


Geoff’s Narrations
The GIST
This is the second blog to emanate from the 2025 IACFS/ME workshop. It covers Kunihisa Miwa’s presentation on disequilibrium in ME/CFS. Japanese researchers have consistently contributed interesting work on ME/CFS, and Kunihisa Miwa is a good example.
This is the second blog to emanate from the 2025 IACFS/ME Conference. More are coming.
Miwa, who runs a clinic in Japan, appears to be something of a lone wolf. He’s been publishing interesting, kind of off-the-beaten-path ME/CFS studies, authored by him and sometimes by others, since 2008. That year, he introduced the idea of “small heart syndrome” in ME/CFS and subsequently published four more studies on it.
If not for Miwa, we also wouldn’t know that the renin-aldosterone-angiotensin paradox – possibly a key problem – exists in ME/CFS. In 2020, Miwa introduced the idea that postural instability or disequilibrium was a more important cause of the orthostatic intolerance (symptoms caused by being upright) in ME/CFS than POTS. He also pioneered the use of repetitive transcranial magnetic stimulation in ME/CFS.

Miwa’s recent study, “Static and Kinetic Disequilibrium are Central Neural Signs in Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome-Therapeutic Effect of Repetitive Transcranial Magnetic Stimulation“, used the Romberg to test for static disequilibrium (standing) and the tandem gait test with turn and return to test for kinetic disequilibrium (walking). Again, he used rTMS in an attempt to alleviate symptoms.
The GIST
- This is the second of a series of blogs emanating from the 2025 IACFS/ME conference.
- Kunishi Miwa, a Japanese researcher, presented the intriguing idea that something called disequilibrium or postural instability (the inability to stand and walk without swaying) was contributing to orthostatic intolerance (inability to be upright without symptoms).
- His large study in his clinic found that 25% and 44% of ME/CFS patients, respectively, exhibited disequilibrium while standing or walking. Miwa used the Romberg test (see blog for how to do it) and a tandem walking test to assess his patients. He also used a 10-minute standing test.
- The fact that almost all of his patients with POTS were able to complete the standing test while almost all of his patients with disequilibrium were not able to, convinced him that disequilibrium plays a more important role in orthostatic intolerance than POTS.
- Other studies have documented (sometimes in smaller amounts) that disequilibrium is a part of ME/CFS, fibromyalgia, and long COVID for at least some patients.
- They have also found that disequilibrium contributes to fatigue due to the need for muscles to constantly try to balance the body, by the muscle bracing that is often seen, and the cognitive drain caused by the need to use the eyes to orient oneself in one’s physical environment.
- One ME/CFS study found that when asked to solve a simple math problem, many people with ME/CFS had to stop their walk to do so – a clear sign that they were already being cognitively stressed.
- Believing that neuroinflammation in the brain stem area was causing the disequilibrium, Miwa used minocycline and repetitive transcranial magnetic stimulation (rTMS) – both of which can tamp down neuroinflammation – to address the situation
- Both were successful. Both resulted in dramatic reductions in disequilibrium. In his presentation, Miwa reported on a patient who was unstable while standing or walking but became stable after rTMS.
- Note, though, that the study was not placebo-controlled, and because it involved recently ill patients, they might have improved on their own. Plus the dropout rate in one of Miwa’s minocycline studies was very high (44%). Still, the studies provide good preliminary evidence that could set the stage for larger trials.
- In conclusion, if Miwa is right and disequilibrium is contributing to problems with standing, then the treatment focus shifts a bit. While we know that reduced blood flows to the brain are contributing to the orthostatic intolerance in ME/CFS and long COVID, the disequilibrium hypothesis suggests that treatments to reduce neuroinflammation could be helpful as well. That’s not a bad finding, given the work underway in many diseases to find ways to reduce neuroinflammation.
Health Rising’s Donation Drive Update!
We look into everything we can. If you appreciate that, please support us!
Thanks to the dozens of people who have contributed over $4,000 to HR’s year-end fundraising drive. This illustrates one of Health Rising’s strengths – its breadth. When Miwa found small hearts in ME/CFS, we covered it. When Miwa demonstrated that the renin-aldosterone paradox could be causing the low blood volume issues in ME/CFS, we covered it – in spades. (It’s shown up in at least five blogs).
