


Geoff’s Narration
The GIST
“For me, the risk is small and the (potential) benefit is huge.” Dr. Kaufman
We’re back, focusing on GLP-1-enhancing drugs. Why another GLP-1 blog? Because new information keeps pouring out. Plus, these surprise drugs constitute perhaps the most exciting treatment possibility ever seen in ME/CFS, FM, long COVID, and related diseases. They appear to have engaged the complex, chronic illness experts like no others.

Suddenly, a new treatment possibility showed up.
In fact, these drugs have pretty much wowed the medical world. Created to combat obesity and diabetes, GLP-1 agonists are now being assessed in dozens of disorders. Besides maintaining blood sugar or losing weight, they are able to affect our metabolic, cardiovascular, and even neuroinflammatory systems.
This blog covers a recent Renegade Research Roundtable, two studies reporting on the effects of GLP-1 agonists on people with mast cell activation syndrome (MCAS) and intracranial hypertension, and two major GLP-1 long-COVID trials getting underway.

The Renegade Research Roundtable
Suddenly, a new treatment possibility showed up.
THE GIST
- We’re back, focusing on GLP-1-enhancing drugs. Why another GLP-1 blog? Because new information keeps pouring out. Plus, these surprise drugs constitute perhaps the most exciting treatment possibility ever seen in ME/CFS, FM, long COVID, and related diseases. They appear to have engaged the complex, chronic illness experts like no others.
- In fact, these drugs have pretty much wowed the medical world. Created to combat obesity and diabetes, GLP-1 agonists are now being assessed in dozens of disorders. Besides maintaining blood sugar or losing weight, they are able to affect our metabolic, cardiovascular, and even neuroinflammatory systems.
- This blog covers a recent Renegade Research Roundtable, two studies reporting on the effects of GLP-1 agonists on people with mast cell activation syndrome (MCAS) and intracranial hypertension, and two major GLP-1 long-COVID trials getting underway.
- Dr. Dempsey described how a woman with a traumatic brain injury (TBI) and a woman with postural orthostatic tachycardia (POTS) responded. After being put on the full dose (2.5mg) the TBI patient experienced nausea but persevered and found that 2-3 hours after taking the drug her brain fog completely disappeared and she was could focus and work like before. A POTS patient who needed to take 2-3 times more time to get her college work done, reported she no longer had brain fog and was able to do her work in a third of the time.
- With side effects not usually a problem at low doses and improvements often seen, Dr. Dempsey and Dr. Kaufman are using these drugs very early in their patients’ treatment. Dr. Kaufman said he was particularly considering doing so in his more severely patients. Dr. Dempsey said, “It was pretty mind-boggling to see the response and the fact that it was global, it was systemic, and pretty quick”.
- Dr. Dempsey also noted that the drug doesn’t work on all patients and that some patients cannot tolerate even the small doses being used. She does not consider these drugs cure-alls and advises that everyone “should go down this path cautiously”.
- Dr. Kaufman’s biggest concern with increasing the dose and producing side effects is not weight loss but gut motility. On the other hand, Dr. Dempsey reported that many of her patients with gut motility issues are doing well on the low doses of the drug being used, and a mast cell paper reported that reductions in nausea were common.
- Kaufman believes that by reducing systemic inflammation, GLP-1 agonists are targeting one of the root causes of these diseases and helping fight reactivated pathogens such as EBV.
- Dr. Dempsey believes the drug binds to mast cell receptors and blocks the release of inflammatory mediators. A recent explored the effects GLP-1 agonists had on a case series of 47 patients with mast cell activation syndrome (MCAS).
- The paper reported on “the remarkably high rate of favorable responses we have seen from ad hoc use of such drugs in the cases presented here of MCAS“. It stated that “overall clinical benefit” was found in 89% of patients.
