


Geoff’s Narration
The GIST
The idea that something in the blood is causing or contributing to ME/CFS, fibromyalgia, and/or long COVID is so tantalizing. For one thing, while it may not be easy to identify that substance, once it is found, the idea that all that may be needed is to turn it off, block, or neutralize it (a common strategy in many diseases) has a simplicity that is so appealing in such complex and mysterious diseases.
As time has gone on, the evidence has continued to build. At least 11 studies have found that exposing muscle, microglial, endothelial, or muscle cells, as well as platelets, to ME/CFS, fibromyalgia, or long-COVID serum, plasma, or IgG caused things to go south.
The GIST
-

Something in the blood may be contributing to ME/CFS and long COVID, but it doesn’t appear to be affecting the mitochondria in their muscles.
The idea that something in the blood is causing or contributing to ME/CFS, fibromyalgia, and/or long COVID is so tantalizing. The idea that, once found, all that may be needed is to turn it off, block it, or neutralize it (a common strategy in many diseases) is so appealing in its simplicity.
- Over the past ten years or so, at least 12 studies have found that exposing muscle, microglial, endothelial, or muscle cells, as well as platelets, to ME/CFS, fibromyalgia, or long-COVID serum, plasma, or IgG has caused things to go south in those tissues.
- The fly in the ointment, however, has been the small size and a lack of validation by external research groups. Until these findings are validated they will always be suspect.
- Recently, a UK group lead by Ryback attempted to replicate 2016 study results which found that serum from ME/CFS patients dramatically reduced muscle mitochondria’s ability to produce energy. This finding was exciting because it potentially explained why people with ME/CFS have so much trouble with exertion. The nub, though, was that the initial test was quite small – just 25 ME/CFS patients and healthy controls.
- The Ryback study, which employed 5x’s as many participants, didn’t find that ME/CFS serum affected mitochondrial energy production at all.
- While that was disappointing, it was also a narrow finding that didn’t bear on other studies that found that ME/CFS, fibromyalgia, or long COVID serum or IgG antibodies inhibited other tissues, such as glial cells and endothelial cells.
- Note that it also has no bearing on the exercise study findings. They still stand. It simply appears that they’re not caused by something in the blood that is taking an axe to the mitochondria in the muscles. Many other possibilities are present.
- In fact, this study may have cleared the way for a different, and perhaps more likely alternative: that something in the blood is interfering with the endothelial cells lining the blood vessels. At least four studies have found that transferring fluids from patients with complex chronic illnesses into endothelial cells disrupts those cells.
- This is potentially a vitally important finding, as endothelial cells regulate blood vessel function and blood flows, particularly in the small capillaries that feed tissues. Reduced blood flows, which seem more and more likely, could explain why people with ME/CFS and long COVID have such problems with exertion.
- Health Rising recently reported on Prusty’s study, which found that IgG antibodies from ME/CFS and long COVID patients fragmented the mitochondria in endothelial cells. The mitochondria were still producing ATP, but they appeared to be “hunkered down” and not functioning well, which may be enough to reduce blood flow and impair energy production in the muscles.
- As so often happens with science, closing off one door opens another.
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit
The Ryback Replication
Audrey Ryback and company picked a great study to attempt to replicate – Fluge/Mella’s 2016 study, “Metabolic profiling indicates impaired pyruvate dehydrogenase function in myalgic encephalopathy/chronic fatigue syndrome“, may have started the whole “something in the blood” saga off.
The idea that something in the blood is contributing to or causing ME/CFS is enticing in its directness.

The paper was mostly focused on amino acid changes, but a secondary finding that muscle cells exposed to ME/CFS serum exhibited dramatically increased rates of respiration and lactate secretion clearly raised eyebrows. It suggested that something in the serum of ME/CFS patients was stressing their muscles and causing them to enter anaerobic respiration (e.g., the lactate finding). It just made so much sense.
This secondary effort (like so many secondary efforts) was based, though, on a very small sample size – just 24 ME/CFS and healthy control samples – not nearly enough to be representative for a disease as large and heterogeneous as ME/CFS.
The Study
In “Indistinguishable mitochondrial phenotypes after exposure of healthy myoblasts to myalgic encephalomyelitis/chronic fatigue syndrome or control serum“, Ryback and company attempted to replicate the findings using the same procedure (using the Seahorse machine) but with about 5 times as many samples (n=120).
The Ryback study had a leg up on the original study in some other ways. The ME/CFS patients all met the Canadian Criteria, were collected within the same time frame, and were less susceptible to “batch effects”, where processing different batches produces different outcomes.
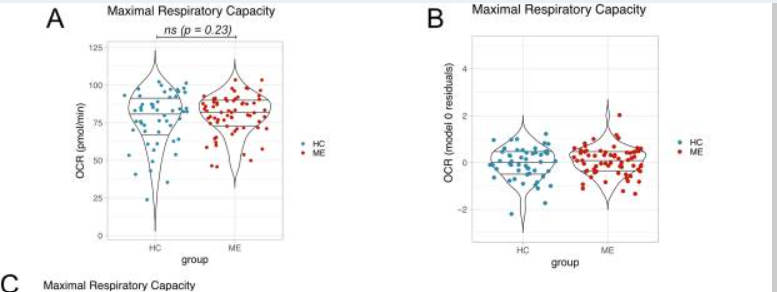
Whoops! Maximum mitochondrial capacity is the same in muscle samples exposed to ME/CFS patients and healthy control serum.

No differences were seen in any of the mitochondrial measures.
No differences, however, were seen in the key finding – the “oxygen consumption rate” at “maximal respiratory capacity” nor in any other mitochondrial measures. This means that when pushed, there was no difference in the amount of energy being produced by ME/CFS and healthy control muscle cells.
The authors concluded: “Results from our study provide strong evidence against the hypothesis that ME blood factors differentially affect healthy myoblast mitochondrial phenotypes in vitro.” (When researchers, who are inherently conservative, use words like “strong evidence”, it’s clear they believe the issue has been settled :)).
