous; i.e. it occupied one of the two alleles for the gene and is not usually deleterious. Illness and exertion later in life could conceivably trigger this variant to produce symptoms.
In order to tell if this variant was contributing to their illness, tests like plasma acylcarnitines and urine organic acids taken during/after a stressor would be taken, which brings up something else the authors pointed out – the need for strategic lab testing. They note that “biomarkers may be missed if samples are taken outside periods of active disease or relevant exposures”; i.e. some tests should be done when active disease (a crash) is present and/or after a relevant exposures (stress/exercise).
My acetylcarnitine tests, for instance, were done while I was at baseline. I had one abnormal result, a couple of low/high normal results, and mostly normal results. An AI search suggested, though, that exercising 2-6 hours prior to the test might have provided more revealing results.
Fatty Acid Metabolism Again
Fatty acid problems are showing up in spades in studies and in this cohort of patients. Given what we know thus far, it seems likely that a prominent fatty acid metabolic subset exists. The pathogenic HADHA variant found in one patient affects the final steps of long-chain fatty-acid β-oxidation, and therefore energy production. A homozygous deficiency typically results in fatigue, muscle weakness, PEM, muscle spasms, nausea, and exercise intolerance.
This variant is, again, heterozygous and does not usually cause problems, but once again, the literature states that stressors such as illness, fasting, or pregnancy can cause this variant to produce problems. The patient’s symptoms (fatigue, PEM, weakness, pain, muscle spasms, sensitivity, and nausea) seemed to fit this variant well. Plus, the authors pointed out that this person had other variants (NLRC4, SLC16A3, and SLC12A9 genes) that might be contributing to inflammatory, muscle, and metabolic problems.
Muscle Problems
Two siblings carried a “likely” pathogenic SLC12A3 frameshift variant. This gene linked to Gitelman syndrome, which produces metabolic alkalosis and muscle weakness, cramps, pain, fatigue, hypovolemia, polyuria, and exercise intolerance during illness, fasting, or exertion.
While the variant was recessive, once again reports have suggested that people with heterozygous forms of this gene can exhibit similar symptoms, and indeed, both of the siblings reported symptoms such as muscle weakness, joint pain, cramps, chronic fatigue, severe overactive bladder (suggestive of polyuria), and exercise intolerance.
One of the siblings contained a pathogenic COL6A3 variant, seen in something called Bethlem myopathy and Ullrich congenital muscular dystrophy, which could explain the greater levels of pain, fatigue, and musculoskeletal problems this person experienced.
Stiff Red Blood Cells
A mother and two daughters carried a fascinating variant given what we know about ME/CFS. The pathogenic splice SPTA1 variant found produces a protein called a-spectin which is essential for red blood cell flexibility and deformability,
A mother and her daughters carried a pathogenic variant that could stiffen their red blood cells, potentially resulting in exercise intolerance, etc.
These variants can produce fatigue, PEM, shortness of breath, exercise intolerance, dizziness and pain that is often triggered by exertion or infections. Plus, these individuals also contained more pathogenic variants which may exacerbate the SPTA findings.
At least 3 studies have found problems with red blood cell stiffness/deformability. Red blood cells that are too stiff may have trouble getting into the capillaries and delivering oxygen and nutrients into the muscles.
Interestingly, red blood cell-driven PEM (occurs more quickly, peaks during or shortly after exercise, clears up more quickly) may be different from mitochondrial produced PEM (shows up later, takes longer to resolve).
B12 Gene Mutation
Participant 18 carried a pathogenic frameshift variant in gene called MMACHC (p.Arg91LysfsTer14), which disrupts vitamin B12 processing and mitochondrial functioning. Jarred Younger explained that because this gene disrupts B12 processing, people with normal or even high B12 blood results might not be getting enough B12 in their cells.
My Results
I was in the 40% or so of people whom Liz believe may have a genetic basis for my illness. (I was not in the paper. I have a healthy identical twin, but while identical twins are genetically very similar, they are not genetically identical. He is being tested to see if we differ in important ways.)
I had 7 pathogenic variants that could be hyperactivating the immune system, impairing energy production, affecting the muscles, and contributing to or producing ME/CFS.
My results included genes that might be activating the immune system and impairing mitochondrial production.
One (FLG NM) results in an incomplete gene, which can produce a hyperactivated immune state that requires a lot of energy. That gene paired nicely with a mitochondrial gene (GLDC NM) which could reduce energy production, and can produce a later onset of fatigue, PEM and liver issues.
A small change in one gene which produces an enzyme called GDP‑mannose pyrophosphorylase B, particularly affects proteins in the muscles. Recent research suggests that a single copy of this gene can give rise to later disease states that result in muscle weakness, later onset fatigue, pain and post-exertional malaise. A large variant in one gene (CLCKNKB) could result in low blood volume; producing fatigue and muscle weakness.
If two of my variants were found on both branches of my genes, I likely would have died as a child. Interestingly, given my northern European background, two of my gene variants occur mostly in northern Europeans.
Validating the Findings
Validating the authors’ conclusions would involve doing gene expression, proteomic, metabolomic and/or clinical laboratory testing. Gene expression tests would determine if genes associated with the putative problems were affected. For instance, problems with red blood cells might result in a compensatory reaction that involved an increased expression of gene involved in maintaining red blood cells – and this was found. Similarly, the expression of glycolytic and mitochondrial genes was altered in some people carrying pathogenic variants involving the mitochondria. Ditto with some patients who had variants affecting the innate immune system and regulatory T-cell networks.
Next Steps
Talk about precision medicine. While the authors acknowledged that studies with large samples are important, they believe that in illnesses like ME/CFS where many roads can lead to Rome, taking a deep dive into symptoms and family history and pairing that with a deep dive into the entire genome may be critical. Indeed, the fact that the authors were able to present plausible explanations for about 40% of the participants (note that some families were included, which drove up the percentage) suggests that these precision-guided approaches may be a necessary component for a substantial subset of patients.