Now we’re onto disequilibrium – a known issue in these diseases, which, yes, we covered, and which Miwa is bringing a fresh look at. If you appreciate that kind of thoroughness and depth, please support us!
Support Health Rising and Keep the Information Flowing!
HEALTH RISING IS NOT A 501 (c) 3 NON-PROFIT
The Romberg Test
If I remember correctly, Dr. Cheney used the Romberg test, and Dr. Bateman has reported that the test is often positive in ME/CFS. The test is very simple. You stand, put your hands on your hips and you close your eyes for 30 seconds. (Another variation of the test has you put your arms out from your shoulders in so that you’re forming a cross.)
How to Assess Balance and Proprioception – Romberg Test – Clinical Skills – Dr Gill
Ten years ago I failed it – this time I passed it (:))
This large study (n=160 patients) found static disequilibrium in 25% and kinetic disequilibrium in 44% of participants. The ability to maintain “postural control,” i.e., stay steady without swaying, is controlled by pathways emanating from the brainstem. When they are impaired, we use our eyes to compensate for the loss of automatic control and maintain an upright posture. A 2015 study indicated how that happens in ME/CFS.
Thinking and Walking at the Same Time: Not a Good Idea in ME/CFS
This fascinating study asked people with ME/CFS and healthy controls to try to walk and think at the same time, exploring gait issues in ME/CFS. The study asked them to walk with eyes open, close their eyes, and walk and stop, and while they were walking, asked them what 100-7 was.
Miwa believes deep brain issues are contributing to, or even causing, orthostatic intolerance in some people.
If the person suddenly looked at the ground to place their feet, or became clumsy when they closed their eyes, or if their gait went wonky, or they stopped walking to figure out what 100-7 was, something was off.
About 25% of the ME/CFS patients looked down at their feet before they began walking, compared to 1% of the healthy controls. The gait of almost 90% of the ME/CFS patients deteriorated slightly or greatly when they closed their eyes, compared to only 11% of the healthy controls.
Finally, 56% of the ME/CFS patients stopped walking to figure out that knotty math problem 🙂 (100-7=?), while only 5% of the healthy controls did. This may be why it’s harder for some people with these diseases to maintain a conversation while walking.
Disequilibrium – A Key Factor?
Why does Miwa believe that disequilibrium is a more important feature of orthostatic intolerance than POTS? In the studies he’s done, patients who failed the 10-minute stand test almost uniformly experienced disequilibrium when standing, but only a small percentage also had POTS. Remarkably, all the POTS patients completed the 10-minute standing test (was their POTS treated?).
While larger studies are needed, the fact that patients with disequilibrium had the worst general health (PS scores) suggests that disequilibrium may be synonymous with poorer health in these diseases.

Disequilibrium can contribute to fatigue in several ways.
Disequilibrium can cause fatigue in several ways. Parkinson’s studies have shown that maintaining stability in the presence of instability is “metabolically expensive”. For one, it takes extra muscular effort to continually be aligning yourself while upright. It’s also cognitively challenging. When I had stability issues, I noticed that I had to consciously look around to orient myself. Plus, being unsure of where you are in physical space may cause you to brace, and that muscle tension burns up a lot of energy.
Finally, all of this could put more stress on what may be a failing sympathetic nervous system.
Treatment
Minocycline
Miwa’s small studies suggest that both rTMS or minocycline may be able to help with the disequilibrium issue. His recent 55-person, non-placebo-controlled, minocycline trial began after a patient of his reported that she’d recovered after using minocycline.
Why use an antibiotic to combat a central nervous system problem? Because minocycline is an unusual antibiotic. It’s able to cross the blood-brain barrier, and can reduce microglial activation, the production of inflammatory cytokines in the brain, and neuroinflammation. For instance, it’s been used to treat traumatic brain injury.

Miwa believes neuroinflammation in the brain is affecting the parts of the brain that control balance and gait.
In the pilot study, ME/CFS patients received oral minocycline (100 mg × 2 on the first day, followed by 100 mg/day for 41 days). Miwa reported that 76% of the 21 patients with disequilibrium no longer had it by the end of the study. Seven of the eight patients who couldn’t complete the 10-minute standing test were able to complete it.
Miwa created his own “performance status” score sheet, which looks much like the functionality score sheet created by David Bell, MD, for ME/CFS. The average PS increase (2 points) would translate to something like “a noticeable increase” in what you can do day to day.