- The six case reports in the paper demonstrated the wide range of effects these drugs can have. Some case reports involved MCAS patients who took the standard dose to lose weight and experienced other kinds of relief. Others included MCAS patients who benefited from low doses of the drug. (See the blog.)
- A systematic review found that these drugs might be helpful in intracranial hypertension, a condition that appears to be widespread in these diseases. One small study, found they were associated with significantly reduced pain, fatigue, and opioid dependency in fibromyalgia (FM).
- In my experience, the biggest problem facing patients is how to use the drug. Three possibilities exist: compounded drugs, vials, and autopens. All present issues.
- Because as of early 2025, semaglutide and tirzepatide were being removed from the shortage list, they are no longer legally available to be compounded. While some compounding pharmacies may still carry them, most patients will have to rely on autopen devices, which provide higher doses than typically used in ME/CFS, or vials.
- Because the autopens have internal mechanisms that control both the plunger travel distance and injection volume, it’s not possible to accurately give yourself a half or a quarter, etc. dose.
- Autopens containing semaglutide (Ozempic, Wegovy) can deliver lower doses (0.25/0.5 mg), but note this is the starting dose for type II diabetes; i.e. it’s probably every bit as powerful as the 2.5mg dose of Mounjaro.
- Some countries, like Australia, have Mounjaro (the doctor’s first choice) pens, which allow you to determine how much of the drug to use. The lowest Mounjaro autopen dose available in the US, though, is a whopping 2.5 mg.
- Lily Pharmaceuticals also offers vials that allow a syringe to draw low doses. It’s not clear how long they will last. It’s also possible to use an insulin syringe to draw the drug out of some autopens.
- Some compounding pharmacies may still offer the drugs. Patients should be careful that they are translating the units correctly as some people have injected themselves with too high concentrations of the drug. (See the blog.)
- The NIH’s RECOVER Initiative for long COVID demonstrated great initiative by using patient and physician reports to initiate a GLP-1 agonist. Dr. Kaufman reported that after embracing doctors’ and patients’ reports and launching the trial, RECOVER will be using far higher doses (0.1-.25mg vs 2.5 mg) in their long-COVID trial. A 1,000-person Scripps long COVID trial is doing the same.
- With regard to RECOVER, this is apparently because “trials funded by NIH must use doses that have an established toxicology and pharmacokinetic profile already accepted by FDA”.
- Dr. Kaufman noted that it’s possible that starting at 2.5mg might work – it’s just that no one has tried. (The mast cell paper mentioned several obese patients who tolerated the standard dose quite well.) Still, it’s a big risk as Dr. Kaufman worried that so many patients will drop out that the drug will be considered a failure.
- The Scripps fully remote Long COVID Treatment or LoCITT (“Lock-it”) trial has a lot going for it. Anyone in the US can participate in the year-long study; no in-person visits are required, symptom and activity trackers and smart scales will be used, and a few people will provide blood for labs. Check out if you’re eligible for the trial here, and check out a webinar on the study in the blog.
- However, the GLP-1 saga turns out, the fact that these drugs have popped up seemingly out of nowhere, and have generated such excitement, highlights the potential existing in the huge repurposed drug (drugs used in another condition than for which they are approved) market for these diseases. Looking at this new class of drugs, nobody thought – oh, man – we’ve got to try these drugs out in ME/CFS/long COVID or fibromyalgia – and yet here we are. More and perhaps better GLP-agonists are on the way.
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit
Renegade Research Roundtable
Dr. Dempsey described the experiences of two very different patients with extraordinary improvements in brain fog and cognitive functioning, as well as other symptoms.
Traumatic Brain Injury – In the Renegade Research Roundtable, Dr. Dempsey described what happened with a long-term, difficult-to-treat patient she’d been treating for about 20 years.
She was a 40-year-old woman who was left with a traumatic brain injury after a car accident in her twenties. (Traumatic brain injuries often produce symptoms similar to those found in ME/CFS/FM and long COVID.) Her case was complicated by a history of infections (Bartonella), and she had particular problems with word finding and brain fog.