Jarred Younger Talks About This Study
The authors believe ME/CFS exists on a kind of gradient. The common genetic variants uncovered by studies like the Decode ME study will help explain some types of ME/CFS. Others will be explained by rare genetic variants that can only be uncovered by analyses of the entire genome.

The authors hope to expand their testing and provide doctor reports that can help inform treatments.
The fact that whole genome studies are so rare in ME/CFS in the history of ME/CFS makes one wonder if the medical field is ready for a genetic explanation of ME/CFS. Note, after all, the bizarre reaction that Camille Birch received when she first proposed that the rare illness program study fibromyalgia. (We don’t know anything about it, so why study it????) (Note also, how important a patient organization – Solve M.E’.s Ramsay award – was in getting this research started.)
This paper is just the beginning, one hopes, of more deep dives in the genetic maze that makes up ME/CFS. One piece of good news is that the price of whole genome sequencing has gone down dramatically over time. I paid $369 for a whole genome sequence from sequencing.com and then gave it to Liz and Camille to analyze. The Decode ME group has announced that a whole genome study is in the works.
Liz and Camille have been able to slowly increase the number of genetic analyses that have been done (they’re up to about 50) and are looking for more funding to do large-scale analyses. Ultimately, they would like to build reports, send them to doctors, and interact with them to help them do confirmatory tests and try the correct treatments at the right dose, etc.
While they don’t have the capacity right now to increase their rate of analyses, people who are interested in providing their whole genome sequence to them and have their analyses done can reach out to them. Plus, if they can get funding, and you’re interested in being in a study, you can reach out to them as well (eaworthey@uabmc.edu, clbirch@uabmc.edu).
Finally, when researchers come across outliers – people whose test results really stuck out – they’d be interested in analyzing their genome.
- *Coming up next – “The Study We’ve All Been Waiting For?”



Interesting study. My mother had ME/CFS for a relatively short time, I have had it for 35 years (albeit at the more mild end of the spectrum) and my 18 years old daughter has had it for 2 years. So I guess there is something genetic at play.
So that test you did Cort would show up all the sorts of things they looked at?
While I am sorry for your situation of having 3 generations with ME/CFS, it gives insight in heredity and the role of mitochondrial DNA:
* Mitochondrial DNA is inherited from the mother, not from both parents. If your wife hasn’t got ME/CFS, then the main cause in your 3 generations of ME/CFS doesn’t look to be dominantly caused by “faulty” mitochondrial DNA.
The working of mitochondria is influenced by the other non-mitochondrial DNA and environmental conditions too, but this insight opens up a very simple ability to study the relative impact of ‘pure’ mitochondrial DNA itself in ME/CFS:
If researchers find enough parent-sibling pairs with ME/CFS, they could score them for disease severity and then splitting them into two groups: mother has ME/CFS too or father has ME/CFS too (and none or both too for completeness). Then take into account how much more prevalent ME/CFS is in females versus males and one could have quite a good understanding of how big the role of ‘pure’ mitochondrial DNA inheritance is.
Simple and relatively cheap to do. I never have seen such research however. Maybe Keep It Simple could help research just as much as advanced tech?
Translation error. Parent-child pairs instead of parent sibling pairs.
Also, to differentiate from sons inheriting Y genes from father, the child groups have to be split into male – female too. Still, all in all it IMO would mainly be a survey type research where scoring the ME/CFS severity as correct as possible plus getting data gathering unbiased (e.g. without selection bias) and good knowledge of statistics would be the main difficulties in this type of research.
It’s not just mitochondrial dna being the problem tho. The whole point is that there are many many different dna errors which can cause the symptom spectrum.
Yes, indeed. The key thing for me was that different errors in say energy production can cause the same general symptoms but often there some, probably missed symptoms, that were different, and helped with the diagnosis.
Hi cort, based on this study and findings are there anything that can help us with energy production and cognitive improvement. I guess I am asking any solution to improve the symptoms?
I do not doubt that it isn’t just about mitochondrial DNA. I tried to make a case for:
* It IMO should be possible to determine how big the relative impact of inherited mitochondrial DNA is in ME/CFS prevalence and severity.
* It should be possible to do so in a relatively simple and affordable way.
And, something I failed to make very clear in what I wrote:
* It IMO would be of great value for determining optimal research funding.
If we had reliable numbers on how big the impact of a few possible / suspected key components (such as how big is the role of inherited mitochondrial DNA, MCAS, mucus genes…) is, then research could IMO be sped up quite a bit. Up to today that still is largely a big question.
For each one of these questions answered, there is the potential to find better answers more quickly. Complex omnics and full genetics is one part of it. Smart use of existing data to extract information (like I suspect is possible with the relative importance of inherited mitochondrial DNA) is an overlooked part and IMO low hanging fruit.
I think the results could eventually point to more options for treatments based on the DNA results. Currently, we have so few treatment options available for such complex conditions. Most treatments center around reducing pain and perhaps helping patients sleep, but so much more needs to done to improve patients’ functioning, as these illnesses reflect such varied dysregulation.
When we do “whole genome” sequencing, we actually get very deep sequencing of the mitochondrial genome too. We look in there as well as in the nuclear genome. Knowing the actual variant is important too. The nature of the variant can impact when and how the disease arises (e.g. whether a second variant is needed for disease to occur).
Question – despite genome variations, which could potentially contribute to ME/CFS symptoms, I imagine there could still be an effectively universal causative factor of ME/CFS that applies to everyone? And further question – some things found in the tests might be treatable, and therefore help if not cure the ‘umbrella’ ME/CFS? Cort did your tests show up anything treatable?
The universal causative factor was discovered about 2010 by Dr. Judy Mikovits at University of Nevada Reno Microbiology and Immunology lab. She determined that primarily XMRV and HTLV, HIV and HERV retroviruses were transferred to ME/CFS victims via contaminated inoculations**. RNA epitope retroviruses integrate into a host cell’s genome via reverse transcriptase and thus corrupts the latter’s genome that intern expresses maldesigned mitochondria that produces deficient amounts of ATP, and thus ME/CFS.