There are some big provisos to this finding, though. The study was open-label (everyone knew what they were getting), there was no control group, and only a single clinician/clinic was involved. Plus, the fact that Miwa found that recently diagnosed ME/CFS patients improved the most could reflect that they were already gradually improving. Plus, while only 7% of patients weren’t able to finish this trial in an earlier study, a whopping 38% of patients didn’t.
Basically, the results cannot be trusted, but they do provide a nice basis for a bigger, more rigorous trial.
The rTMS trial
Miwa used rTMS over the DLPFC and M1 to enhance activity in the brainstem vestibular centers. These centers help us orient ourselves in space.
The rTMS was focused on the left dorsolateral prefrontal cortex (DLPFC) and the left primary motor cortex. Why would Miwa target the prefrontal cortex and the motor cortex – neither of which are located anywhere near the brainstem? Because these parts of the brain communicate with each other, and studies have shown that targeting these areas affects vestibular functioning in the brainstem. DLPFC inactivation has been observed in several studies and has been proposed by both UK and Japanese researchers to play a key role in the brain network underlying fatigue.
The 30-person 2023 ME/CFS study found that after rTMS, 10 out of 12 patients who were unable before were now able to complete the 10-minute standing testing, disequilibrium was resolved in 15 (88%) out of 17 patients, and neuropathic pain was reduced in seven (70%) out of 10 patients. Another small ME/CFS rTMS trial found, interestingly, that blood flows to the frontal lobes improved.
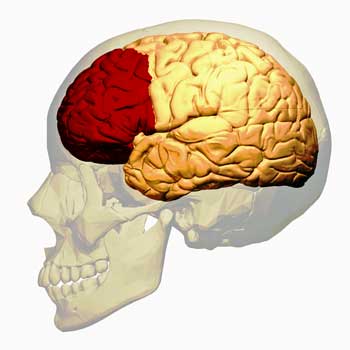
Miwa targeted an area of the brain – the dorsolateral prefrontal cortex – known to impact vestibular functioning. (The image shows the prefrontal cortex).
rTMS has received the most study in fibromyalgia. A systematic review of rTMS in FM concluded that rTMS reduces pain intensity and improves depressive symptoms, anxiety, and general health but that methodological issues (as always) were present. While methodological problems are present, enough studies have been done to identify a specific target and dose (M1 at 10 Hz) that helps. Miwa also targeted the motor cortex (M1) and the DLPFC, and used slightly different pulses. In another argument for going low and going slow, he had to reduce stimulation intensity for most patients.
While data suggests that rTMS may help with FM and ME/CFS, it won’t eliminate either condition. It may, though, be able to help with pain, disequilibrium, mood/anxiety, overall health, and quality of life.
Conclusion
If Miwa is right and disequilibrium is contributing to problems with standing, then the treatment focus shifts a bit. While we know that reduced blood flows to the brain are contributing to the orthostatic intolerance in ME/CFS and long COVID, the disequilibrium hypothesis suggests that treatments to reduce neuroinflammation could be helpful as well. That’s not a bad finding, given the work underway in many diseases to find ways to reduce neuroinflammation.

Once again, Miwa has introduced a new concept into ME/CFS.
Miwa reported that the oft-used tilt-table test can detect only orthostatic intolerance due to circulatory issues (reduced blood flow to the brain). Tests such as the Romberg and tandem walk tests are needed to detect orthostatic intolerance (symptoms triggered by standing) caused or contributed to by deep-brain issues.
Time will tell if Miwa or somebody else gets the funding to test his hypothesis. It would be great to see a study that assessed disequilibrium and performed brain scans before and after treatments.
Donation Drive Update
We look into everything we can. If you appreciate that, please support us!
Thanks to the dozens of people who have contributed over $4,000 to HR’s year-end fundraising drive. This illustrates one of Health Rising’s strengths – its breadth. When Miwa found small hearts in ME/CFS, we covered it. When Miwa demonstrated that the renin-aldosterone paradox could be causing the low blood volume issues in ME/CFS, we covered it – in spades. (It’s shown up in at least five blogs).
Now we’re onto disequilibrium – a known issue in these diseases, which, yes, we covered, and which Miwa is bringing a fresh look at. If you appreciate that kind of thoroughness and depth, please support us!