Over time, she had gained weight and used the drug to address that. After being put on the full dose (2.5mg), she experienced nausea but persevered and found that 2-3 hours after taking the drug, her brain fog completely disappeared and she could focus and work like before. While she never lost much weight, she was so happy with the results that she didn’t care.
Postural Orthostatic Tachycardia Syndrome (POTS) – A POTS patient who needed to take 2-3 x’s more time to do her college work, reported she no longer had brain fog and was able to do her work in a third of the time. Her improved numbers on the NASA lean test suggested her brain was getting more blood flows. Noting the drug’s anti-inflammatory effects, Dr. Dempsey suggested it may be reducing neuroinflammation.
Doctors Move These Drugs To the Top of the List

A new treatment possibility is causing some doctors to use it early and often.
ME/CFS/FM and long-COVID doctors are inherently conservative – not in the range of treatments they use – but in how they use them. They tend to introduce them slowly so as not to spark a bad reaction. At least for these two doctors, the trial period appears to be over. They are introducing them early in their protocols.
Dr. Dempsey said, “It was pretty mind-boggling to see the response and the fact that it was global, it was systemic, and pretty quick”. She, like Dr. Kaufman, has moved GLP-1 agonists way up on her protocol. Both are considering using it very early with their patients. Why, Dr. Kaufman said, make the patient wait, particularly since at very low doses, side-effects are usually not a problem?
In good news, for more severely ill patients who can tolerate little, side effects don’t appear to be much of a problem. When asked if the drug was suitable for mostly bed or housebound patients, Dr. Kaufman gave what has become a rather familiar answer, and which shows what a core part of his treatment regimen, tirzepitide (Mounjaro) has become.
If he’d been asked that question 8 months ago, he would have waited 3, 4, 5, 6 or months to see if other treatments worked. Not anymore – particularly in more severe patients – he’s ready to try to the drug sooner. He believes GLP-1 agonists should “be tried sooner rather than later”. Referring to the risk/benefit analysis that all doctors do with their patients, he’s found that the potential risk is small and the potential benefit is huge.
He’s had a similar experience with mast cell treatments. Before he would have started with an antihistamine and two receptor blockers like Zyrtec and Pepsid. If that didn’t work he would add a flavonoid, then a mast cell stabilizer, etc. Now, if he has a good reason to think a drug like Cromolyn would work faster, he’s just going for it.
Dr. Dempsey also noted that the drug doesn’t work on all patients and that some patients cannot tolerate even the small doses being used. Everyone “should go down this path cautiously”.
Gut Tweaker / Gut Enhancer?
Dr. Kaufman’s biggest concern with increasing the dose and producing side effects is not weight loss but gut motility – a common problem. The MCAS paper suggested that “MCAS-targeting ‘rescue’ therapy” (e.g., extra doses of H1/H2 receptor blockers) can help.
On the other hand, Dr. Dempsey reported that many of her patients with gut motility issues are doing fine on the low doses of the drug being used, and the mast cell paper reported that “9 of 14 of the patients in its case series with baseline nausea experienced reduced nausea after taking the drug”. Indeed, GLP-1 agonists appear to be helpful for gastrointestinal diseases such as IBS, ulcerative colitis, and Crohn’s disease.
Systemic Inflammation Reducer?
Kaufman believes that by reducing systemic inflammation, the GLP-1 agonists are getting at one of the root causes of these diseases. (GLP-1 agonists appear to be helpful in a wide variety of inflammatory diseases and have been found to effect multiple immune pathways including tumor necrosis factor alpha (TNF-α) and nuclear factor kappa beta (NF-κβ) inhibition and NLRP3 inflammasome and IL-1B suppression.) While he doesn’t have proof of it, he believes the inflammation reduction is allowing the immune system to recover and keep the infections under control.
Dr. Kaufman believes reducing inflammation may be allowing the immune system to recover – enabling it to now fight off pathogens.