** Vaccine antigens are all cultivated from animal soft tissue such as from mice and hamsters, etc. The latter tissue is often contaminated with undetected retroviruses.
Judy is back! I lived through the XMRV saga. Here’s the thing – researchers were very interested in finding another retrovirus that possibly infected humans – no surprise there given that HIV is one. Retrovirologists could have made hay off of XMRV for decades- but what happened? Interest evaporated.
The most recent major paper on XMRV was “False Alarm: XMRV, Cancer, and Chronic Fatigue Syndrome” published in 2024. https://pubmed.ncbi.nlm.nih.gov/38976866/
The next one was
Fake Science: XMRV, COVID-19, and the Toxic Legacy of Dr. Judy Mikovits.
Neil SJD, Campbell EM. – https://pubmed.ncbi.nlm.nih.gov/32414291/
Everyone wants there to be a simple answer but the truth is that virologists would have loved to have a new human pathogen to study and if it had worked out they’d be studying it still.
Oh that old chestnut
the search for the magic virus!
How much time and money was wasted on that as well as the elusive immune dysregulation (note – I do think the immune system is involved to some extent).
Hello, Cort
The fact remains that mutated or contaminated DNA causes chronic and autoimmune disease. The host cell’s DNA repair mechanisms do not function if the host cell’s 3.2-billion nucleotide DNA is contaminated by one or more “smart” 8K nucleotide retroviruses that are integrated into the DNA molecule. Thus, despite attempted repair, the disease remains.
Subsequently, the prevention of chronic and autoimmune disease is to eliminate the source of the retroviruses. One is contaminated vaccines. If Cerus Intercept Blood System can sterilize blood in blood-banks, someone ought to be able to determine how to neutralize retroviruses that contaminate vaccine formulas.
Unfortunately for Judy, she unintentionally almost interrupted the multi-billion dollar for-profit vaccine-industry corporacracy juggernaut.
Yes, but Randy, remember that the XMRV virus was found only in the samples from Dr. Mikovits laboratory, and it came from mouse DNA that got into the samples.
XMRV was created when two mouse viruses combined (recombined) while being grown in human prostate cancer cells for research. It didn’t exist in nature before that but more importantly it is not infectious; that is, outside of the lab it’s never been found to infect humans. The only lab that found it was Dr. Mikovits lab – because her lab was the one that got contaminated.
I don’t know how vaccines got into the discussion but Dr. Mikovits reputation was essentially destroyed by the XMRV saga when she accused scientists of being against her, claimed that XMRV was going to be more dangerous than HIV/AIDS, is found in mother’s milk, told patients not to cooperate with SolveME, and couldn’t complete a very basic test during the last study, etc..
This email addresses two subjects. 1) Why does no one have a problem with Covid causing Covid and Long Covid, but they think that a single virus can’t cause ME/CFS?
Of course, affected people have different symptoms. As the former head of NIEHS said “genetics loads the gun and environment (in this case maybe a virus) pulls the trigger”. A person’s genetics will determine the symptoms they have although a similar trigger may create overlapping conditions.
2) Back to Covid. I have had Long Covid with heart and blood pressure involvement since 2023. I thought these problems were resolved until I passed out in October. My cardiologist, a very smart man, ran an EKG, ECHO and 7-day Halter monitor. My heart was physically fine but the electrical system had gone haywire. In 7 days, my heart ran up to 200 bpm 28 times. This didn’t correlate with any particular activity. I am now on a beta-blocker (these have been useful in Long Covid patients) and I will see another cardiologist who specializes in electrophysiology later this month. Other than passing out, I never noticed any symptoms. These problems have been reported in other Long Covid patients, but not all. Long Covid should be your roadmap into investigating the cause of ME/CFS, not trying to find myriad things that could cause it. By roadmap, I mean a known cause with different outcomes in different patients.
Hello, Cort
In my opinion, it appears that you’ve been compromised by the apparently sinister leaders/protectors/collaborators of government public health entities (both Britain and USA) whose job it is to assure public confidence in both the blood supply and vaccine safety. Indeed, anyone who accuses the former of malfeasance shall be vilified and discredited. That’s just the nature of how sinister politics can be against scientists whose goal is to improve the health of humanity, that is, vilify the messengers in order to suppress the facts of their discoveries.
Both Dr’s. Judy Mikovits and Frank Ruscetti have preserved their lab data that supposedly was incinerated. Additionally, a full sequence of XMRV was obtained in addition to liquid nitrogen samples of B cell lines and patient samples.
BTW, the contamination you are referring to indeed occurred in Building 535 at the National Cancer Institute in Frederick, Maryland. It occurred when collaborators/subversives contaminated a fermenter containing a natural isolate of XMRV by placing it next to a fermenter containing VP62 (and NOT at July’s lab at University of Nevada Reno).
No need to reply since it won’t change the facts of the matter.
The thing about conspiracy theories is that there’s no end to them. If the scientific community considered XMRV a threat they would have been more than happy to spend the next ten years learning everything about it. Remember the last retrovirus to infect humans was HIV, so there was huge interest in XMRV. Their lack of interest may be the best evidence that XMRV was/is a lab contaminant that is able, under certain conditions, to infect cultures but does not impact humans.
Did you know there was a form of non-HIV AIDS? Idiopathic CD4+ T-lymphocytopenia (ICL) is a rare immune disorder known as “non-HIV AIDS,” characterized by severely low CD4+ T-lymphocyte counts and opportunistic infections in the absence of HIV.
In the beginning of ME/CFS, the CDC monitored a number of these patients and Dr. Cheney had many as well. This was quickly shut down at an international conference.
You won’t be hearing about this or the “unfairly” discredited XMRV because no one wants to “panic the public”.
Waste time and money probing genetics. All illness has a genetic component, but that is not the triggering cause.
