


Geoff’s Translation
The GIST
“With this breakthrough, we are proud to enable a first-in-class test that can address an unmet need for a quick and reliable diagnostic for a complex, challenging-to-identify illness,” said Oxford Biodynamics’ Chief Scientific Officer Alexandre Akoulitchev.
We live in creative times. The number of clever ways researchers can identify and diagnose disease states appears to be growing exponentially. Back in the day we had cytokines, antibodies, and MRIs. It used to be so simple. Now we have “3-dimensional genomic regulatory immuno-genetic profiling”!
Epigenetic changes that occur during infections can turn off “good genes” and turn on “bad genes”. An epigenetic shift makes perfect sense in ME/CFS and other post-infectious diseases, but until now the evidence has not been convincing.
This new technology takes a deep stab at an area of interest for all post-infectious diseases – epigenetics. Epigenetics refers to the changes in gene expression that occur as we encounter pathogens or other stressors. We adapt to these stressors by turning on or off parts of our genomes. Genes that didn’t used to fire strongly now do so. Genes that were firing strongly die down. Given that many people with these diseases can date the start of their illness to an infection, it only stands to reason that an epigenetic shift – and not a good one – may have occurred.
Epigenetic studies, however, have not exactly lit up the ME/CFS world. This one, by using a different technique, has.
This new study, “Development and validation of blood-based diagnostic biomarkers for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) using EpiSwitch® 3-dimensional genomic regulatory immuno-genetic profiling“, though, takes epigenetic analyses one step deeper.
In the paper, the authors focus nicely on three main factors in ME/CFS: immune dysregulation; dysregulation in the expression of genes involved in the immune response, energy metabolism, neurotransmission; and problems with energy production and metabolism (i.e., energy production).
Then they go to the nub of the problem – identifying these problems has not produced much help, clinically; i.e., while the scientific findings are generally cohering, they have not helped ME/CFS patients at the doctor’s office.
Why? Because ME/CFS is quite heterogeneous, the findings have not always been reproducible, and the studies have generally been small. None of this is news, of course. The question is why Oxford Biodynamics thinks they can help out.
THE GIST
-

EpiSwitch® charts how the folds in our chromosomes that occur as a result of epigenetics changes which genes can interact with each other.
We live in creative times. The number of clever ways researchers can identify and diagnose disease states appears to be growing exponentially. Take the latest study employing “3-dimensional genomic regulatory immuno-genetic profiling”!
- This new technology takes a deep stab at an area of interest for all post-infectious diseases – epigenetics. Because pigenetics refers to the changes in gene expression that occur as we encounter pathogens or other stressors, epigenetic changes could play a huge role in ME/CFS. Thus far, though, epigenetic studies have had less than enticing results. This study, which received widespread media attention, is different.
- This study attempted to get at epigenetic changes in ME/CFS through the back door, so to speak. The chromosomes, which hold our genes, change the way they are folded when confronted with pathogens or other stressors. They do this to bring genes that are not normally near each other close together, allowing them to interact. These new interactions are called “loops”.
- Usually, these loops produce a boosted immune defense, but sometimes the chromosomes become folded in such a way as to promote adverse effects.
- This new study from Oxford Biodynamics used specialized technology to assess the loops in housebound ME/CFS patients vs healthy controls.
- The results were startling. Their ability to accurately (96%) identify which people had ME/CFS and which people were the healthy controls was remarkable. The fact that they did this using 200 genomic biomarkers suggested that their findings had a strong foundation.
- Using pathway analyses, they identified three main immune issues in ME/CFS: an IL-2 network hub, innate immune activation, and JAK-STAT signaling. All could conceivably make sense with ME/CFS as we know it today.
- The authors identified approximately a dozen drugs that, if the IL-2 finding is replicated, could be applied to patients with high IL-2 levels. Plus, at least 3 JAK/STAT-inhibiting drugs are being trialed in ME/CFS.
- Encouragingly, the authors also noted that the inflammatory pathways found in ME/CFS are similar to those found in better-studied and treated diseases such as multiple sclerosis and rheumatoid arthritis. Validating that could conceivably open the door to dozens of immune drugs that have never been trialed in this disease.
- Considerations regarding this proof-of-concept study include its small size, its focus on only one slice of ME/CFS (housebound patients), and the use of a specialized procedure that may not be easily or cheaply replicable in other labs. Additionally, larger studies involving more diseases are needed.