Dr. Malcolm chimed in, stating that he has quite a few patients who got sick hiking abroad and we have no idea what kinds of infections they have picked up. Malcolm noted that David Putrino recently talked about the incidence of bartonella infection in long COVID.
Dr. Kaufman focused on the immune system. He noted that EBV probably reactivated in most people with COVID-19, but that only about 10% went on to develop long COVID. Instead of focusing only on bringing EBV or Lyme or whatever it is that got reactivated down, Kaufman asserted that finding ways to get the immune system up to speed is probably more fruitful in the long run. Once the immune system is in shape, it can keep the bug locked down.
By increasing autophagy and decreasing inflammation, he believes that rapamycin is doing something similar. Studies have shown that rapamycin improves immune functioning and reduces the incidence of infection. (A rapamycin blog is coming up.)
Mast Cell Blockers
Dr. Dempsey believes the drug binds to mast cell receptors and blocks the release of inflammatory mediators. She was a co-author on a recent paper, “Utility of glucagon-like-peptide-1-receptor agonists in mast cell activation syndrome”, which explored the effects GLP-1 agonists had on a case series of 47 patients with mast cell activation syndrome (MCAS).
The doctors reported on “the remarkably high rate of favorable responses we have seen from ad hoc use of such drugs in the cases presented here of MCAS” and stated that “overall clinical benefit” was found in 89% of patients. They asserted that the “the high clinical benefit rate from GLP-1RA therapy in our series raises a clarion call for rigorous, systematic investigation to define what the appropriate roles for such treatments in MCAS actually will be.”
Mast Cell Case Reports
Dr. Dempsey and Dr. Kaufman believe the drug may be blocking mast cells from activating (gold – mast cell; blue – histamine).
The case reports provided suggested these drugs can produce a wide range of benefits. Several of these cases involved people with MCAS who were taking the drugs for obesity at the standard dose. While dramatic improvements were reported, some symptoms tended to remain. Interestingly, the obese MCAS patients tolerated the high dose quite well, while others did fine on lower doses.
- A 24-year-old with chronic inflammatory problems since infancy, who had tried many treatments, found that within hours of taking .25mg, his hunger and blood pressure had normalized, and his fatigue, brain fog, and inflammatory issues were substantially reduced. Every increase in dose brought improvements and he settled in a .75mg.
- A 42-year-old female with longstanding profound fatigue, chronic pain, asthma, multiple food intolerances, GI symptoms including diarrhea, urticaria, food cravings, weight gain, and migraine who was essentially housebound due to constant exhaustion (she estimated 30% of normal energy) took tirzepitide at 3.75 mg principally to address obesity. Within days of the first dose, she gained great improvements in essentially all symptoms and was no longer housebound. Dosing was later increased to 5mg, each time with additional improvement and only transient mild nausea with the initial dosing.
- A 41-year-old woman with brain fog, insomnia, vertigo, neuropathic symptoms, blood pressure lability, postural orthostatic tachycardia syndrome (POTS), dermatographism, macular erythematous rash, flushing, burning skin, severe gastroesophageal reflux, migratory joint pains, vaginal pruritus, intermittent hoarseness, and chemical sensitivity. Within hours of the first dose, all troublesome symptoms had substantially improved or resolved.
- A 50-year-old obese woman with dysautonomia, unexplained dyspnea at rest, orthostatic dizziness, fatigue, brain fog, acid reflux, nausea, POTS, hypermobility and headache of post-viral onset. Tirzepitide 2.5mg to address her weight gain was increased to 5mg once weekly, resulting in at least 65–70% improvement in her symptoms, including fatigue and cognitive impairment. She felt she was being productive for the first time in years.