ME/CFS patients aren’t allowed to donate blood. More than one study has found “something in the blood” of ME/CFS patients. Transmissible? Oh no, don’t panic the public.
With all due respect to these intelligent, articulate and well-meaning ladies, their research isn’t going to get you any closer to the cause or potential treatment of ME/CFS.
I have had ME/CFS since 1985 and Long Covid since 2023. Believe me, these are not the same. How does genetic research explain this?
I got to see the XMRV debacle from a unique position.
Working in Dr Judy’s lab as a volunteer.
Actually, according to their IRB they cannot give the report directly to me – it has to go to the doctor first – and the she has to give it to me. They’re having a little trouble getting it through to the doctor, so I don’t know! I would be a bit surprised actually but time will tell.
Sorry I don’t follow. In the article you talk about your results , including 7 pathogenic variants. To be clear I am talking about the genome study you said you did
I was also wondering about treatments for deeper issues indicated by these genetic tests. For example, B12 (if it’s a ‘regular’ problem of absorption as indicated by low blood B12 levels, this can, as we know, be treated by very high oral doses or by injection) – can the problem of downstream metabolism somehow be treated?
Feature
Why covid-19 is “a vascular disease masquerading as a respiratory one”
New study in prestigious British Medical Journal
https://www.bmj.com/content/392/bmj.s31
I like it! I think this guy will add muscles to his list at some point. ““The virus enters through the airways but exerts its systemic effects through the vasculature, the common denominator in the lungs, heart, kidneys, and brain,” “
Since I’ve already been diagnosed with several genetic defects (detoxification, cholesterol, and another one that can’t be directly attributed), I would very much like to have this test done. Unfortunately, I can’t afford it right now; with a severe disability of 50% and care level 2, it’s impossible for me to manage as a single person. Perhaps one or two of you could share my fundraising appeal. Thank you very much. Of course, I would keep you informed about everything and disclose the results.
https://spendenaktion.de/spendenaktion/me-cfs-kosten-fur-einen-genexpressionstest/-61422
Good luck. I hope you can raise the funds 🙂
So interesting! I had my whole genome run last year, and I’ll reach out to them. I had a few genes with “high confidence” that indicated an illness that was, in their words, “not yet defined.” Curious as to how they determined that a gene caused illness when there was no definition for it. Wondering whether it is one of the genes they found, particularly since I had a juvenile onset illness.
Interesting. “not yet defined” So there was strong evidence that something pathological was present but they couldn’t pin an illness name on it (?). If that’s right it sounds like they found quite a bit. I hope Liz and Camille give it a shot!
I found this interesting that Charcot-Marie-Tooth was mentioned. I have had my WGS done (by Nebula and I’ve run it through Sequencing and gene.iobio) and I have a heterozygous pathogenic GDAP1 variant. If I’m understanding this study correctly, this means that I could have symptoms of CMT although I do not have the homozygous variant? I also have five VUS variants in other CMT genes, for both types 4A and 2K.
I think I might reach out and see if they’d be interested in my WGS data for their research.
I hope you do, Melissa…I think they’d love to talk to you.
Thanks, Cort! I sent Dr. Birch an email.
“Inclusion criteria required a confirmed diagnosis of ME/CFS meeting the Fukuda 1994 definition [16], with additional cutoffs for moderate fatigue severity and frequency proposed per Jason and colleagues (2014) to reduce misclassification [15]. Whilst not used for inclusion/exclusion criteria, all participants also met the Canadian Consensus Criteria (CCC) criteria [17]”
Why not just use the CCC as inclusion criteria? Fukuda1994 is obsolete. It doesn’t need to be used.
I don’t know. It was good to see, though, everyone met Canadian Consensus Criteria (CCC).
Thanks for reporting on this, Cort. I’m wondering if this group plans to publish findings on fibromyalgia too or did they only focus on ME/CFS? I think this is a very plausible reason why we see so many subgroups with variations in their illnesses in ME/CFS, FM and long COVID, if it’s due to different underlying gene variants triggered by whatever stressor.
Camille Birch’s mother has a long history of fibromyalgia. I think they’d love to dig into FM if they could get the funding. Health Rising did a big post on a FM genetic study which strongly suggested genetics were playing a role.
https://www.healthrising.org/blog/2025/10/20/brain-fibromyalgia-genetics/
Plus, there was an earlier family study – https://pubmed.ncbi.nlm.nih.gov/15022338/ and there are other studies suggesting that widespread, chronic pain has a strong genetic component.
Let’s hope both ME/CFS and FM get their due.
We have enrolled patients across the spectrum for this very reason Emily. Different genetic risks combined with different triggers and other health situations. Happy to discuss further if interested. Just drop me a note.
Interesting study, but too little direct relevance to evidence-based, tailored, interventions. When does the promise of improving patient’s lives start?
This again this edition of Health Rising feels a bit too much like a marketing campaign for research participation, instead of what it used to be; a reliable science blog about ME/CFS.
Harold, this is a great piece of journalism, which Cort is known for – it’s about exciting scientific research directly relevant to us and even includes an in-depth interview with the 2 key researchers. (If you haven’t watched the video interview yet, I encourage you to do so – even if you can only watch a portion of it. These two brilliant researchers should be applauded for their ingenuity, hard work & perseverance.)
Not only that, both researchers have an important personal connection to these kinds of diseases.
Furthermore, there’s even a plan to create reports with testing & treatment suggestions for patients’ doctors, and then collaborate with them directly on fine-tuning the doses – directly addressing your question: “When does the promise of improving patients’s (sic) lives start?”
I’m not sure what more you’d want?
If you don’t want to participate in the research, then no-one is forcing you to. I believe plenty of patients would jump at the chance. I welcome being notified of the opportunity to participate in research about our “mysterious” conditions.
“great piece of journalism”?
Clearly you have no idea what “great journalism” is. This is a summary – which is fine — plus a marketing campaign — which is questionable, just like your pattern of reflexive defensiveness. Stick to the facts and don’t make these matters personal — that is what adults do.