Several things could have gone wrong in the Fluge/Mella study. The ME/CFS patients may not have been representative, “batch effects” – those elusive and dreaded changes that sometimes occur when different batches are run at different times – could have played a role. (Check out an interesting discussion in the reviewers’ section of the paper for more on this.) With money short, many ME/CFS researchers may simply not have the funding to be as careful as possible. (Ron Davis has talked about how important sampling procedures/batch effects, etc., are.)
Fluge/Mella’s dramatic finding was begging for replication, and the only pity was that it took ten years to attempt it. The Ponting paper dashed a large bucket of cold water on the idea that something in the blood is whacking the muscle mitochondria in ME/CFS and preventing them from producing energy.
Narrow Finding
This was a narrow finding that applied to just one aspect of the “something in the blood” hypotheses.
It’s also a “narrow” finding that applies strictly to one situation: ME/CFS serum and muscle mitochondria. It does not mean that something in the blood isn’t affecting people with ME/CFS. Indeed, the authors write, “Our results do not rule out the possibility of ME-biased factors being present in serum”, and at least ten other ME/CFS/FM/long-COVID studies suggest that something in the blood affects other parts of the body.
- 2016 -X- Fluge/Mella reported that exposing muscle cells to ME/CFS serum increased lactate production and mitochondrial activity.
- 2020 – ME/CFS serum fragmented mitochondria and produced an antiviral state in the lab.
- 2022 – Endothelial cells exposed to long-COVID serum exhibited reduced nitric oxide (NO) functioning.
- 2022 – Endothelial cells exposed to ME/CFS plasma showed reduced nitric oxide (NO) production.
- 2023 – Exposing endothelial cells to long-COVID serum produced inflammation.
- 2023 – ME/CFS serum produced increased reactive oxygen species production in human microglial cells.
- 2024 – Long-COVID plasma activated platelets.
- 2024 – Exposing the endothelial cells from human brains to serum from long-COVID patients induces inflammation.
- 2024 – Transferring long-COVID IgG antibodies into mice produced increased pain sensitivity, loss of balance/coordination, and a trend toward weakness, and small fiber neuropathy.
- 2025 – Exposing “muscles on a chip” to ME/CFS or long-COVID serum produced weakened muscles.
- 2025 (?) – Exosomes isolated from patients with ME/CFS stimulated the microglia to produce IL1B.
- 2026 – Prusty et al. find that IgG from ME/CFS and long-COVID ME/CFS patients fragments the mitochondria in endothelial cells.
Plus, a few studies that used plasmapheresis or immunoadsorption to remove potentially offending substances from the blood have generally had at least moderate results.
The Ryback study, however, provides a cautionary tale about how much confidence we can place in the “something in the blood” hypothesis, given that the findings have not been replicated. As enticing as these findings are, they generally need to be replicated by external labs for us to rely on them.
This finding also doesn’t affect the exercise findings. The energy impairment observed during exercise could be due to reduced oxygen delivery to the muscles (which seems increasingly likely), mitochondrial inefficiency, autonomic nervous system issues, etc.
Of course, it’s also possible that mitochondrial ATP production in ME/CFS patients’ muscles is impaired; it’s just not being impaired by something in the blood.
Close One Door – Another Opens

Several studies suggest that something in the blood may be impairing the blood vessels.
The Ponting finding would seem to put a premium on endothelial cells. Six of the ten “something in the blood” studies have found that something is impacting endothelial cells.
Prusty’s recent study is a case in point. It found that ME/CFS and long-COVID IgG fragmented the mitochondria in endothelial cells but did not significantly affect energy production. That provides an intriguing possibility: maybe the mitochondria don’t have to be completely whacked to cause problems – maybe they just need to be disturbed enough.
Prusty found that in a substantial subset of patients, mitochondrial fragmentation placed endothelial cells under stress, leaving them less resilient and less able to function overall.
The study suggested that the cells had hunkered down, aka Naviaux’s cell danger response. Simply doing that could be enough to hamper blood flows to the muscles and impair them from producing normal amounts of energy. Indeed, as noted earlier, four studies, some of which used the same cell types, have suggested that something in the blood is affecting the blood vessels.
In the end, it was good to see someone finally try to replicate a “something in the blood” finding. While Ryback was unable to replicate Fluge/Mella’s finding of 10 years ago, her findings simply close out one narrow possibility – and in doing so, bring into focus other possibilities (reduced blood flows to the muscles) which, in the end, may be more likely anyway.



SO THIS ONE STUDY INVALIDATES THE FINDINGS 0F 12 OTHER STUDIES? IF THEY REALLY WANT TO FIND OUT IF THERE IS SOMETHING IN THE BLOOD CAUSING (AND POSSIBLY TRANSMITING) ME/CFS, THE GOVERNMENT WOULD FUND THREE STUDIES AT THE SAME TIME WITH IDENTICAL PROTOCOLS. BUT RESEARCHERS ARE ALL FIGHTING FOR FUNDING FOR THEIR LABS AND DON’T WANT TO SHARE CREDIT FOR AN IMPORTANT DISCOVERY. AND THE GOV CERTAINLY DOESN’T WANT TO CONFIRM A POSSIBLY TRANSMISSABLE AGENT. BUT, OH YEAH, YOU CAN’T DONATE BLOOD IF YOU HAVE ME/CFS.
Actually it only invalidates one study (I changed the title of the blog to clarify that) but yes, we really do need a large-organized effort to figure out the “something in the blood” question.
. The “something in the blood” hypothesis with regard to endothelial cells – which was not assessed in this study – actually looks quite strong with 4 studies finding, one way or another, that something in the blood affects the blood vessels 🙂
If you look carefully into the technologies which the Prusty Lab are deploying in order to understand what’s going on, you will see that they are pursuing an innovative and really interesting approach to unravelling the problem.
What amazes me is that they are doing this on a small budget and they are the only lab in the world who are employing innovative technologies in this way.