- That last point appears to be the sticking point in ME/CFS diagnosis. Creative attempts to accurately diagnose ME/CFS are popping up more and more. What the field lacks are the larger, follow-up studies that could validate them.
- The small 2019 nanoneedle produced the most stunningly accurate results yet (100% accuracy) but failed to get further funding. Recently, though, ME Research UK and the ME Association have begun funding more nanoneedle work.
- The single-cell Raman microspectroscopy + AI study stood out with its high accuracy rate 91%, its inclusion of both multiple sclerosis patients and healthy controls, and its remarkable ability to accurately distinguish between mild, moderate, and severe ME/CFS cases. The Open Medicine Foundation and ME Association are funding more work into Raman spectroscopy.
- Some metabolomic and proteomic studies have also achieved high accuracy rates.
- As noted earlier, though, what this field lacks is the next step: large, comprehensive trials that contain both healthy controls and several different disease states. Hopefully, Oxford Biodynamics and/or the nanoneedle group and/or the Raman spectroscopy group, or another group, can get their diagnostic work across the finish line, and we will finally have a biological diagnostic marker for ME/CFS.
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit
Looking for Loops
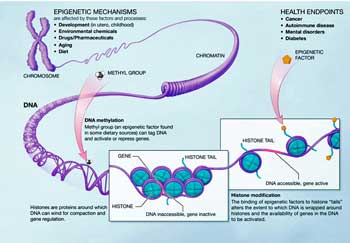
Epigenetics occurs when parts of the genome which regulate gene expression (promoters, enhancers, insulators) get turned on. Because these epigenetic changes can get passed down during cell division, the changes can be more or less permanent (until the next epigenetic change occurs).
It turns out that the chromosomes in which our genes occur are amazingly flexible. When faced with an infection, the chromosomes in our immune cells, for instance, fold themselves in such a way as to turn on certain genes. They do this by folding themselves to bring genes which are ordinarily distant from each other, close together. When this happens, a “loop” is formed.
These loops bring regulator genes (promoters, enhancers, etc.) next to active genes in order to turn them on or off. Most of the time, this is helpful, but viruses and inflammation can hijack this process and turn on genes that produce inflammation and immune activation.
The EpiSwitch® technology, developed by Oxford BioDynamics, basically identifies genes that, by virtue of the unique folding patterns found, have become able to talk to each other in diseases. Once they uncover these loops, they look for genes within a specific distance that these loops may be turning on or off; i.e., they’re identifying disease-specific epigenetic wiring patterns.
Using EpiSwitch® technology, Oxford Biodynamics has identified epigenetic signatures for amyotrophic lateral sclerosis, rheumatoid arthritis, and urothelial cancer. The authors reported that EpiSwitch®-based commercial tests are now available to diagnose prostate cancer with 94% accuracy (PSE test) (!) and the response to immune checkpoint inhibitors across 14 cancers with 85% accuracy (CiRT test).
EpiSwitch charts how the folds in our chromosomes, resulting from epigenetic changes, determine which genes can interact with each other.
The authors reported that Oxford BioDynamics has also produced a blood-based test that can predict COVID-19 severity, and have uncovered genomic markers that identify potential treatments for the biological pathways associated with them.
In this proof-of-concept study, they tested their procedure on an even bigger challenge – ME/CFS. The study included 47 people with severe ME/CFS, and 61 age-matched healthy controls. The goal was to see if the chromosomes in ME/CFS had become folded in a way that turned on pathogenic gene combinations that produced or contributed to ME/CFS.
Oxford Biodynamics used a more rigorous approach in this study compared to their past disease studies. Because we didn’t know as much about ME/CFS, instead of targeting their analysis on specific loops, they searched through the entire genome of the ME/CFS patients. Because of this, they were more apt to uncover more novel “loops”, or DNA folding patterns.
The Study
The study assessed chromosome folding patterns in 47 patients with severe ME/CFS (housebound) and n = 61 age-matched healthy controls.
This study found a significant amount of aberrant chromosome folding has occurred in ME/CFS. Using 200 genomic biomarkers, the researchers were able to identify ME/CFS patients with a sensitivity of 92% (correctly identify 92/100), and specificity of 98% (identified virtually everyone who was healthy as healthy), had an overall accuracy of 96% (when putting ME/CFS and healthy controls together, it was accurate 96% of the time).