I count 4 personal attacks in your reply. Please keep it civil.
“too little direct relevance to evidence-based, tailored, interventions. When does the promise of improving patient’s lives start?”
I almost feel like we’re reading different papers. The new thing about this study vs other ones is that instead of identifying broad themes they believe they’re uncovering precise and determinative factors that are contributing to/causing illness. That’s pretty tailored!
This paper was not about interventions but that’s where the next step lies. If a person has a fatty acid metabolism issue, for instance, they would try to enhance that part of the energy production pathway.
This support research by paying for tests is a new thing but I like it. Many research projects are dependent on patient funding and I see these studies as simply a more direct way of doing that, plus in contrast to most studies, both in both the Amatica and the whole genome sequencing work you get the benefit of moving the science forward, and getting personalized data about your illness.
Yes, but we have been hearing about “next steps” for decades. Great for professional researchers, but not so great for patients.
It is what it is. We have to value something rather than nothing. And these studies are the foundations of what you’re/we’re all asking for. If there’s no foundations, we need to value people who are putting the foundations in place.
I agree with Harold
Health rising seems to have switched from “finding the smoking gun” to
Treatment Drugs to mask symptoms which has already been going on for decades.
All I’ve heard for decades from doctors is… ” we don’t know the cause so all we can do is treat the symptoms”
Nothing new, nothing changed
What we are doing is absolutely research, and you are right to say that. But our primary goal is not a distant, abstract research output; it is truly a drive to help patients who are sick now. This is drive is why I have spent my academic career working in the rare, undiagnosed, or misdiagnosed space in academia. And why we work in this space even though financial support is lacking, sadly.
I genuinely believe that for at least some individuals we have and will continue to identify real underlying causes and, from that, more rational paths forward for care. We will not succeed in every case (assuming what we believe to be the complexity in causes for ME/CFS is born out), but the motivation is very much patient-centered.
Many people in the group have been profoundly impacted personally or through family members by this illness, so we bring both personal urgency and unfortunately – a very clear sense of what is at stake.
Your critiques are important; they help us do better work and stay authentic. I just did want you to know that we really are invested in this work. We hope to generate the interest and the initial findings to get more people involved and interested.
This sort of seems like bad news. How are the activated, recessive genes supposed to be turned off or flipped back?
Some genetic diseases do have treatments. Others rely on management. And some will have treatments in the future. I guess time will tell. Gene therapy including CRISPR is making it possible, for instance, to turn genes off or on, edit mutations, there is also diet modification for some genes,, using enzymes to provide the missing factors, using drugs to make proteins work better.
Since, illness can turn on these recessive genes, it’s possible that nudging the body back to health by treating these genes could allow them to turn off as well.
When there is heterozygosity for a pathogenic gene variant, it often isn’t turned off. The genes are recessive *for the disease that results from homozygosity* for the gene variant, but that doesn’t mean that the gene variant (necessarily) is silenced, or that it doesn’t have some impact.
Lots of heterozygous pathogenic gene variants leads to reduced capacity in functions. I think it’s fair to say that they normally do. It’s common that the pathogenic variant is equally expressed (used for protein building) as the non-pathogenic one. But it may be that half the capacity is enough for full function, as long as the cell or the body isn’t under too much load/stress. Sometimes the pathogenic variant isn’t totally dysfunctional, so that the capacity lies somewhere between 50 % and 100 %. A lot of times overload in some functions doesn’t lead to big problems either since there is a lot of redundancy in the system at large. A lot of times there is an upregulation of the gene to compensate for reduced function – but still half of the gene expression is dysfunctional.
(What is functional and what is dysfunctional isn’t always as clear cut either. Sometimes a gene variant that is be pathogenic in some situation has advantages in some other way.)
Hi Cort,
Before I posted “Uncovering the genetic architecture of ME/CFS: a precision approach reveals impact of rare monogenic variation” on Phoenix Rising, I spent considerable time comparing my DNA results from 2010 with a second test performed in 2020. I then ordered an updated analysis that included markers (RS) which had not been evaluated previously.
In short, I observed differences suggesting that certain genes may have been switched on or off-silenced over time, likely influenced by environmental factors (viruses, bacteria, ect) and regulatory mechanisms. This aligns with Prof. Sapolsky’s teaching https://www.youtube.com/watch?v=YWrPauqthWE&t=1535s (starting around minute 14:35), which explains that much of DNA functions as a regulatory system, where environmental signals can activate or deactivate gene expression rather than changing the genes themselves.
“About 95% of DNA is non-coding DNA, which does not produce proteins. Instead, it contains switches that turn genes on and off. These switches control when a gene starts or stops making its protein.
Signals from the environment, including conditions inside the cell like low energy, can activate or deactivate these switches. For example, a signal can turn on genes that help the cell absorb more glucose when energy is needed.
This shows that non-coding DNA acts as a control system for gene activity, allowing the environment to influence how genes function. This is also the time when other hormones become active, as they interact with these switches to regulate gene activity.
THanks for explaining that Sieglinde.
“much of DNA functions as a regulatory system, where environmental signals can activate or deactivate gene expression rather than changing the genes themselves.”
This explains, I imagine, how recessive genes can get turned but also how if we can turn things around, the environment will call for different, healthier forms of gene expression. To my mind, it’s hopeful 🙂
You are right, Cort. It is possible to trigger the off-and-on switch to function.
To do so, we need to identify the exact trigger or diagnosis—the underlying cause that changed the switch.
Hi Cort. Outstanding medical journalism, as always. Congratulations on this article and the excellent video interview. Having followed you for 8 years, it feels to me that a breakthrough has finally been made in understanding some of the mechanisms that cause ME/CFS symptoms, and why there is such heterogeneity. With all your years of investigating ME/CFS, do you feel the same? I would appreciate your input as I intend sending this article and paper to some senior people in the medical field.