Support Health Rising and Keep the Information Flowing!
HEALTH RISING IS NOT A 501 (c) 3 NON-PROFIT



On October 7th, I was returning to my bed from the bathroom around 4 in the morning. Suddenly, I passed out and fell against the desk next to the bed and did a lot of damage to my body. I was so dizzy when I woke up, I couldn’t walk without my husband’s help. I was really scared. Was this a stroke? I didn’t seem to have any of the residual effects you would expect from a stroke.
I did a lot of research on Long Covid and learned that passing out was not uncommon.
I live in a two-story house and two days a week I drive a hour to my office in heavy traffic. I haven’t gone upstairs or driven since this episode.
I decided I had to get serious about new treatment options. One is a medicine that I won’t talk about until I see how it works for a month. The other is in the realm of alternative medicine…reiki. I always thought reiki was a bit out there, but a lovely practitioner let me try it for free. I have never felt so calm and peaceful and the next day, I had less dizziness and could walk better than I had in weeks. Of course, I did too much and didn’t feel as great the next day. Was it the reiki or the new med or a combination I don’t know, but if you live in Central Florida, I can recommend a wonderful reiki practitioner. As far as the new medicine, time will tell.
Please keep
Us updated on medicine.
I am not surprised that anything that reduces brain inflammation helps aspects of ME/CFS/FM. Supplements which are anti-inflammatory to the brain have pretty well gotten rid of my FM pain and greatly reduced my brain fog.
Which anti inflammatory supplements did you take please. Specifically for the brain.
I will them soon.
Sorry I meant I will post them soon.
Thank you Joan. Are you in the UK?
No, Wendy. I am in Canada. If I can be of any more help, let me know. I have researched all the supplements I take for their mode of action and for their safety. I don’t take that lightly.
Wendy, the list is posted below. Some are general anti-inflammatories but also anti-inflammatory to the brain, The one that surprised me is acetaminophen. One that I don’t do well without is dextromethorphan (Robitussin). It really helps my pain.
Could be the guaifenesin in the Robitussin. Guaifenesin alone helps many of us with pain.
Hi Denise. The gels I take do not have Guaifenesin in them. The only active ingredient is Dextromethorphan hydrobromide which has a number of effects on the brain. Simply said, it calms brain cells. This is the reason I chose to add it to my regime.
Thank you for sharing. Please look into how bromide displaces iodine in the body and the long term thyroid effects, including cancer, pain and less energy. ‘Iodine Crisis’ by Lynne Farrow.
I’d love to hear what’s worked for you 🙂
I posted the list below. I was going to respond to the low nor-epinephrine blog and probably will yet. Again I was not surprised that that family of neurotransmitter is low in CFS/FM. What I have read is the we are low in serotonin and nor-epinephrine and possibly dopamine. There are behaviours such as listening to music, exposure to cold and more that will raise them. Also some supplements may help.
Wow! I found this incredibly fascinating and exciting to read. I’d just this morning been thinking about my experiences of a combination ME/CFS and Post Concussion Syndrome (PCS) relapse that started a week ago. I do a version of the Romberg test at times to check how much my PCS is flaring up. Earlier in the week, when doing the test, I’d start to fall over after 22 seconds (and with quickly openening my eyes, I save
my self from falling). As I approach my limit, I find nausia flares up and worsens. I improved over several days, lasting longer before stating to fall. Then a couple of days ago, during the test, I found I wasn’t starting to fall, but I was getting waves of nausia and feeling a bit like losing my balance at times, but repeatedly kept coming right (and that’s happened at times before, with the test). I could tell it was a somewhat stressful challenge for my brain. It got me wondering about my OI and of my BP dropping (and at times narrowing of pulse pressure). I wondered if they were not the only causes of my OI experiences and if there were also neurological ones restricting how long I could be on my feet, and relating to the stress on my brain and body of keeping balance.