Right now, the Epswich test is one of the most accurate diagnostic tests ever reported for ME/CFS, and has received plenty of coverage in the media.
The fact that the study used approximately 200 broad-based biomarkers suggested: a) ME/CFS is polygenic; i.e. many genes contribute to it; and b) the results rested on a broad biological foundation. The accuracy also suggests that, for all the discussions of subsets in ME/CFS, core biological features involving the immune system, in particular, persist throughout ME/CFS. Once again, (how many times does this need to happen?) the idea that ME/CFS is some sort of wastebasket disease was demolished.
A pathway analysis found that the top 200 genomic markers existed within a densely connected immune network strongly enriched for (biased towards) immune and inflammatory signaling and cellular stress responses. Both the idea of inflammation and stressed-out cells, of course, makes sense in ME/CFS.
Update! Check out a January, 2025 Solve ME webinar
IL-2 Stands Out
One cytokine – called IL-2 – appeared to play a key role.
Within that network, several hubs appeared. The top hub focused on the IL-2 cytokine, which appeared to influence several other immune nodes. IL-10 and other interleukins also showed up strongly, as did T-cell regulation – another immune cell which has shown up recently (aka T-cell exhaustion) in ME/CFS.
IL-2 was the major focus, though. The authors reported that IL-2 can cross the blood-brain barrier, and, by influencing microglial activity, result in central sensitization and cognitive symptoms, and neuroinflammation. Interesting animal studies suggest that IL-2 administration can produce fatigue-like behaviours and cognitive problems.
IL-2 levels have been variable in ME/CFS, but as we’ve seen, the level of a cytokine is less important than the role the cytokine plays in the immune networks. One study suggested that in the lab, IL-2 can restore NK cell functioning in ME/CFS cells. Low levels of the soluble IL-2 receptor were also associated with a poor response to IVIG in ME/CFS.
IL-2 plays a key role in the survival and expansion of T-regulatory (Treg) cells. Levels of these cells, which rein in the immune response, tend to be high in ME/CFS, presumably because they’re trying to tamp down an overactive (and exhausted) immune system.
Low-dose IL-2 is used in several autoimmune/inflammatory diseases to boost T-regulatory cells and get autoimmune/inflammatory processes under control. The authors focused more, though, on dampening IL-2 levels in ME/CFS patients to stop chronic T-cell activation, and ultimately, the T-cell exhaustion.
Innate Immune System Activated – Several hubs (TNF / NF-κB axis, Toll-like receptor signaling) were associated with activation of the innate immune system, which increasingly appears to be a prominent feature of ME/CFS. Nath and others have proposed that problems in the adaptive, later-acting immune system may be causing the early, more inflammatory innate immune system to become hyperactivated.
JAK/STAT Pathways Highlighted – Finding evidence of activated JAK/STAT immune pathways was a welcome sign in many ways. For one, JAK/STAT pathway plays a fundamental role in a wide range of diseases including autoimmune and inflammatory diseases. It’s getting a lot of study, drugs are available, and one (Baricitinib) is being trialed in long COVID.
Problems in the JAK/STAT signaling pathway increase the expression of inflammatory genes in several diseases.
The JAK/STAT pathway translates signals from cytokines that land on the outside of the cell into gene expression in the cells. Aberrant JAK/STAT functioning chronically activates immune cells, leading to inflammation and damage. JAK/STAT inhibitors calm this pathway down, taking immune cells off the ledge. If ongoing immune activation is exhausting T, NK, and other immune cells, JAK/STAT inhibitors could help return the system to normal.
The pathway map suggests, if I understand the authors’ report, that altered cytokine signaling produces innate immune hypersensitivity. That, plus a pathogenic JAK/STAT transcriptional program that promotes immune activation and inflammation, could be producing the fatigue, cognitive symptoms, and autonomic dysfunction described in ME/CFS. It’s a nice model!
ME/CFS Not Alone?
In what can only be good news, the authors reported that similar immune pathways have been found in multiple sclerosis, rheumatoid arthritis, and other chronic inflammatory disorders. They stated that the “epigenetic alterations” found in ME/CFS aligned “closely with known pathways involved in chronic inflammation and immune dysregulation”.
That’s good news for anyone looking for sooner-rather-than-later treatment options. The best outcome would be for the immune and other findings in ME/CFS to line up closely enough with other disorders that the treatments which work in those disorders could be tried. These are the kinds of findings, which, if validated, promise to bring ME/CFS “out from the cold”, and into the broad mainstream of disease.