They put to shame those huge Government research organisations (such as the NIH) with their big budgets and large numbers of researchers, who seem incapable of thinking differently and embracing a Mitochondrially-driven disease paradigm as per ME/cfs and Long-COVID.
https://www.prustylab.org/current-research-areas
That’s good to hear, Paul. Our researchers, including Prusty, do seem to be uncommonly creative. I am again and again surprised to see our small field substantially ahead of the long COVID field in some areas.
There have already been studies on covid and shows that it tampers with the The Ace receptors which regulates blood flow in the brain the heart the lungs and the kidneys. So it’s not such a far leap to think that chronic fatigue syndrome and fibromyalgia could have similar causation.
This study used serum. Sadly, it did not test plasma.
So true!!
Well, if we all have leaky gut, wouldn’t our food particals be in our blood and possibly biofilms and/or anything else that are found in our microbiome re:bacteria, inflammatory cytokines
I would think they would. One study which found that exercise greatly increase bacterial translocation provided one way exercise could enhance inflammation.
This is being seen in Long COVID microbiome studies. Many, many patients are deficient in Akkermansia muciniphila which increases Treg cells that balance the immune system, as well as stimulates endogenous GLP-1, and ensures gut barrier integrity to prevent translocation and protect the tight junctions. Hence the explosion of GLP-1 testimonials – part of why these medications do what they do, is they cause Akkermansia to bloom in numbers. Exercise worsens gut translocation, which in turn causes inflammation, cytokines, etc.
Imbalanced gut also causes microglial activation, lower anti-inflammatory compounds like Butyrate that also help stabilize the immune system, modulates NF-kB and mTOR in undesirable ways, which can cause immune activation that leads to cytokine release.
The GLP-1 stabilizes mast cells, to boot. I’ve now read 500 journal articles on the microbiome, and have been playing with it for a year with broad and now targeted therapies. I’ve moved it massively, lowering symptom burden and requiring lowered or discontinued medication, and supplements.
The one thing I haven’t been able to do yet is get Akkermansia to come back – profusely feeding it and the GLP-1 caused no bloom. 0.0 level on tons of tests. I’m now trying to engraft it via state-of-the-art probiotics coupled with compounds that make it bloom. Time will tell how this ends up working, may have to pivot and try again, but eventually I think I will find an answer, and with it, potential remission.
Hi! I’m really interested in what you have done that have moved the needle for your symptoms and microbiome (I do realize it might be very long for a comment).
If you have the time and energy, could you please share some your methods? Or perhaps it could be possible to send a blog post that Cort could share?
I myself got a boost from Mounjaro, but still some ways to go.
Hi,
I’d love to share something in-depth – there’s a lot to the science that I’ve learned over the last year. I’ve used metagenomic testing which can identify bacterial functions, inflammatory properties, health promoting properties, etc. This is what has guided me to know what bacteria are living in my gut, and then I applied various modalities from broad to narrow to really target everything I could.
In my case, I had Citrobacter, high R. gnavus, and high P. dorei, they are now suppressed into the noise floor. Additionally, other interventions lowered elevated beta-glucuronidase which can recycle medications and other hormones.
The GLP-1 has helped me recover lost foods, which has been incredible. So much better regulation and function of my gut.
I actually am registered as a practitioner now for the company that I used because of how much I believe in it – I have a background in herbalism/vitalism and always knew the gut was important, but we can now see everything, including the why.
Hi Corey!
Sorry I didn’t get around to replying before. I just wanted to let you know I really appreciated your comments and your knowledge!
I got the possibility to switch to tirzepatide from Wegovy before Christmas, and it has actually helped a lot! Wegovy helped with weight, but not fatigue or PEM, only tirzepatide did that.
I have also added lithium, which might also be helping in it’s own way (dampening neuroinflammation and being antiviral), but I think the tirzepatide has made a huge change for me! I noticed effects around 6-7 weeks after starting it.
I am so much better. I still get some bad days, but my stamina is better, I live a more normal life than before, and my quality of life is a lot better. Also, my mood is finally, after feeling situationally depressed for years now, lifting somewhat.
I am trying to do other things for my gut health, little by little, adding fermented food, eating a little more vegetarian etc.
I don’t have much mental stamina left right now to make huge changes and sticking to them right now as I feel I have been in an 8 year marathon, but I find your approach intriguing and I’m going to keep looking into it more!
I have also figured out I am suffering from B6-toxicity, adding to my neuropathic pains. I am guessing this also produces it’s own symptoms, affecting the autonomic nervous system. I have followed a diet with less b6, and this has helped – albeit looking at the science it will take a couple of years with strict diet and whatever activity I can manage probably before this is fully resolved. I forgot about it for a little while and ate normally for a week, and bam – started feeling bad the fifth day and woke up the sixth day with sharp neuropathic pain in hands and feet again. So it will be a challenge to eat for gut bacteria but at the same time follow a low-ish B6-diet.
Thank you for sharing your knowledge, just wanted to let you know it really helped me!
Bonjour, avez vous songé à la transplantation fécale? Et si non pourquoi ?
It reminds me of the XMRV saga. But if this research(n=1) is well conducted then it can scientifically undermine a theory and other studies. The blood of ME patients is stickier and stiffer. Maybe somewhat related to fat and red blood cells. This hinders oxygen and other nutrients from entering the cells. I would like to see much more research into this phenomenon.
*IF* I get it right, there may be a small difference in method detail that *could* explain the difference in results (Note that I did not re-read all details of the text due to exhaustion so I could have missed the info in the original Fluge and Mella paper):
The 2026 paper says:
“Thresholds for data exclusions were decided before unblinding. We excluded wells with cell counts below 8000 and above 35000 cells as well as OCR or ECAR measurements”
“OCR and ECAR are both dependent on cell numbers, and normalizing measures based on cell numbers was carried out as recommended by Agilent [24,25]. Indeed, we observed significant positive correlations between cell count and measurements at maximal respiratory capacity for both OCR (r2 = 0.36, p < 0.0001) and ECAR (r2 = 0.88, p It *seems* to me that the 2026 study normalized OCR and ECAR for cell count (and excluded samples with lower and upper extreme number of cell counts) while the 2016 study did not.