- A 63-year-old female with allergic and asthmatic symptoms since childhood, fibroids, Hashimoto’s thyroiditis, experienced diffuse body aches and bone pain, insomnia, brain fog, bloating, food sensitivities, and a need to eat every 2–3 hours. She did not respond to mast cell treatments. Weekly tirzepitide shots immediately brought significant relief of pain, insomnia, and glycemic lability, but her symptoms reliably relapsed shortly before the next dosing. Dosing was changed to 2mg twice a week and all symptoms have been remained significantly improved.
- A 62-year-old woman with chronic health problems since the age of 10, who experienced anaphylactic attacks, fatigue, tinnitus, bone pain, itching, and nausea, and was largely housebound, tried semaglutide at 0.125 mg once a week. After her second, she started walking three miles per day, her anaphylaxis attacks improved, and her further pruritus, flushing, diarrhea, or post-prandial abdominal pain disappeared, and she regained tolerance for previously intolerable foods.
Blood Flow Enhancer?
GLP-1 agonists may be reducing brain fog by increasing blood flows.
Another person (unidentified) suggested that by decreasing inflammation around the capillaries, the GLP-1 agonists were increasing blood flows.
Dr. Kaufman believes that the fact that GLP-1 receptors are found all over the body explains why these drugs can have so many effects. Even though most of these drugs do not cross the blood-brain barrier, brain fog is often one of the first symptoms affected and may be due to improvements in blood flows.
Intracranial Pressure Reliever?
Dr. Dempsey reported that the GLP-1 agonist Zepbound removed the high intracranial pressure in one patient. Indeed, a recent systematic review found that “GLP-1 RA use was consistently associated with improvements in headache frequency, weight reduction, and reduced need for acetazolamide or surgical interventions. One small randomized controlled trial found that “exenatide significantly lowered ICP within hours”. Other studies have reported that papilledema (swelling of the optic disc in the eye due to increased intracranial hypertension’) was removed. Cognitive function either improved or remained stable. Mild gastrointestinal symptoms were the main side effect.
Because high intracranial pressure appears to be very common in these diseases, relieving it could be a big deal.
Fibromyalgia Anyone?
What about the mostly forgotten player in the complex, chronic disease (CCD) field – fibromyalgia (FM)? Except possibly for long COVID, more people have FM than any other CCD, yet we hear little about it. One small study, however, found that GLP-1 agonists were associated with significantly reduced pain, fatigue, and opioid dependency.
There’s also the osteoporosis factor. Studies indicate that people with FM are at increased risk for osteoporosis and while it’s early days, some studies suggest these drugs may be able to increase bone formation.
Using the Drug
Figuring out how to use drugs that are in available in much higher concentrations than the doctors use has been a challenge.
In my experience, the biggest problem facing patients is how to use the drug. I don’t know if these doctors realize how difficult it’s been for patients to find a way to use these drugs at the low concentrations they recommend. It would be great if someone would put out a sheet describing how these drugs are being used.
Three possibilities exist: compounded drugs, vials, and autopens. All present issues.
Five different GLP-1 agonists have been FDA-approved, and doctors have focused mainly on one – tirzepitide (Zepbound/Mounjaro). Others may be as effective. The dosing regimens for these drugs vary dramatically. For Type II diabetes, tirzepitide starts at 2.5mg injection weekly for four weeks and goes up from there. Semaglutide (Ozempic, Wegovy) starts at .25mg/week and then goes up from there. All the drug protocols feature a 4-week stabilization period and then titrating up after that.
Compounded formulations can be found here and there, but are now basically illegal – and hard to find. (When I asked ChatGPT to find compounding pharmacies that provide GLP-1 agonists, it could not produce any.) That means most patients will have to rely on autopen devices, which provide higher doses than typically used in ME/CFS, or vials.
Autopens
Autopens containing semaglutide (Ozempic, Wegovy) can deliver lower doses (0.25/0.5 mg), but note that this is the recommended starting dose for type II diabetes, so it’s probably every bit as powerful as Mounjaro’s 2.5mg starting dose.