This is why it’s so darn important to identify the molecular pathways at work in ME/CFS. Lots of studies do identify molecular pathways and we are seeing overlaps, but we still apparently don’t have the consensus needed to launch major drug trials that attempt to alter them.
It would seem that we’re at or near the place where patients with alterations in specific molecular pathways could be identified and treated, but we haven’t seen those kinds of personalized studies yet.
Possible IL-2 Treatment Regimen
If the authors of this paper are right, the path could be much simpler: identify the subset of ME/CFS patients with high IL-2 levels and try them on IL-2-reducing drugs.
The authors identified at least 12 drugs that can reduce IL-2-producing CD4+ cells while increasing IL-10 levels. (Il-10 tamps down immune activation). The fact that numerous drugs exist indicates how rich a space this could be for ME/CFS if the IL-2 connection is validated.
The drugs included Rituximab, Copaxone, Rapamycin, Tacrolimus, mycophenolate mofetil, azathioprine, low-dose methotrexate, corticosteroids, dimethyl fumarate, hydroxychloroquine and Vitamin D3 (Calcitriol).
Although the large Rituximab ME/CFS trial failed, some participants showed results, raising the question of whether the maintenance dose was sufficiently high. A Japanese study underway will help to answer that question. The Rituximab study was not targeted in the same way as a study focused on patients with high IL-2 levels.
The idea that epigenetic modifications could be driving ME/CFS makes perfect sense. With their new technology, Oxford Biodynamics appears to be making good on that notion. We can’t celebrate yet, though. Much work remains to be done before we can say we finally have a diagnostic test for this disease.

Oxford Biodynamics is off to a good start, but many questions remain to be answered before the Epswich test can be considered a diagnostic test for ME/CFS.
Considerations
- The best diagnostic biomarker would be cheap and readily available. Because chromosome folding assessments require specialized labs, one question is whether this tool could ever be widely used as a diagnostic measure. Chris Ponting believes this test would probably cost over $1,000. One of the significant advantages of the nanoneedle was that it offered the potential for a cost-effective test that could be easily conducted in a doctor’s office.
- Because all the ME/CFS patients were severe, i.e., housebound, these findings might not reflect those in less ill patients. Chris Ponting pointed out that because gender can make a big difference, genders need to be assessed separately. Activity levels need to be addressed as well; i.e., the comparative group needs to be sedentary. Age needs to be matched more closely.
- This was a proof-of-concept study. It certainly worked, but as the authors (and others) have noted, bigger and more comprehensive studies need to be done, including assessing the test against similar but different disease groups.
- We have several potential diagnostic tests, and more will surely be forthcoming. Finding a potential diagnostic test is becoming increasingly easier. It’s the next step – validating it – and then getting it into a doctor’s office – that has proved more challenging.
Diagnosing ME/CFS: Creativity Abounds; Persistence Not So Much
Researchers are investigating ever more ways to diagnose ME/CFS. The small 2019 nanoneedle produced the most stunningly accurate results yet (100% accuracy) but lacked external validation.
The single-cell Raman microspectroscopy + AI stood out with its high accuracy rate 91%, its inclusion of both multiple sclerosis patients and healthy controls, and its remarkable ability to accurately distinguish between mild, moderate, and severe ME/CFS cases.
The .95 (AUC) figure in Germain’s small 2021 plasma proteome study suggested that proteins may be able to cull out people with ME/CFS accurately.
Interestingly, some of the highest diagnostic accuracy rates have come from metabolomic studies. Naviaux’s small targeted plasma metabolomics (Naviaux et al., PNAS 2016) came up with an overall accuracy of .96 (AUC) for females and 0.94 (AUC) for males. Similarly, Nagy-Szakal’s 2018 metabolomics model had an accuracy rate of .960 (AUC) with ML (Nagy-Szakal et al., 2018).
The good news is that researchers appear to be getting better and better at finding ways to accurately diagnose ME/CFS. Plus, we’re seeing more and more new researchers entering the field. Their findings suggest that ME/CFS is not a wastebasket disease but that core abnormalities exist and can be found. That’s all good news for a disease that’s still struggling for validation and funding.

Possible diagnostic biomarkers exist. The next step is getting the studies together that can validate them.