=> the 2026 study concludes that OCR and ECAR correlate much more with cell count then with HC versus ME/CFS status, which makes sense given the wide number of cells per sample.
=> since “standard” cells were growen and used, they did not differ in *expected* quality and cell count before applying either (some percentage) of HC versus ME/CFS plasma
=> BUT the cell count before applying either (some percentage) of HC versus ME/CFS plasma *WILL* see more then significant variation over each sample and with it between any to halves if one were to random split these in two batches half the size.
=> This will add a lot of variation in initial cell counts in each subgroup (HC versus ME/CFS) and with it OCR and ECAR IF cell count was not taken into account in the 2016 study.
=> This still leaves the option open that adding ME/CFS plasma to the samples killed off relatively more cells in the sample then adding HC plasma. Assuming the cell count at day 1 and day 6 are the same in all samples is IMO a bit optimistic and as far as I see the 2026 study did not check it.
=> From this point of view, the 2026 study would (IF the 2016 one did leave out normalizing for cell count) be methodologically stronger but comparing both 2016 and 2026 studies *might* point to a relatively higher dying of cells in ME/CFS plasma (or a reduced multiplication rate of cells between day 1 and 6).
I found this in the 2026 paper:
“4) In Fluge et al, data were not normalised by cell count or protein concentration. We observed a strong correlation of OCR and ECAR with cell counts and therefore accounted for cell numbers in our analysis. However, no differences in cell counts were observed between ME and HC, so are unlikely to have contributed to ME serum effects previously observed by Fluge et al.”
=> So Fluge and Mella did not normalize by cell count. This IMO already undermines their results.
=> This study says “However, no differences in cell counts were observed between ME and HC, so are unlikely to have contributed to ME serum effects previously observed by Fluge et al.”.
I say OCR per sample should differ massively if sample 1 can for example has 8500 cells versus sample 2 34000 cells. That’s a 1 to 4 ratio and 4 times as many cells are bound to consume more oxygen in total.
The question here is: do they mean with “However, no differences in cell counts were observed between ME and HC, so are unlikely to have contributed to ME serum effects previously observed by Fluge et al.” that the mean (number of cells per sample) in *their particular* (2026 study) batch is equal enough in both their HC and ME/CFS group? If so, then they disregard that the mean values *also* show a great random distribution (per each test / study setup) *and* that the 2026 study with a lot more total samples would have a lot lower variation between the two mean values (compared to the 2016 study).
=> With over 1:4 variation in sample cell counts, a lower total number of samples *is bound* to see large statistic variation in average OCR and ECAR values in the 2016 study. It’s hard to beat statistics with too small sample numbers!
=> That still leaves the option that initial number of cells per sample before adding HC or ME/CFS plasma differs from the number of cells in that sample after addition of HC or ME/CFS plasma after 6 days. I wouldn’t count on that making up the difference however but it might be worth investigating.
I think they do mean “batch is equal enough in both their HC and ME/CFS group” with “However, no differences in cell counts were observed between ME and HC, so are unlikely to have contributed to ME serum effects previously observed by Fluge et al.”. But are they referring to day 1 or day 6?
I know it is a different study, but thinking back to Davis’s work with the effects of HC vs ME/CFS plasma and the nano-needle, that whole study was based around the extremely sick patient cohort. No need to control for PEM with those poor people – their whole life is PEM, and then some. But given the strength of that study’s signal, I also wonder if not accounting for something inherent to ME/CFS that wipes out the ME/CFS cohort cells isn’t a bit of an issue. Basing results on OCR and ECAR that strongly correlate with the number of cells that survived over six days (but not checking those cell numbers) seems a bit like doing an economic productivity analysis of the USSR vs Switzerland in 1942 but excluding those cities with low civilian population density.
Based on the work of Robert Naviaux, MD PhD on the Cell Danger Response, I wonder if anyone has been investigating whether there is more ATP in the serum of ME/CFS and long Covid patients. If there is elevated circulating ATP in some but not all ME/CFS, etc. patients, then the question would be, was ATP elevated during the onset of ME/CFS, etc. and then returned to baseline later after the Cell Danger Response had been activated by the purinergic signaling system.
If elevated ATP is found in the serum of some ME/CFS, etc. patients, it would then make sense to do a study to see if exposing muscle cell mitochondria to serum selected for its elevated ATP causes the mitochondria to reduce energy output, consistent with a “Dauer reaction” response that conserves cellular energy production in the face of a challenge (hence the name, “Cell Danger Response).
Does that make sense?
Great question! I asked ChatGPT about this and while it makes sense it is not easy to do. Thanks for bringing it up 🙂
“So the best answer is: yes, eATP in blood can be tested, but it is technically fragile and hard to interpret, which is probably why it has not become a routine biomarker for ME/CFS. If someone wanted to study this seriously, the stronger approach would usually be a research protocol that measures not just ATP, but also related purinergic markers such as ADP, AMP, adenosine, ectonucleotidase activity, hemolysis indices, and perhaps standardized pre/post-orthostatic or post-exertional sampling. That last part is an inference about better study design rather than an established clinical standard.”
Thanks, Cort. That’s very helpful.
Generally I am frustrated by the siloing and “blind men and the elephant” character of so much work that is being done looking for “the” answer to ME/CFS and long Covid.
By way of background, I have lived with ME/CFS for over 30 years. In the early nineties I cofounded a medical practice with a physician who was struggling with similar medical issues as I was. I served in the roles of office manager and director of patient education. We networked with leading clinicians who were having success and learned everything that could be known at the time, much of which seems to be ignored or forgotten nowadays by researchers looking to “solve” ME/CFS.
For example, it appears that in the onset of ME/CFS there is often an insult to the hypothalamus due to hyperinflammation that leads to a “brownout” of the entire endocrine system. This will be something like panhypopituitarism but not as severe. Labwork will show values for cortisol, testosterone/estrogen and thyroid trending in the lower third or so of the reference range. Mainstream clinicians will look at that and say, “There’s nothing wrong.” Integrative doctors familiar with this work will supplement each hormone to bring the lab values solidly into the middle of the reference range, often with striking improvements clinically.