Some countries, like Australia, have Mounjaro (the doctor’s first choice) pens, which allow you to determine how much of the drug to use. The lowest Mounjaro autopen dose available in the US, though, is a whopping 2.5mg. Because the autopens have internal mechanisms that control both the plunger travel distance and injection volume, it’s not possible to accurately give yourself a half or a quarter, etc. dose.
Why has Mounjaro been preferred? Because Mounjaro has one more GLP-1 receptor agonist than semiglutide (Ozempic, Zepbound) it may be more effective. It’s also simply the drug both doctors are most familiar with. Other GLP-1 agonists have been helpful, though.
Getting Really Low – The very low doses these doctors often start their patients off on (0.1mg) means either a compounding pharmacy needs to be found or insulin syringes are used to draw the drug from the pen or from a vial. (The insulin syringe technique will only work if the pen has a removable cap and rubber septum.
Figuring out the correct dose from an autopen to an insulin syringe is no easy task. I know of somebody who prepared an Excel spreadsheet in an attempt to figure it out and even then, they’re not sure if it’s correct. It appears to be far easier to buy a vial.
Lily Pharmaceuticals offers Zepbound/Mounjaro in vial form (5mg/ml, 10 mg/ml, 12.5 mg/ml)- allowing the use of syringes to fine-tune doses. According to ChatGPT this is the formula to determine the correct dose
Then, if you’re using a U-100 insulin syringe, you convert the mL’s to the units/lines on the syringe.
Units =
In other words, if you purchase a 10mg/ml bottle….
- .10 gm dose – If 1 mL=100 units, then a .10mg dose (0.10 / 10) × 100 = 1 unit. To get his lowest dose you would fill the insulin syringe to 1 unit or the first line on the syringe. You can see how low a dose this is. You couldn’t calculate a lower dose using a standard I mL syringe. (You can purchase smaller syringes).
- .25 mg dose – If 1 mL=100 units, that an .25 mg dose (0.25/10 x 100 = 2.5 units. You would draw up to 2½ units (about midway between the “2” and “3” marks).
Note, though, that depending on which vial of tirzepatide you purchase the calculation changes. ChatGPT created this table to show.
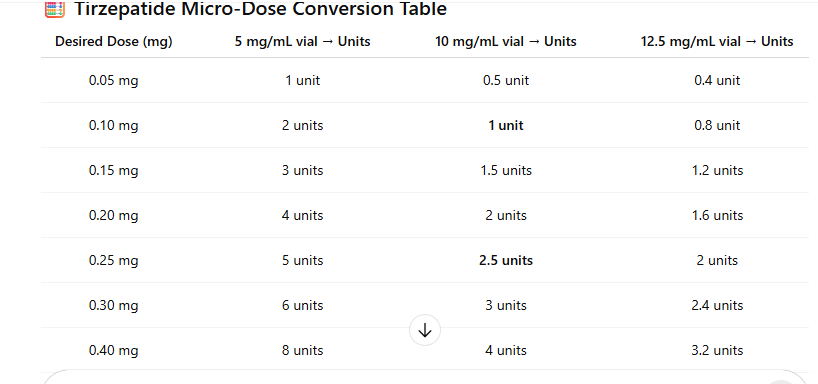
The vials should be refrigerated. I have been told that Lily states that the vials – which do not have a preservative – last for a month. Since a 10mg/ml vial contains 100 doses at the lowest dose (.10 mg) and 25 at the next lowest dose (.25 mg), it has far more of the drug than you could use in a month (1 dose a week). Some people are experimenting to see if the vials last longer.
PrecisionAI reported that prices in the US for vials are quite reasonable if you can get a good number of doses out of them.