Thanks, Di 🙂
It does feel like we’re on the cusp of something. It seems like the general mechanisms are becoming clearer and that what’s next is finding the precise problems. We’re not there yet – and that is not an easy thing – but its encouraging that researchers like Liz Worthey and Camille Birch, and research groups like Precision Health, Amatica, Ian Lipkin, and the Open Medicine Foundation (See the next blog) believe we can get there. It always seems to take longer than we would want but I think we’re in a better place. 🙂
I watched this video (or rather, listened to it while lying down) when Cort posted it. Being such a long interview, I wasn’t expecting to be able to cover the whole thing in one session, but it was so interesting the time flew by. And I’m utterly blown away by Cort’s ability to bring together all that information in this blog. Cort, a big shout out to you on your talent in doing this, especially so when you are ill yourself. So appreciated!!!
I’m so glad that you watched it and enjoyed it Fay. I’m worried that the length will put people off but these women are so articulate and down to earth that the interview just flew by. I was astonished at how long it was (lol). Thanks for sharing that 🙂
Ordered from sequencing.com and will give the results to Liz and Camille. Thank you for the reporting!
🙂 🙂 🙂
Can any of us submit results to Liz and Camille?
Yes please feel free to reach out!
Yes please feel free to reach out to the email below.
Hello Liz,
First off, a gracious TY for your amazing work. I am interested in “reaching out”. Can you tell me if that would include personal genetic testing and analysis?
Please explain what options I have to acquire a genetic analysis, and to potentially be of help. Please include any financial costs that I would be expected to bear, as I live on a limited fixed income.
I have quite a personal story of CFS symptoms that I believe were there since childhood, but did not become overtly clinical and severe until age 30. I am now 70 years old. I also have a long list of rather mysterious secondary symptoms affecting my gastro, immune, endocrine, neuro and (I believe) vascular systems. The cause(s) of these multi-system symptoms are unknown, but I have always attributed virtually all of them to the same underlying cause(s). I also have some unusual health challenges not commonly associated with CFS – that I also believe are part of the same core root problems. My health challenges have produced many abnormal symptoms and test results, but their cause(s) have been unexplained by clinical medicine, with no effective treatments found to date. I perceive that these symptoms could very well be genetic, and have been impossible to otherwise explain. I could provide much more detailed information, if desired.
Thank-you for your considerations and response.
With warm regards,
David Ward.
Hi David.
Please drop me a note at my email eaworthey@uabmc.edu. I can share some info with you.
Yes this would be a personalised analyses and genetic; a whole genome or perhaps an “exome”, which is essentially just the protein coding proportion of a genome.
We are not asking for any financial input – in fact; I’m trying to work out if I can find someone who can hep cover sequencing costs for folks who cannot afford it. Still looking into this.
Happy to chat!
Thanks for reaching out.
Liz
Hello Liz,
In response to your invitation above, I sent you an email expressing my interest in participating, to eaworthey@uabmc.edu on March 8th.
I have not yet received a reply. May I ask, did you receive my email?
With regards and thanks for your response,
David Ward.
Hi Dave. Did you get a response as yet? If not; could you resend a message.
So…..these two amazing women have provided us with what appears, at last, to be a ground breaking concept. (I want to actually say a that they have found the definitive answer…..) What was so very stunning to me is that Camille spoke of having to broaden her view of what she was looking at in her data, whilst doing her analysis. She in essence checked her own bias, and as such with her meticulous attention to detail she was able to establish these results. She is clearly an exceptional analysist.
I’m left wondering now about the DECODE project….. so many millions spent on that, yet these two shero’s, whose research findings can offer us the potential for real practical medical help right now, are grappling for funds to develop next steps.
I pray that someone will step in fast and fund these two to create a plan to roll out a next step so that can all see some light at the end of the tunnel.
“What was so very stunning to me is that Camille spoke of having to broaden her view of what she was looking at in her data, whilst doing her analysis. She in essence checked her own bias, and as such with her meticulous attention to detail she was able to establish these results. She is clearly an exceptional analysist.”
That was special! Without a family connection I wonder how many people would display that kind of commitment.
They’ve done this work on a shoestring and while I’m very happy that DecodeME has been able to gather the funds I sincerely hope that Liz and Camille can get the funds to do the wholeshebang – get the sequencing done, analyse it, and test the results.
I also wondering if this is similar to the follow on from DECODE – Sequence ME and Long Covid, at Edinburgh university ? just in first stages, but it sounds like the same kind of analysis and on the 15,000 or more samples used for Decode. I may have misunderstood and not able read all details, but if it is same kind of thing, I wonder if they can collaborate, it always seems made when disparate researchers are doing similar things on tiny budgets get funding to scale up. Large scale is essential to get mainstream recognition.
Sorry mistakes in my above comment- I meant seems mad if researchers are doing similar things with tiny budgets , then can’t get funding to scale up – better if they can collaborate
Yes it is likely to be the same type of study. I discussed this approach with some of the folks in that team – unfortunately just as I was getting sick back in 2021/2022 and have reached out to discuss again just a few weeks ago. Hoping to do just as you say and collaborate to make sure we all work together on building lots of steps to our goal and not all just building the same first step :).
Thank you Liz!
I hope that some collaboration will happen! It is so interesting! Considering the common comorbidity of hEDS/HSD and the genetic studies in the “Road to 2026” by the Ehlers Danlos Society and by the Norris lab that could also be some possible collaboration.
I read today that one consideration for confirming fibronectin 52 kDa as a possible biomarker for hEDS/HSD was to see if that also appeared in ME/CFS and fibromyalgia. I think that fibronectin 52 kDa has to do with genetics too, but I might be wrong.
There is a study by the Norris lab on klk15 gene and hEDS.
I know that ME/CFS and hEDS/HSD are common coexisting syndromes with overlapping symtoms. As well as fibromyalgia and hEDS/HSD are. And hEDS/HSD and fibromyalgia. And as EDS Society and others now are exploring genetics on a larger scale, maybe…. … maybe there could be some useful collaboration?