In my own case, for several years I benefited from supplementing thyroid hormone (in the form of sustained release T3 to address a possible cellular conversion defect in which T4 was getting converted by the dehydrogenase enzyme into inactive reverse T3 instead of normal, active T3. That, btw, is another example of a Dauer reaction, similar to the Cell Danger Response in that it inhibits energy production in response to overwhelming stress).
Eventually I didn’t need to continue supplementing thyroid and stopped several years ago. However, I have continued supplementing hydrocortisone and testosterone to this day and find them EXTREMELY helpful in allowing me to function well enough to remain active and productive.
It is important to note that there is huge misunderstanding and I would have to say, ignorance, about the safety of hydrocortisone and its proper use that has prevented it from being properly documented and made use of. Specifically, hydrocortisone is a naturally occurring hormone that is necessary to maintain life. If there is mild adrenal insufficiency or low adrenal reserves, which is OFTEN the case with ME/CFS, judiciously supplementing hydrocortisone with doses BELOW REPLACEMENT DOSAGE so the adrenals are not suppressed (typically 5 – 20 milligrams/day) can produce impressive benefits.
Now let’s think about this.
SO much of the work on ME/CFS and long Covid focuses on inflammation, going into elaborate detail about the complex biochemistries involved. But NONE of that research that I’m aware of considers the possibility that much of that inflammation can settle down if adequate plasma cortisol levels are established and maintained by skillfully supplementing hydrocortisone with physiological, sub-replacement (not supraphysiological, pharmaceutical) dosages. We may not even need to know all the subtle mechanisms of inflammation involved if we can bring inflammation down globally in a way that creates a more normal endocrine/immune homeostasis.
I’ve experienced this in my own 30+ year experience with ME/CFS. I am convinced my illness has been much milder with MUCH less inflammatory activity because I have appropriately treated my adrenal insufficiency all these years.
If you look at research into “low dose” hydrocortisone therapy safety, you’ll see the research is worse than useless, “designed to fail” because it uses dosages above 25 mg/day (the average replacement dose, which WILL have the damaging side effect of suppressing adrenal function) and then claims “low dose” hydrocortisone therapy is not safe. I’m sorry, but that isn’t true. True low dose hydrocortisone therapy will be in the 5 – 20 mg range, and there is ZERO research that I’ve seen that conscientiously examines the effects of supplementation that is appropriately in that range.
If you look at the research on hydrocortisone supplementation and ME/CFS you’ll see that 30% of patients reported improvement. And this is from a VERY random sample that, if I remember correctly from reading the article, didn’t screen the subjects to only include those whose labwork suggested mild adrenal insufficiency or low adrenal reserves (as defined by the pioneering endocrinologist Dr. William Mk. Jefferies, not as defined by conventional endocrinology standard of care guidelines). So it is likely that research cohort not only did not distinguish whether the dosages involved were appropriate but also didn’t screen patients (with 4X salivary cortisol or Cortrosyn simulation testing) to determine whether they would even have been likely candidates for successful supplementation.
The hormone part of ME/CFS is one leg of the elephant. (“This wonder of an elephant is very like a tree!”) but it is just one dimension. ME/CFS is multidimensional and will benefit the most when as many dimensions as possible can be addressed at once. In many instances, one dimension will be predominant and you will see a dramatic improvement or even cure just from addressing that one dimension, but long-standing cases will likely tend to be more multifactorial.
That makes looking for “the” answer to be naive, in my opinion.
A semi-exception to this will be work that looks for an underlying mechanism that generates the whole galaxy of dysfunction across various dimensions. In particular, I’m impressed by the Cell Danger Response work of Dr. Naviaux and the work on the itaconate shunt (aka “itaconate trap”) hypothesis from Dr. Robert Phair, et al.
Over the last several years (with myself as both scientist and guinea pig) I’ve been looking for naturally occurring nutraceuticals and/or drugs available OTC that inhibit purinergic receptors, on the premise that excess purinergic receptor activity (triggered by excessive extracellular ATP) is the major driver of the Cell Danger Response, which Dr. Naviaux posits is the likely underlying mechanism that establishes ME/CFS, long Covid, etc. as intractable, chronic illnesses.
More recently I’ve learned about the itaconate shunt hypothesis, which suggests a specific mechanism by which cellular energy production is systematically down-regulated in the Krebs cycle and which might be restored again with drugs or nutraceuticals that inhibit the enzyme that (mis)converts Krebs cycle cis-aconitate to itaconate and thereby shunts the metabolic cascade away from the Krebs cycle and reduces energy output.
I have identified a number of naturally occurring nutraceuticals that inhibit various of the purinergic signaling receptors and have experimented with several. (Most of them are not well absorbed and do not cross cell membranes and reach the relevant receptors in the mitochondria, so delivery systems are also an important issue.)
So far I’ve been able to experiment with two that selectively inhibit the P2X7 receptor, which is considered the most important of the P2X and P2Y receptors in the Cell Danger Response and I’ve had significant positive results from both. However, based on that experience, I believe what is really needed to effectively turn off the Cell Danger Response is a formulation that addresses as many of the receptors as possible. (That, btw, is why there was excitement about the potential for suramin to help resolve the Cell Danger Response, because suramin is a broad spectrum P2X/P2Y receptor inhibitor.)
And I’ve had some success in my kitchen laboratory developing a functional food that provides increased amounts of citraconate. Citraconate is one of four potential drugs/nutraceuticals being discussed by the researchers that inhibits the dysfunctional Krebs cycle enzyme (ACOD1) and can potentially help turn off the itaconate shunt metabolic defect. The other three are powerful drugs and not readily available for testing, but citraconate naturally occurs in the crusts of bread that is baked at high temperature, so it is possible to develop a therapeutic food that provides increased amounts of citraconate from a natural source.
I’ve had a very interesting experience with this functional food. My body temperature has risen by as much as a full degree and has stabilized closer to a baseline of 98.6 after running lower for many years. I think it’s clear that there has been a change in my cellular metabolism at the basis of that change in body temperature. Not only does it show on a thermometer, I can feel more heat in my breath as I exhale air through my nostrils, my eyeballs feel noticeably warm and I generally feel warmer.