-
5mg/0.5ml vial: Approximately $110–$141 per vial (or $1,000+ per box of four vials for U.S. retail pricing)
-
10mg/0.5ml vial: Approximately $150–$154 per vial
Compounded Forms
Using a low-dose compounded formulation is the most straightforward. Drug companies are cracking down on compounding pharmacies, but some apparently still provide the drug. (Diane reported that compounded drugs are “easily found legally in the US through many telehealth providers. Search Reddit: r/compoundedtirzepatide) (Because compounding pharmacies can legally produce drugs if the drug is not available, one would think compounding pharmacies might have an out, given that low-dose formulations of the drug are not available).
The biggest problem for Dr. Kaufman with the compounded medications is translating from milliliters to milligrams and/or units. Enough dosing errors have been reported with compounded GLP-1 injectables (mis-calculated concentrations, wrong syringes, unit mix-ups) that in 2024, the FDA published a warning. At times, patients have accidentally injected five to 20 times more than the intended dose of semaglutide (!). Note that “units” refer to the lines on the syringe; one line = one unit.
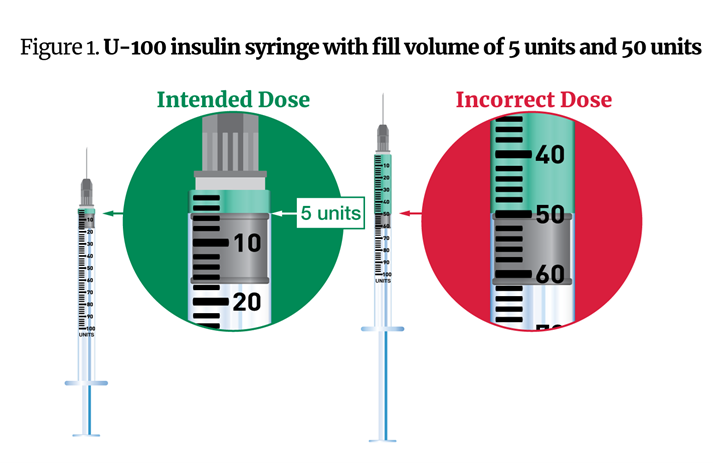
From the FDA report.
Instead of barely filling a U-100 (1 milliliter) insulin syringe to draw a 5-unit (0.05 milliliter) dose some people have injected half the syringe, producing vomiting and other side effects. The FDA stated that compounders should use a 503A-compounded, low-concentration sterile vial and syringes that reflects the prescribed amount; i.e., the prescription is listed in mg/ml, and the syringe gradations match the prescription.
A 10ml prescription should come with syringes that have 0.01ml gradations; i.e., it should come with a 1ml syringe which is broken up into tenths and hundredths of a ml. 1 ml insulin syringes are readily available on Amazon.
Large RECOVER and Scripps GLP-1 Agonist Long-COVID Studies Buck Expert’s Recommendations
The NIH’s RECOVER Initiative for long COVID demonstrated great initiative by using patient and physician reports to initiate a GLP-1 agonist. Dr. Kaufman reported that after embracing doctors’ and patients’ reports and launching the trial, RECOVER is not following ME/CFS and long-COVID doctors’ experience when it comes to running the trial.

Both the RECOVER and Scripps long COVID trials are using far higher doses than cautious ME/CFS/long COVID doctors do. Let’s hope it works!
RECOVER long COVID will be using a far higher starting dose (2.5 mg) than ME/CFS/long-COVID doctors are using. Not just a little higher. If my math is right, their starting dose is 10-25 times higher than the dose (0.1/.25mg-2.5mg) that doctors have starting their notoriously sensitive patients on.
Gut issues are a big concern with higher doses. A review of GLP-1 agonist studies using the standard dose in high intracranial pressure reported:
“Patients should be counseled about the high likelihood of nausea and GI upset (diarrhea, vomiting, and constipation, delayed gastric emptying) especially in the first 4–8 weeks of therapy. Slow titration of dose can help, as can dietary adjustments.”