Sequencing kit winging its way to me in the south pacific now….
Hope it is ok to respond here Cort! Thank you for the opportunity to share our work.
Thank you so much for these comments; we really are on a mission. It’s been a long path! Please do reach out if you would like to discuss the project.
I should also have mentioned the other folks roles in the interview. Though Camille and I divided up the majority of the small variant analysis and interpretation, we had a whole team working with us to make that possible. Brandon Wilk and Mana Gajapathy developed the methods and pipelines we used to perform the genomic analysis and Brandon set up the systems we use for tracking analysis whilst Mana performed all of the larger variant analysis, including finding one of the variants of great interest in one case. Donna Brown, Jarred Younger, Kathleen Hodgin, and Alp Turgut did all the work on patient intake and sample collection for sequencing. Without Jarred we would not have had this cohort to work on as he was the one that put it together! Shaurita Hutchins for all the expression analysis work that gave us clues in one of the cases, and Gurpreet Kaur and Tarun Mamidi for assistance with methods and case review.
If we didn’t have all these wonderful people in the group we would not have been able to do this work. Should have mentioned that. Sorry folks!
Thanks Liz. Your work is so impressive and it’s great that you acknowledge all those who have helped.
Excellent article, Cort, on an amazing paper. This does sound like a promising breakthrough. It gels well with my family experience. My father’s mother became ill in her twenties after a pregnancy and spent the rest of her life bed-bound. Her trigger may have been pregnancy or her severe diabetes? My brother had a Borrelia infection in his forties and has been bedbound unable to work since.
I had a Borrelia infection in my 50s and, although cured of Borrelia, have had mod/severe ME since. I would like to investigate any possible pathogenic recessive genes. Will order through sequencing.com and give the results to Liz and Camille
I am interested in the ‘so what?’. The theory is all great and nice, but how can this help us get better?
So I will ask again, Cort. You did the tests, you got the results – then what? Have the results informed potential approaches that might help your condition?
This email addresses two subjects. 1) Why does no one have a problem with Covid causing Covid and Long Covid, but they think that a single virus can’t cause ME/CFS?
Of course, affected people have different symptoms. As the former head of NIEHS said “genetics loads the gun and environment (in this case maybe a virus) pulls the trigger”. A person’s genetics will determine the symptoms they have although a similar trigger may create overlapping conditions.
2) Back to Covid. I have had Long Covid with heart and blood pressure involvement since 2023. I thought these problems were resolved until I passed out in October. My cardiologist, a very smart man, ran an EKG, ECHO and 7-day Halter monitor. My heart was physically fine but the electrical system had gone haywire. In 7 days, my heart ran up to 200 bpm 28 times. This didn’t correlate with any particular activity. I am now on a beta-blocker (these have been useful in Long Covid patients) and I will see another cardiologist who specializes in electrophysiology later this month. Other than passing out, I never noticed any symptoms. These problems have been reported in other Long Covid patients, but not all. Long Covid should be your roadmap into investigating the cause of ME/CFS, not trying to find myriad things that could cause it. By roadmap, I mean a known cause with different outcomes in different patients.
We have patients with Long COVID as the trigger and others with other types of infections or stressors; pregnancy, accidents, others. We absolutely take this info into account. Not everyone who gets covid ends up with these symptoms; that is where we feel and see the other genetic risk elements coming into effect. Happy to chat more if helpful.
I wonder in light of this research, and indeed DeCODE also, what the near future holds for the classification of ME/CFS, and also for its own specific naming.
Having thankfully wrestled it out of the clutches of Sir S and his fellow “Mad Men” in the UK, who had re-classified it as a psychological illness, the WHO still has our illness sitting safely under the umbrella of Neurological Conditions.
Would it potentially become classified as a Genetic Disorder perhaps?
I did get my dna done at 23&me, but got it deleted due to being notified it was hacked. Still scared about that since they went thru my family tree. Studies…are they doing one on our neighborhood right now as we speak? I have extremely sensitive hearing. We have a security system on our house. No one ever complained, since so, so many ppl have ring doorbell and like setups all over now. Hubby upgraded the system since it was over 10 years old and we have felt what it is like when there it multi-bullying. That was around October, I cancelled doc appt and never left the house since!! We did nothing wrong!!!! The next door neighbor would bring someone over and then this awful sound would occur. My hubby could hear it especially when it was loud, and one cat would run and hid under something and the other (who was old and has passed away from a supposed rare thyroid storm in Jan 2026) would throw up multiple times when this high frequency noise would occur.
Appears I can hear when they are searching for our electronics…. not going to go into what I hear, but it is horrible. Not sure if it is jammers or what. Our water meters are digital wireless as well as our electric meters. They are doing something around here with that horrendous sound and when you look out of your cameras, the whole street looks like it has an opaque wall, the cars drive thru it and almost become invisible, if you have it set on black & white. Not sure if they are using the water meter WIFI or what, but enough is enough. Every time that sound made the one cat throw up she looked like her face was contorting and she would just cry and cry.
The people don’t care what it is doing to us. If this is a study experment, shame on them for not getting our permission to torture us or our animals. If this is just some neighbor mad at everyone for having security of some kind, they need to stop what they are doing. Early on with minor issue, we did call it in, but I guess they just laughed it off.
So now, I don’t trust a sole. I won’t move either. This is our home. Being in our 60’s starting over is not an option, and having chronic mono, ehlers-Danlos, serious eczema (or is it reaction from the serious EMF interference around here), and being flooded twice, once in 2022 and again 2024, we have to stay. I seriously couldn’t even consider a study since they keep us in constant anxiety mode. My family tree is old and huge too. We’re talking, my family worked for William Penn, got married and came over with him to America family tree.