This is all a work in progress. I’m hoping eventually that the Cell Danger Response will resolve, as Dr. Naviaux hypothesizes it may, when I’ve been able to address a broader spectrum of the purinergic receptors, provide nutraceutical support for the Krebs cycle to shift back out of the itaconate shunt dysfunctional pathway, and continue to address the various factors on a more manifest/superficial level (hormone balance, inflammation, nutrition, stress, sleep, etc.).
I believe it is likely all these will need to be attended to in many cases, and there will not be a single “solution” for ME/CFS, long Covid, etc. (That is why I referred to Dr. Naviaux’s work on the Cell Danger Response as a “semi”-exception to my skepticism about finding a single “answer” to ME/CFS. I believe the Cell Danger Response does offer a plausible conceptual “answer” to what is going on with ME/CFS, but based on my own personal experience, I believe for an intervention addressing the Cell Danger Response to work on a practical level it will need as many of the multiple interconnected factors to be addressed simultaneously as possible.
Does that make sense?
Thank you Jerry.
I found your post very interesting.
I would add to the “multifactorial” list — in addition to hormone balance, inflammation, nutrition, stress, sleep, etc. I would add glucose metabolism (insulin resistance/elevated blood sugar) and neurotransmitter balance (in my case I tend toward inadequate dopamine, which I have considerable success managing with the help of a brilliant psychiatrist). And I would mention, dosage is highly individual. I take 10 mg/day of bupropion (typical conventional daily dose is 150 mg) and 0.25 mg/day of Abilify (typical lowest dosage is 2 mg/day) for neurotransmitter support and 0.026 mg/day orally of the GLP1 drug semaglutide (equivalent to 0.182 mg/week; typical dosage is 7 mg per week) to support insulin/glucose metabolism.
Other hormones, nutritional supplements, etc. I take at conventional dosages. I am hopeful this will become less complicated if/when I have more success finding ways to work with nutraceuticals that inhibit multiple purinergic receptors to more decisively address the underlying mechanics of the Cell Danger Response.
Good to know Jerry.Thank you for going to the trouble.I wish you ,Cort & all at Health Rising a happy Easter break.
Very interesting.
I am interested in your thoughts on pregnenolone. This is a precursor to other hormones, and is a neurosteroid so can work on the brain / CNS.
We ordered some from overseas but the shipping timeline is very long. So will have to be patient and wait for its arrival before trying.
I like pregnenolone, have taken it for years at 100 mg/day. You can order it cheaply from Vitacost.com.
I especially find it helps with memory and cognition (brain fog has been a frequent feature of my ME/CFS, but fortunately it’s well under control most of the time). As you say, pregnenolone is a neurosteroid that works in the brain, in addition to its role as THE precursor for all steroid hormones.
Thanks for the reply. Do you find it helps mental fatigue at all?
I would say it does. I think what I’m calling brain fog could just as accurately be called mental fatigue. I find several things help with the mental fatigue/brain fog in my case:
1. Supporting adequate dopamine function in the brain chemistry. There are several avenues that I’m working with in my own case. This has been such a central feature in my ME/CFS, I’ve had to give it a lot of attention over the years.
2. HORMONES (in my case, hydrocortisone to address my adrenal insufficiency and testosterone presently and thyroid previously during much of the 30 years I’ve had ME/CFS), which not only support energy, metabolism, etc., but they interact with and strongly support a robust brain chemistry, affecting mood, motivation, memory and cognition in a major way.
3. Food and environmental sensitivities, which can trigger/exacerbate ME/CFS symptoms including brain fog/mental fatigue. Doris Rapp, MD, a leading environmental doctor we mentored with when I was a medical practice office manager in the 1990s used the phrase, “allergy tension fatigue syndrome” in much of her writing. That was before Chronic Fatigue Syndrome was a recognized diagnosis.
4. Supplements of various kinds that support brain function. Generally these are referred to as “nootropics.” Another example in addition to pregnenolone would be Ginkgo biloba, which many people find helps a lot. (Like many herbs and herbal extracts, it has blood thinning effects, so it may be contraindicated for people on blood thinning medication.)
Dopamine is interesting. I have always suspected it plays a part. The NIH study led by Nath found lower levels if I recall.
I think the benefits quite a few people get from nicotine are likely to relate to its effects on dopamine.
My hunch has been that inflammation in ME/CFS plays a key role in terms of dopamine.
Mucuna pruriens has been on my list of things to try
I had not known of Macuna pruriens. Very interesting herb. I would try it myself but at the moment, things are going so well with my dopamine situation I don’t have a reason to tinker with what I’m doing. I will keep it in mind, however.
I’ve found that various things affecting dopamine have different mechanisms of action, which affects the way they work or don’t work in my system.
For example, stimulants, e.g., modafinil, Ritalin, caffeine, etc. provide temporary improvement but then I crash into exhaustion and depression. Nonetheless, many ME/CFS patients do report benefit from various dopaminergic stimulants.
MAO inhibitors (especially the herb Banisteriopsis caapi, which I have tried, and I suspect the same will be true with other, milder MAO inhibitor herbs like Saint John’s wort) also produce a transient benefit and then a crash.
I’ve had success with medicines that have more complex dopanergic mechanisms of action and thereby have a long-term beneficial effect without a crash, specifically Abilify (at 0.25 mg/day = 1/8 of a 2 mg tablet) and I’ve found that testosterone boosts dopamine better than any other thing I do.
Definitely seems naive to presume 1 answer! I agree it’s frustrating to be treated using the let’s throw a bunch of spaghetti against the wall and see what sticks approach without being able to get an understanding of how my mitochondria, endothelial cells, immune system, and gut are responding!! The approach seems very crude.
Could it possibly be the difference of whether the participants are in PEM or not at the time of the study? Or perhaps their severity? What was the difference in methodology?
That’s one possibility. The blood from the present study was gathered in a less stressful way (I can’t remember how). The first group was likely more severe as well but when the present study assessed severity they didn’t find that the more severe patients had worse mitochondrial results.