Despite the creativity shown by ME/CFS researchers, the next steps to validate these diagnostic biomarkers using larger cohorts and more disease groups have not yet been taken; i.e., it all comes down to that perpetual problem – securing funding. The nanoneedle is a telling, if somewhat tragic, example. The NIH funded the creation of the needle, but then, after the needle proved effective at distinguishing ME/CFS patients, it failed to fund it further.
Thankfully, the ME Research UK and the ME Association are funding more nanoneedle work, and the Open Medicine Foundation and ME Association are funding more work into Raman spectroscopy. Hopefully, Oxford Biodynamics will be able to expand its ME/CFS findings.
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit


Interesting!
I found the comments on IL-2 especially interesting, as I was quite obsessed in the 1990s with some small Japanese research linking IL-2 and natural killer cell activity with ME/CFS. A researcher from Kyoto University was experimenting with a compound called sizofiran from a mushroom.
I think the researcher died and perhaps so did the research
As always, my central theory on the cause and the treatment target (s)
of CFS has evolved since last time I posted.
I take special note of Cort’s points that IL-2 cytokines are boosted in CFS and that the innate immune system is hyperactivated.
Starting from my theory that there is glutamate excitotoxicity occurring, producing a calcium level overage in cells (as part of hypoxia from poor blood perfusion),
I think back to Rob Phair’s Itaconate Shunt hypothesis of why so few ATP are available during exertion.
He stated that ATP can be produced, but then shunted away from use for exercise. He left us with the question: if this is indeed occurring, then WHY?
Working in the content in today’s blog, I have previously learned that ATP may be shunted for use in Cytokine production. Given that the Innate immune response relies on cytokines and anaerobic conditions to make infected cells hostile to microbes…
innate response can explain: raised IL-2 levels, shunted ATP, and an anaerobic state consistent with flu symptoms inclusive of fever.
I read a review stating that “CFS onset is triggered by an infection with EBV or other intracellular pathogens”, citing a 2008 paper.
https://www.sciencedirect.com/science/article/pii/S0889159115300209
As many of us know, Epstein-Barr Virus
can go dormant but remain with us.
“EBV establishes a permanent infection in human B cells. It uncommonly causes infectious mononucleosis”
Such an infection would be a likely cause of chronic innate immune response, therefore of fatigue and of PEM.
Another resident pathogen could be triggering the innate response, and in some patients the B-cells activated contain EBV,
The net effect is that the Krebs cycle fails, but this failure might be part of the immunity design to simultaneously require anaerobic metabolism, minimize ATP production, and nourish
the cytokine farm.
What causes incorrect blood pressure may also be what causes excitotoxicity: TRPM3-type ligand-gated ion channel failure.
My view is that the core problem is in the brain / CNS. That a chronic state of neuroinflammation is established by an initial insult, often but not always viral. I do not believe the illness is perpetuated by a virus, viruses or viral factors. Which is why I have held for a long time that trials of antivirals are a waste of time.
The neuroinflammation generates cytokines in the brain. One of them, Interleukin-6, has been shown to communicate with muscles in the periphery. This, in my opinion, is the cause of muscular fatigue and PEM.
The neuroinflammation negatively impacts on dopamine. And there is a feedback loop – low dopamne leads to more neuroinflammation which leads to low dopamine which leads to more neuroinflammation ….. The low dopamine, together with impacts on glutamate, adds to the fatigue from cytokines.
My view is that treatments that act on inflammation in the brain are the answer to this illness.
It’s good to see one or two being trialled.
I just looked up sizofiran. it is a beta d glucan.
Very interesting and potentially promising. I’d love to see how the accuracy holds up when looking at people with fibromyalgia or long COVID, does this test still distinguish ME/CFS because there’s so much overlap?
That would be quite a challenge! If I was doing this I think I would include FM and long COVID and then more distant diseases like MS and RA.
Thanks, Cort. As always, thorough and clear and the Gist is a godsend.
I remember the buzz around the nano-needle but I didn’t realize there were 2 other approaches that also showed massive promise.
I apologize if you answered this in the article, but what is the reason that such promising opportunities are not followed up on in private, public or international research?
The work on the nanoneedle collapsed when the inventor couldn’t get funding from the NIH. He had just moved to a faculty position at UC Irvine and needed to get funding to achieve tenure. I’m not sure what happened there at Irvine with him, but I know the NIH turned the application down.