I got ME/CFS and Fibromyalgia in 1983 (mostly bed-ridden) then around 2009-2010, I had mostly recovered and returned to work. Unfortunately, in 2018, I had a bad bump on my head causing a concussion and leaving me with Post Concussion Syndrome since, and the return of CFS symptoms. I had a lot of vestibular/Occular problems with the head injury (I’ve improved over time, but not recovered). When my therapist did the Romberg test on me early days of the head injury, I’d fall over after only a few seconds (and the same happened later, when I’d have a relapse). In 2021, I developed Microvascular Angina. Interestingly, Medications for my heart condition for opening up blood vessels inc Isodorbide Mononitrate, and GTN spray and patches give me improvement in my vision as well as make me stronger on my feet, with better balance. The improvent with the GTN is short lived though, but spectacular. I marvel at the world looking clearer, brighter and more 3D again, like before the head injury. I assume it’s due to improved blood flow to the brain. However if I have too much GTN, I get ME/CFS/FM pains down my limbs.
Another interesting thing is that when I had a scan of my heart a few years ago, the radiologist said ‘Oh (with considerable surprise), you have a small heart’. Then he Said ‘but that’s OK’. I took his word fot it being OK, and didn’t think anything of it, until months later, I read about the association of small hearts and CFS/ME.
Could this be merely inflammation, or might there be undetected neuronal damage between the visual cortex—situated just above the cerebellum—and brain regions involved in memory and interhemispheric communication?
Since the COVID pandemic, I’ve experienced short-term memory issues, particularly difficulty recalling acronyms while sitting upright and writing. Interestingly, although my blood pressure remains stable whether I’m sitting or lying down, I notice a marked improvement in memory when I’m lying down and reading.
This raises important questions: Is the underlying cause simply brain inflammation, or could it involve demyelination, reduced white matter integrity, or abnormalities in cerebrospinal fluid (CSF) dynamics—such as overproduction, underproduction, or impaired circulation? Could these symptoms also be linked to structural conditions like spinal stenosis or spondylitis affecting neural pathways involved in visual and motor processing?
An MRI, neuropsychological testing, or CSF analysis could bring clarity.
The minocycline is interesting. Very well known to reduce neuroinflammation, so I have always been surprised that it hasn’t been trialled in ME/CFS. Perhaps because of the side effect profile.
It has though, I think there have been several trials with certain success. Nothing placebo-controlled though I think. Side effects could be an issue long-term.
Here’s an overview of Minocycline studies:
https://scholar.google.com/scholar?hl=de&as_sdt=0%2C5&q=me%2Fcfs+minocycline&btnG=
I struggle with one methodological problem. Those tests with walking and talking or standing 30 s. How can you rule out the impaired blood flow? Or we can assume that impaired blood flow in brain = brain stem problem? We need the test where you can see the brainstem problem without standing position.
Or maybe there is something I didn’t get.
I am sure about my blood flow problem in vertical positions. For me it is impossible to remember the PIN to my card when I stand in front of cashier. But when I am on a wheelchair no problems. My speaking and thinking is the best when I lay down.
I have to move to Mars, Moon or space station ;).
I don’t think you can. Studies have shown this is a problem for almost everyone. It’s part of the picture. I think Miwa goes quite a bit too far by discarding POTS. Note that he found disequilibrium in at most about 45% of patients and other studies have found lower rates. For me, the takeaway from his work is that that should be looked into as well. I hope he or someone can explore this in bigger studies.
Though I am much better – my immune system and infections have been addressed along with mitochondrial rehabilitation and autoimmunity, my pots is better and so is fatigue, but I have lingering postural instability.
I can walk, but standing in one place for any like the time is problematic.
I greatly appreciate learning about this. I would not take minocycline and risk damage to my microbiome, nor do I have access to transcranial stimulation, but I think I will try taking buzzwellia or curcumin to reduce any lingering brain information.
This is likely why LDN works. It’s reducing brain inflammation. More good news! 🙂
That’s the idea with LDN 🙂
Off topic, but these are interesting thoughts from Ron Davis and others at Stanford on the potential important role of glymphatic issues in ME/CFS:
https://www.mdpi.com/1422-0067/26/23/11524?utm_source=substack&utm_medium=email
Thanks for this interesting blog. I’ve noticed too that several Japanese researchers do great work.
In May there was one of them in Berlin, originally an MS researchers. He is also researching brain inflammation in ME/CFS.
Since I speak German I don’t fully understand what’s actually talked about here. I know benign paroxysmal positional vertigo (BPPV).
I had it once about ten days after a serious ME/CFS flare that involved brain inflammation in January 2025.
About ten days after the flare when I had overdone it a little bit one afternoon I woke up and felt so dizzy that I immediately felt sick and vomited.