Wishing someone would stop this crazy stuff happening. We’ve had intereference before, from the previous owners, hoping it’s not the sattelite dish on the roof 15-20 feet away from us and the new owners have upped the high frequency level. Sometimes it would make me get so dizzy or swooney, it did make me fall three times and ended up with de quervains. Had to get shot and worst pain ever, but doc got it in one shot. cortisone has never helped me before, so not sure what he did. Yea for that, but he was also treating me with meds for conditions I do not have and the last med, almost sent me to the ER, my heart rate plummeted just mere minutes after taking it. I’m afraid to go back.
Does anyone else have these issues in their neighborhoods? I can’t believe we’re the only ones going thru this. Doc said he had to get my immune system calmed down. How can that ever happen if these people don’t stop the sound torture????
One of the electronic sounds, it’s a hissing variable high frequency sound, ultransonic, sometimes we hear low tones. Mostly high ones. How on earth do you get these people to stop this? We don’t know if there are Mosquito Boxes that run ppl off on the light poles or not, I read they have a couple of frequencies, or it they’ve been hacked.
You go outside and you can’t see any of that stuff, the opaque privacy wall shield, only on the cameras. I complained to my doc about the high frequency sound and months later, going to one of my appts., in the parking lot they had one of those parking lot poles with that Mosquito Box and the sound was horrendous. It was a seriously hard appt to sit thru. I told him about the sound. That was the one and only time that was in the parking lot. They have it at alot of stores now. How do sensitive hearing people navigate these days? Are we such a small number now or are there many of us? Any guidance on a resolve????
Thanks for listening….
I wonder if there is a tool to analyze data from Whole Genome Sequencing with mtDNA, in order to find the alleles that have been linked to ME in scientific studies.
The process we use does include looking at all of the body of literature to see if the variants that show up have been published previously. Or submitted to various clinical and research databases. Including for mitochondrial variants. There are a few of these tools on the market these days. My lab developed the very first ones – for clinical use back in 2008 :).
I sit on my data after a Whole Genome Sequencing with mtDNA, but I have never managed to figure out to how to check what variants/alleles I have for a specific gene. I have a 54 GB BAM file and I guess that some tool should be able to process the data and find out what allele I have of a specific gene. Any advice how I could do that would be appreciated.
Hi Karl. Yes there are tools to compare the data you have versus the human reference data and then tools to identify differences between them; this would be your set of “variants”. And then there are other tools to “annotate” the variants with all the info that is needed to try to determine whether any of the variants are or might be associated with your disease. For the latter part a human expert is involved to work through all the variants of interest to be able to identify the ones most likely to be of interest. Hope that makes sense. Feel free to drop me a note if you have other questions: eaworthey@uabmc.edu.!
Hello,
Have any of you tried the supplement Oxaloacetate? If so, has it benefited you, and how much did/do you take daily?
Thanks so much.
Im willing to bet my bottom dollar that every single one of us has crunching neck vertibrea when we turn our head from side to side?
Indeed, i have that too. Cort, can we create a poll to see if it is common among ME patients, Cort?
Yes, I did. For once I am one of the high responders. Even at 1x 100mg a day (the Benagene version of 100 mg oxaloacetate plus 100 mg vitamine C per cap) I noticed a small but clear improvement. So I guess I would respond quite well on 2x 1g or 2x 2g a day but I simply can’t afford that.
I slowly (my standard procedure for anything I try) build up to 3x 100mg a day and the main benefit is a bit more energy but clearly recovering a lot quicker from any exertion. So the max energy only increased a bit, but the recovery rate from any dip improved a lot. With that, the worst days became a lot less in number and less deep. So mainly symptom related discomfort improved.
I plan to further up dose later (money and trying out different thing now…).
No side effects from the added vitamin C yet (lose stool is possible with some people).
Dejurgen,
Thank you SO much for taking the time to reply in detail. I’m going to order it and get started right away! I could really get going here with a long reply, but this isn’t the platform for that.
If there’s something else you try that you find helpful, I would love to know. I understand about the financial cost of all this too….
Thank you again!
With Kindness,
Ann
Dejurgen,
I just ordered some! Thank you so much for your response! 🙂
With Kindness,
Ann
This is something I have been trialing also. I think the comments about getting just the right dose are key. Would be very interested in others experiences here.
I’ve just begun taking 100 mg daily of Benagene. After 7 days, I will increase to 200mg. I’ll see where I’m at after a month to determine if I will increase to 300 mg daily. I’ll keep you posted and would very much love to hear about your experiences.
Thank you, Liz!
Your email won’t show up on this platform, so I’m not sure how to exchange emails…
It is on our web page; you can search for “worthey” and “uab” and you should be able to find me 🙂
Woah, Cort, was Elizabeth saying at 1:32:00 that if the child in your womb was carrying the same recessive deleterious gene as you it could trigger your illness? Am I understanding that correctly? I had always assumed that pregnancy wasn’t the trigger because I had no problems after my first but after the second birth I was very unwell by the time he was 12 months old. Would that also mean it’s possible that he could be the one out of my two kids who could end up also becoming unwell? If I am not misunderstanding her comment, that is mind blowing.
I did my genome via 23andme ages ago; followed by using StrateGene to map SNPs to chemical cycles. It shows several clear patterns: slow ATP production and folate bottleneck, causing shortage of energy; and slow toxin clearance (multiple reinforcing SNPs on each pathway). The slow toxin clearance maps directly to my PEM (which takes 3-4 days to clear).
To Matthias’ “so what?” — It’s this kind of understanding that leads to diagnostics and identifying possible solutions. E.g.: I’m now able to directly target my problematic pathways with supplements to support them; and to predict/adjust/schedule activity, dramatically lowering the frequency and impact of crashes (when I follow it, which I don’t always, but now with fairly predictable results).
Prior to taking this approach, either my doctors or I were throwing spaghetti on the wall – “random study S (or random person P) said XYZ helped, let’s try that!” — with also predictable results (occasionally something helped a bit, too often, it didn’t).
Personally I suspect that the “avatars” mentioned in this study will likely map to different causes, and thus needing different fixes. Which may be medicines in the form of pills – or may not.