Some ME/CFS groups have picked up the slack with the others. The nanoneedle is being pursued again. The thing about the nanoneedle that is so intriguing is that Ron Davis said a test would be cheap and easy to administer. I get the impression but don’t know for sure that Morten has received a good amount of funding to pursue the RAMAN finding. That finding seems really promising – and he’s already tested it against MS 🙂 If I remember correctly RAMAN spectroscopy is more expensive.
Thank you, Cort for highlighting this important news.
I hope the Max Delbrück Center in Berlin is also investigating demethylation, especially in light of recent advances demonstrating that gene-editing in patient-derived and humanized-mouse primary muscle stem cells can restore dysferlin expression in dysferlin-deficient muscular dystrophy.
Professor Simone Spuler and her team, led by Dr. Helena Escobar in the Myology Lab at the ECRC, have successfully isolated muscle stem cells from two patients with limb-girdle muscular dystrophy, corrected the genetic defect, and restored functional dysferlin protein in cell culture.
Max Delbrück Center in Berlin: https://www.mdc-berlin.de/news/press/developing-crispr-therapy-muscular-dystrophy
Nature paper: https://www.nature.com/articles/s41467-024-55086-0
“corrected the genetic defect” – amazing what’s possible now 🙂
I understand that CRISPR-Cas9 is only the beginning of what gene editing technology can achieve.
Jennifer Doudna has already demonstrated its potential by using CRISPR-Cas9 to treat sickle cell disease—editing a patient’s own blood stem cells to correct the underlying genetic mutation. https://www.youtube.com/watch?v=D4FOtJoqoKM
However, there remains one major obstacle for most individuals: the cost.
For example, I’ve learned that treating Dysferlinopathy—a rare, inherited form of muscular dystrophy caused by mutations in the DYSF gene, resulting in a deficiency of the dysferlin protein—currently costs around 2 million euros using gene editing technology.
Like I say, it is just the beginning.
Thanks. I can’t imagine but that the cost will come down – this technology has so much promise!
The Max Delbrück Center is the future of medicine—powered by exceptional scientists and innovative labs.
Each lab offers specialized platforms and collaborates in interdisciplinary teams to drive groundbreaking research.
https://www.mdc-berlin.de/research/discovery/labs-platforms
Thanks for the tip. It’s pretty clear that interdisciplinary is the way to go…
That is excellent news! Thanks!
So what happens if a definitive test for ME/CFS is confirmed?
Private insurance companies have to cover our care.
Medicare and Medicaid have to cover diagnostics, testing and treatment.
Long term disability has to be granted by private companies.
Social Security Disability must also be granted.
The focus for funding availability will change from the theoretical to definitive treatment options so a lot of labs will be out of the loop.
Friends, it is all about the money. A reliable test for ME/CFS would cost a lot of money…no one wants to pay.
Unfortunately, you are most likely right. 🙁
It’s not up to Medicare, Medicaid, Social Security or insurance companies though…It’s up to the researchers! Yes, they will have to decide whether to ignore it or accept it. In some ways a diagnostic test would be helpful – patients wouldn’t have to go through this long process – costing insurance companies, etc. a lot of money as they wind their way through the medical system.
Plus, if it led to more interest from Pharma – as I’m sure it would – it could result in fewer charges as better treatments are developed and FM patients don’t need to try everything under the sun.
The road to accurate diagnosis and effective treatment is finally being paved.
Health insurers now face a pivotal decision: continue funding costly, lifelong treatments for conditions like Type 1 diabetes, spinal muscular atrophy (SMA), leukemia, or other metabolic disorders—or invest in one-time genetic cures.
Platforms like 23andMe are equipped to identify “RS” genetic markers across the genome, enabling a new era of precision medicine. With the rise of CRISPR-Cas9 treatment centers, the traditional model of long-term hospital care is poised for disruption.
I’ve had my DNA sequenced and began comparing well-documented genetic markers with the genes highlighted in green in Fig. 3 of the following study. Furthermore, Fig. 4 illustrates the overlap between ME/CFS and other inflammatory conditions, revealing shared pathways involved in chronic inflammation and immune dysregulation. https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-025-07203-w
These insights suggest a possible genetic basis for a range of acquired illnesses.
This marks the beginning of a shift—challenging outdated approaches still relied upon by some medical professionals who prescribe treatments that may be ineffective or harmful. It also pushes back against the psychological dismissal of chronic illnesses as being “all in your head.”