I agree that nicotine’s benefit for some ME/CFS patients has to do with it’s effects on dopamine. It powerfully increases dopamine and also acetylcholine. Here’s what Google AI says about acetylcholine:
“Acetylcholine (ACh) is a vital neurotransmitter that enables muscle contraction, voluntary movement, and autonomic functions like digestion and heart rate regulation. In the brain, it plays a key role in memory, attention, and learning. ACh is used medically to treat Alzheimer’s and neurodegenerative disorders, while low levels are linked to memory impairment, dementia, and muscle disorders.”
My experience with a trial of extremely low dose nicotine was, I felt like I was 100% cured, had the best day I’d had in years and then crashed spectacularly. I reported this to my psychiatrist and we did trials of two different acetylcholinesterase inhibitors (Aricept and Mestinon/pyridostigmine. Mestinon/pyridostigmine is producing promising results for many ME/CFS patients and is the subject of important ongoing research. Acetylcholinesterase inhibitors increase circulating acetylcholine by inhibiting the enzyme that breaks down acetylcholine molecules.)
Experimenting with various dosages and timings, including extended release, I couldn’t get either of the acetylcholinesterase inhibitors to work and concluded that the major neurotransmitter I need to target is dopamine, not acetylcholine.
This was meant to reply to Matthias’s comment but somehow it ended up under a different string of comments:
Matthias wrote:
“Dopamine is interesting. I have always suspected it plays a part. The NIH study led by Nath found lower levels if I recall. I think the benefits quite a few people get from nicotine are likely to relate to its effects on dopamine. My hunch has been that inflammation in ME/CFS plays a key role in terms of dopamine.”
Important study and message indeed.
There are two things to keep in mind when we talk about the endothelium being possibly vulnerable to “some factor in the blood”:
1
The “surface tissues” of the body (endothelium and mucous membranes) are the home base of many endogenous viruses – waiting for their chance to replicate whenever immune surveillance weakens (potentially: from oxidative stress or other damaging exposures after exertion). If viral reactivation starts (even if abortive), endothelial cell function may suffer with a multitude of consequences, e.g. disturbed coagulation, disturbed blood flow, disturbed vascular matrix, disturbed local immune responses etc.
2
But there is more to the endothelium than just “lining blood vessels”. The endothelium also constitutes the “window to the brain”. This is because the chorioid plexi (there are 4 of them) are basically convoluted assemblies or sponges of endothelial cells with a huge surface area. These plexi have direct (i.e. blood-brain-barrier free) contact with cerebrospinal fluid and communicate freely with the the socalled “circumventricular organs” (CVOs). These brain nuclei have important roles in body fluid regulation, cardiovascular functions, immune responses and autonomous regulation ((for a summary see: https://en.wikipedia.org/wiki/Choroid_plexus )). These nuclei not only consitute relay stations for communication between the central nervous system and the periphery, they are also functionally connected to brainstem centers involved in the stress response (like the noradrenergic networks of the locus coeruleus). Interestingly, the chorioid plexus was recently shown to be enlarged in Long Covid.
This means that the observed ability of “some factor in the blood” to challenge the functioning of endothelial cells is indeed a big thing which can have a far reach into many other tissues and, possibly, the brain.
It is a good idea to pursue this further. What I am missing so far in these experiments is the assessment of the viral genome in challenged endothelial cells or at least measurement of the dUTPases for a start (researchers may team up with Eurenia Ariza who has a ton of expertise here).
We currently focus very much on the mitochondrial changes – which is a good thing but we should not forget that these visible changes could also be but a bystander phenomenon indicating a generally stressed cellular milieu (if the mitochondrial “shrinkage” was clinically relevant in and of itself one would certainly expect to observe this phenomenon not only in female patients (see Prusty/Scheibenbogens work) but also in male patients – after all, males do have the same symptoms in need of explanation as the females do 😉
As always thanks for significantly contributing to the blog 🙂 Shungu found problems in the CVO’s if I remember rightly and a small study found an exquisite connection between vascular problems and neuroinflammation in long COVID. Here’s from the blog (which I had completely forgotten about).
https://www.healthrising.org/blog/2023/12/20/blood-vessel-neuroinflammation-long-covid/
One of the authors, VanElzakker will be part of a RECOVER panel on neurocognitive issues in long COVID coming up.
Thank you, Cort. A japanese researcher has even presented a whole hypothesis around the role of the CVOs:
https://www.jstage.jst.go.jp/article/ans/56/1/56_1/_article/-char/ja/
The CVOs indeed allow dynamic immune interactions between the periphery and the CNS, notably upon stress and other challenges. In this context it may be of interest that “distressed glial cells can allow extravasation of peripheral immune cells, complement proteins and aAB from the bloodstream into the parenchyma of the CNS (Watkins et al., 2007), thereby allowing aAB access to neuroantigens including β2-adrenergic and muscarinic acetylcholine receptors. This process, which was shown to last for several days after initiation, is now discussed as a central pathomechanism in Complex Regional Pain Syndrome (CRPS), a disorder that clinically overlaps with ME/CFS (Cooper and Clark, 2013)” (from our review paper on the role of neuroglia ((https://pubmed.ncbi.nlm.nih.gov/35614970/)).
For me this is interesting because we need to integrate what we now know (or suspect) about the role of the noradrenergic system (locus coeruleus and its networks) in ME/CFS. This brings the question into focus how peripheral phenomena and central phenomena may be connected. The CVOs clearly are a wide open window to the brain.
Weder bin ich Medizinerin, noch verbindet sich mein Gehirn mit der Schulmedizin und deren Terminologie. Dies nur als Entschädigung meines unprofessionellen Kommentares.
Ich habe me/cfs und bin seit zwei Jahren ans Haus gebunden.