Half a day later with bed rest I could get up again and walk without getting feeling sick. The vertigo stayed with me for many weeks though and got better only very slowly.
I saw an emergency GP because I was on a holiday at a time. He confirmed the diagnosis and told me that vertigo and dizziness are quite common after flu-like infections that sometimes can affect also the brain.
I got bad vertigo, for the first time ever, about two years ago after being infected with covid.
I had dizziness for about 6 months after.
Btw, the vertigo came on about 10 days after that infection started…
My list is still a work in progress. I’m adding Baicalin (Chinese skull cap) to this list It may stay on the list or not. As far as I can find out these are safe for anyone taking thyroid meds, and low dose antidepressant. I have researched these for safety and taken many of them for several years now with no ill effects except perhaps a little gut trouble – hard to tell as I have that anyway. I started with a few i.e. quercetin and resveratrol and added to them. When (if?) I reach a point that I feel I have the benefits I want, I will start to prune my list to see if I can manage with less. Here’s the list: I’m hoping the formatting doesn’t get messed up.
Neuroprotective/Anti-inflammatory for pain and brain fog:
(Daily unless noted otherwise.)
Dextromethorphan (Robitussin) 15 -20 mg 2 x daily
– neuroprotective, SNRI
Quercetin with bromelain or Vit C 400 mg 2 x daily
– anti-inflammatory, neuroprotective, antioxidant
Resveratrol 300 mg 2 x daily
– anti-inflammatory, neuroprotective, antioxidant
Acetaminophen
– anti-inflammatory, neuroprotective 500mg 2x daily
Fisetin (Bio fisetin) 100 mg
– reduces neuroinflammation
Luteolin 100 mg
– anti-inflammatory, neuroprotective, antioxidant
Boswellia (Maxi-Boz) 333 mg
– anti-inflammatory, neuroprotective, antioxidant
Cinnamon 1000 mg.
– reduces neuro inflammation
Curcumin 150 mg
, reduces neuroinflammation, antioxidant
Baicalin (Chinese skull cap) 400 mg
possibly neuroprotective & mitochondrial support
As needed:
Robax (methocarbamol) as needed for pain/ brain fog 1-2 tabs
GABA for anxiety/sleep 250-500 mg
Our organization has done a lot of work on the risks of taking acetaminophen during pregnancy. This morning, however, I found this new warning on acetaminophen.
“A Tylenol rash can range from mild to severe, and if you develop any rash while taking a product containing acetaminophen (the active ingredient in Tylenol), you should stop taking it immediately and seek medical attention. Severe reactions, which are rare but potentially fatal, can include blistering, peeling skin, and widespread red lesions, and require immediate medical help. If you have a serious skin reaction, you should never take acetaminophen or any product containing it again.”
Acetaminophen is not an anti-inflammatory drug, but in certain instances it can have severe effects on the liver. Acetaminophen products carry a prominent liver warning that advises against use with alcohol due to the significant risk of severe liver damage.
It is a mistake to assume that over-the-counter drugs are benign.
I think if you read this article you will see that acetaminophen is anti-inflammatory to neurons. “Acetaminophen inhibits neuronal inflammation and protects neurons from oxidative stress”
I never assume that OTC drugs are benign, or supplements, for that matter.
Here is the link to that article.
https://pmc.ncbi.nlm.nih.gov/articles/PMC2662814/
Macabre story; just in time for Christmas.
I’ve been dizzy for over 5 years, since my one and only bout of acute Covid. Was tested for POTS but don’t have it. For me it has been the single most debilitating symptom of Long Covid. But when I try to get treated for it I am asked whether I have vertigo or pre-syncope and I have neither. I’ve tried electrolytes and copious amounts of water, oral rehydration salts and copious amounts of water, and compression garments in combination with those things; nothing has helped. Then I read this Health Rising post and it just completely changed my thinking. Disequilibrium! Of course that’s what I have! I recognized myself immediately on reading the symptoms of disequilibrium. So does that mean I can dispense with all that water, which contributes rather a lot to my insomnia? Can I quit the horrible tasting oral rehydration salts? Do compression garments make any difference? I have now quit all those things to see if I really need them, because they sure as heck haven’t helped with the “dizziness”, and they do have unpleasant side effects, for me.