Cort, I think you missed the point of my post.
You said…The work on the nanoneedle collapsed when the inventor couldn’t get funding from the NIH.
Why wouldn’t the NIH fund such an important study. The very reasons I listed.
I have 40 years of working with researchers and some are dedicated to the issue and the others to keeping their labs funded.
And no, researchers don’t hold the cards on government decisions on health care.
Over 90 researchers have warned that acetaminophen can be linked to neurodevelopmental problems like autism and attention disorders when mothers take the drug during pregnancy. There are now 29 peer-reviewed published studies confirming this association.
We first presented this possibility at a national autism conference in Chicago in 2009 and put it out on the PR wire that goes all over the internet.
Finally, the FDA is requiring pregnancy warnings on all products containing acetaminophen an sending out a Dear Doctor letter with the warning as well.
This took 16 years and some very dedicated scientists who managed to find funding on a very controversial issue.
If they could do it, why haven’t ME/CFS researchers been able to do better in the 40 years I have had it.
Interesting.
Short version:
Caffeine has quite a strong impact on both IL-2 and IL-10. Caffeine also increases acetylcholine release, affecting both the nervous system (parasympathetic versus sympathetic) and immune functionning. The many ME/CFS patients who do well on weak coffee may well be self-medicating with it.
IMPORTANT NOTE: caffeine does have significant side effects, more does not simply mean better.
Long version:
Two weeks ago user Baz493 posted a connection between over-exertion, extracellular ATP and mast cell activation on https://www.healthrising.org/forums/threads/oxidative-stress-induced-histamine-release-and-fatigue.6965/
I can relate to over exertion causing MCAS like symptoms and ME/CVS cells are observed to dump some ATP when over-exhausted. I think Ron Davis had a post on cells doing that.
Now some search showed that this P2X7 receptor (that responds to excess extracellular ATP with giving us things like immune activation) can be blocked by an oxidized form of ATP called oxATP: https://onlinelibrary.wiley.com/doi/10.1002/eji.200939838
The interesting thing is: oxATP has a very strong effect on IL-2 (and IFN-gamma) (see Fig2) and with it some potent effects on parts of the immune system. (Note: simply more or less IL2 is NOT the answer, it requires a complex equilibrium with things like soluble IL2 receptors). The functioning of P2X7 is closely linked to adenosine receptors (AR). And caffeine is an A1 receptor (subtype of adenosine receptor) antagonist.
This leads me to https://www.sciencedirect.com/science/article/abs/pii/S152166161830216X saying: “Cytokine levels of IL-8, MIP-1β, IL-6, IFN-γ, GM-CSF, TNF, IL-2, IL-4, MCP-1, and IL-10 were decreased significantly with caffeine treatment.”
It also strongly reduces macrophage reaction against the strong innate immune activator LPS: https://pmc.ncbi.nlm.nih.gov/articles/PMC8308523/
Caffeine is so interesting because when it works it can just erase my symptoms. When I use it too much or when I’m too weak to handle it, it just makes things worse. When it works though it really works and I only need a little of it. 🙂
I’m so grateful that caffeine works for you, Cort. Anything that helps you live a quality life is great news. Thanks for all you do here and all the support you give us all. And for all the years you have been out there picking up the research and handing it on to us.
Thanks! It can be a bit of a double-edged sword but when it works its great 🙂
Good news on the nano-needle front! Hopefully more private money will keep things moving slowly ahead!
It’s mind blowing to me that Oxford Biodynamics stock went up 33% on the day of the Episwitch for ME/CFS announcement.
There are 18 ME/CFS diagnostic blood tests in various stages of development, and not a single mention of them has been mentioned in the media to explain the ME/CFS biomarker field to investors.
The Nanoneedle technology was able to identify every single ME/CFS patient in its pilot study. The technology can take 200 measurements can second. I think it’s inaccurate to say “The Nanoneedle is back” in reference to Clarke et al. In the U.S. the electrophysiological properties of white cells in ME/CFS patients was measured with the Nanoneedle, in the UK, it’s being measured by a technology called the 3DEP. We have no way of knowing how comparable the 3DEP and the Nanoneedle are.
The fact is that the Nanoneedle technology is/was amazing. North American Advocates should have gone against the NIH for the Nanoneedle to be funded. In 2020, when we all heard what the NIH did to Dr. Ron W Davis and Dr. Rahim Esfandyarpour – WE – should have supported our researchers and the Nanoneedle technology by going to the mattresses for them. We should have turned over the tables at the NIH to support them, and someday it will be our shame that we chose to do nothing instead.