In schweren Episoden oder als deren Ankündigung erinnern mich meine Arme, Beine, selbst Gesicht mit plötzlich überdeutlich blauen Adern ans Amazonasgebiet, wie blaue Flüsse…
Nie wurde das beachtet es hieß, bei manchen sei es so, oder -sehr charmant- das kommt mit fortschreitendem Alter. Aber wenn es mir besser geht, das sind Adern, rote Punkte, eingebaute Flecken weg. Daher macht es mich aufmerksam, das hier immer wieder von Blutgefäßen etc. die Rede ist, wenn auch für mich oft unverständlich.
Dankeschön, dass hier Forschungen zusammen getragen werden.
Google Translate
“Neither am I a medical professional, nor does my brain connect with conventional medicine and its terminology. This is just as compensation for my unprofessional comment. I have ME/CFS and have been housebound for two years. In severe episodes or as their warning, my arms, legs, even my face remind me of the Amazon region with suddenly very pronounced blue veins, like blue rivers… This was never noticed; it was said that for some people it is like that, or—very charmingly—that comes with advancing age. But when I feel better, the veins, red spots, built-in patches disappear. Therefore, it catches my attention that blood vessels, etc., are repeatedly mentioned here, even if often incomprehensible to me. Thank you for compiling research here.”
Fascinating! I asked ChatGPT Pro about this. It replied:
Common systemic reasons include:
connective-tissue laxity that may allow more venous distention during orthostatic stress,
or generalized vasodilation/flushing.
What matters most is the pattern:
More visible when standing, sitting upright, after heat, showering, exertion, or during a crash; better lying down → more consistent with dysautonomia/venous pooling.
Persistently visible all the time, even lying down, especially if there has been weight loss or skin thinning → more likely a body-composition/skin explanation.
Face + neck/chest veins, swelling, shortness of breath, cough, headache/fullness, worse bending over or lying down → that is more concerning for upper-body venous congestion/obstruction and should not be written off as ME/CFS.
A useful bedside clue is whether the veins fade substantially after lying flat for 10–20 minutes. If they do, that pushes the explanation more toward orthostatic venous pooling than a fixed structural problem. That last point is an inference from the orthostatic-pooling physiology rather than a direct test standard.
It is sad that this “something in the blood” finding wasn’t able to be replicated.
However, I found it encouraging that the Dr. Audrey Ryback Replication was a real replication.
It used the same method (Seahorse), it used the Canadian Consensus Criteria – which ensured that each ME/CFS patient was a ME/CFS patient. It reduced batch effects.
Although the finding wasn’t what we wanted, Dr. Audrey Ryback and Dr. Chris Ponting’s team were rigorous in their replication method. Thank you so much for your scientific rigour.
This is what we need for ME/CFS replication studies.
So often ME/CFS replication studies are not true attempts to replicate. The studies will use ME/CFS definitions where PEM is not mandatory, where therefore, the data is corrupted at the start because it mixes in Non-ME/CFS patients with ME/CFS patients. They will call it a replication, then ignore the method that was used.
So replication studies that are done with what is actually normal scientific rigour are so very welcome here – no matter what the results are.
It feels like a loss in some ways, but because science held fast, it’s a win.
I think it is really rare that a group explicitly tries to replicate a finding! And, I agree – good for them and they picked a good one to try. If it had panned out that would have really been something! As it is, it closes one door but points to others – and thankfully, there are plenty of other doors. 🙂
BUT WHICH STUDY IS RIGHT? THE ONE THAT FOUND SOMETHING OR THE ONE THAT DIDN’T. WHAT MAKES THE SECOND STUDY BETTER THAN THE FIRST?
What strikes me reading this is how it might connect to something many of us experience that doesn’t fit a “mitochondrial/energy” model very well: sensory overload triggering PEM.
In my case, environments like big box stores (bright lights, motion, noise, constant peripheral stimulation) can reliably trigger a crash, even without meaningful physical exertion. The response is systemic (gut, glands, brain fog), not just “fatigue.”
By contrast, a slow, well-paced walk without that kind of external sensory load does not produce the same level of PEM for me. That makes it difficult to frame this as a muscle energy problem and seems more consistent with a central regulation issue, which is where the CVO idea becomes interesting.
I’m in the mild/moderated band – funerals wipe me out for days afterwards, and not just the tragic ones but the “long life well lived” ones as well. Too much small talk with people you haven’t seen in a long time. Busy, noisy cafes, restaurants, birthdays etc – same thing.
SORRY ABOUT ALL CAPS, WRIST STILL IN BRACE.
I READ THE ACTUAL STUDY THAT IS THE SUBJECT OF THIS BLOG. IT WAS FUNDED BY AN ME FOUNDATION. THE STUDY’S AUTHORS SEEM TO USE ME/CFS AND ME INTERCHANGEABLY IN THE PAPER.
‘While often used interchangeably as “ME/CFS,” Myalgic Encephalomyelitis (ME) and Chronic Fatigue Syndrome (CFS) are not always considered identical, though they share key symptoms. ME often refers to a more severe neurological condition, while CFS has historically been used to describe a broader range of fatigue-related illnesses, leading to debate over whether they are the same disease or distinct subgroups.
Myalgic Encephalomyelitis (ME) was officially named in 1955 following an outbreak at London’s Royal Free Hospital, though recognized outbreaks of the disease date back to at least 1934.’
ALSO, THE CURRENT STUDY INVOLVED SELF-SELECTED PARTICIPANTS WITH SELF-REPORTED SYMPTOMS THAT AS FAR AS I COULD TELL WEREN’T VERIFIED WITH MEDICAL RECORDS,
BETTY…..and anyone else….check out the documentary
” the heart revolution”
Also the heart math institute.they have been doing research about the heart fir 30+ years.
Its all getting so very interesting.
Have read the gist. So, did the study find an effect on mitochondria in no patients at all? Or did they find no significant effect on statistical average, but an effect showed up in some patients meaning there could be a subgroup?
Mast cells are one of the most plausible sources of the circulating factors discussed in this article. MCAS causes all sorts of problems with endothelial cells and blood flow, including up regulating the SNS and norepinephrine, causing vasoconstriction and, voila, blood flow problems.
I wonder, what the cell cultures would look like after a month, – or perhaps even years from now and how different their function would be by then.