Right now, Open Medicine Foundation is back with the largest ME/CFS Biomarker study and ready to leap the world ME/CFS diagnostic blood tests forward with OMF BioQuest – and we need all hands on deck to fund and support it. The Irish ME/CFS Association has donated to OMF BioQuest and now we need ME Action, ME Association, ME Research UK, Invest In ME, World Alliance for ME, to step up and do the same.
The Nanoneedle was designed by Esfandyarpour et al to measure Proteins in the blood. OMF BioQuest is going to measure 10,000 Proteins, along with metabolites, lipids, and cytokines. Proteins can be easily turned into commercial blood tests. The recent FDA-approved Alzheimer’s blood test is 2 Proteins, beta amyloid and tau. Recently, a new study has found a. panel of 33 proteins in ALS patients. The Michael J Fox Foundation has found two proteins for Parkinson’s disease alpha-synuclein and LRRK2.
If BioQuest finds a protein panel for ME/CFS, we are going to be catapulted onto this august list.
The time is now to stand in solidarity with Open Medicine Foundation to support BioQuest. Every ME/CFS and M.E. Organization needs to sign on, promote, and fund OMF BioQuest.
I think in ME/CFS we are far too hung up on the fact that our disease is heterogeneous.
ALS is also heterogeneous, with multiple triggers, and that is not a barrier to having a multi-disciplinary medical team, a treatment plan, FDA-approved drugs, or a thorough diagnostic biomarker search to help make ALS diagnosis faster. In ALS they say, “Every patient is their own control”, and we as ME/CFS patients need to send that same message about ME/CFS. Because it’s ok. They found a 33 proteins panel for ALS.
There is a huge possibility that OMF BioQuest will do the same for ME/CFS.
So please support BioQuest.
Thanks Cort, this is amazing! With regard to diagnostic tests out there, I think https://www.healthbioai.com/our-science (Dr. Bruce Patterson et al) are essentially claiming they can categorize/identify people with various invisible illnesses from Long COVID to ME/CFS to chronic Lyme using their Cytokine 14 test.
I am not saying this study is not onto something, but at the same time some caution really has to be taken into account.
It is not a large study, but more importantly… who has actually been studied??
The study says they researched ME/CFS patient. This would mean a mixed population of both fatigue-based (CFS) and neuro-immune based (ME) patients. This would also imply the use of either CCC or NICE criteria. However the criteria they use are not only not referenced, they also do not conform with any known ME/CFS criteria (why not?). When you look a bit further down in the article, at the patient inclusion criteria, they suddenly only talk about CFS and no longer ME/CFS. Again, why?!
So who has actually been studied (and potentially will benefit from the findings)?
CFS, being fatigue-based patients.
ME/CFS, being a mix of neuro-immune based and fatigue-based patients.
Or ME, being neuro-immune patients (ICC criteria).
@Kristien fully agree I am very weary of this study as definitions are vague and only CFS is considered with no mention to PEM… I find this shady asf, and worry the NHS psych lobby may very well be behind it.
This epigenetic test really makes sense, considering the findings of Al and Kathy Light at the University of Utah, with their first journal article published in 2009. (Covered on Health Rising in 2017.) Their studies documented epigenetic changes for sensory, adrenergic and immune genes in me/cfs patients after 2 consecutive cardiopulmonary exercise tests. Their studies distinguished pwmes not only from control subhects but also from people with fibromyalgia only or an unrelated fatiguing illness (multiple sclerosis).
I just hope this test can hit the market soon, to help the many people searching for a diagnosis. Primary care providers are reluctant to even think about me/cfs without diagnostic tests. At least a test result may encourage them to try off-label meds with patients who test positive.
I first read about this in the UK news about 2 weeks ago and the let’s wait and see comments from long time ME doctors. I was surprised the research had been done at East Anglia university – a small UK university. I did my own research about Prof Pshezhetskiy the lead researcher at East Anglia University working with Oxford Biodynamics. A new name in ME research. A very ambitious and bright guy with a long track record and prizes for his work. I feel really positive that medical researchers like this are now taking an interest in ME.
https://research-portal.uea.ac.uk/en/persons/dmitry-pshezhetskiy