The recent mast cell paper suggested:
“significantly lower doses of GLP-1RAs than presently used as starting doses for T2DM and obesity therapy might be sufficient, and even optimal, for MCAS. Such trials hopefully will also identify whether lower doses might thus reduce even further any risks from initial and/or long-term use of such drugs.”
Not the RECOVER or Scripps trials, though. Both appear to be placing all its bets on a very high dose (for this community). Why would they take such a risk? I asked ChatGPT 5.0.
ChatGPT reported that with regard to RECOVER that because “trials funded by NIH must use doses that have an established toxicology and pharmacokinetic profile already accepted by FDA”, RECOVER was in a bind. Even though lower doses are presumably safer, using them would still require a “new pre-IND safety justification, dose-range toxicology studies, and possibly a new manufacturing lot release.” That would add ~1–2 years of delay.
Dr. Kaufman noted that it’s possible that starting at 2.5mg might work – it’s just that no one has tried. (The mast cell paper mentioned several obese patients who tolerated the standard dose quite well. Plus a non-obese mast cell patient, who, due to a pharmacy error, got 2.0mg instead of .75mg, improved further.)
The just-announced 1,000-person Scripps LOCIT trial for long COVID is using the same dose. Dr. Kaufman’s fear is that both trials will fail because too many patients will suffer side effects and withdraw, and the drug will be forever lost to vast majority of long-COVID patients. Let’s hope that both RECOVER and Scripps groups have chosen well.
The Scripps LOCIT Trial
The Scripps fully remote Long COVID Treatment or LoCITT (“Lock-it”) trial has a lot going for it. Anyone in the US can participate in the year-long study; no in-person visits are required, symptom and activity trackers and smart scales will be used, and a few people will provide blood for labs.
Julia Moore Vogel, senior program director at the Scripps Research Translational Institute, noted that “LoCITT enables even patients with the most severe symptoms to join the search for answers.” Vogel, who has long COVID, and Eric Topol are co-principal investigators of the study.
Check out if you’re eligible for the trial here, and check out a webinar on the study.
More GLP-1 Drugs on the Way
No drug company wants to miss out on GLP-1 bonanza and more drugs are on the way. Orforglipron (oral GLP-1 – Eli Lilly) is expected to receive FDA approval over the next year. A triple agonist (Retatrutide (GLP-1 + GIP + glucagon) is expected in a couple of years, plus oral versions that could help with dosing are expected to come online over the next couple of years as well. At least four other candidates are in trials.
The Promise of Repurposed Drugs
However, the GLP-1 saga turns out, the fact that these drugs have popped up seemingly out of nowhere, and have generated such excitement, highlights the potential existing in the huge repurposed drug (drugs used in another condition than for which they are approved) market for these diseases. Looking at this new class of drugs, nobody thought – oh, man – we’ve got to try these drugs out in ME/CFS/long COVID or fibromyalgia – and yet here we are.
Other surprises surely await us.



I am skeptical. It just reeks of snake oil. The wide range of purported benefits for a wide range of disorders seems too good to be true.
But as always, I am very happy if my skepticism is ill founded and these drugs do work for many patients.
Curious if anyone has tried?
Ps. I really DO hope I am wrong.
I just want to see effective treatment
oh, AND the warning signs of a crash – inflammation in my throat – I haven’t had that since I started. So I’m guessing other inflammatory markers that were less obvious have also reduced. My friend isn’t restored to total good health, but there is a heap more she can do now.
More on Metformin September 11, 2025
A Perspective on the Role of Metformin in Treating Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and Long COVID
https://pubs.acs.org/doi/10.1021/acsptsci.5c00229
It has made all my symptoms worse and caused tinnitus. I even started at .05. insomnia, anxiety, tinnitus, massive increase in brain fog and fatigue. I was hoping it would go away but it’s been a month and isn’t better. I’m extremely disappointed. I might try to do just the .05 without going up again for a few weeks but this is ridiculous.
I did not do well on Metformin either. It made me very constipated which is the opposite you would expect. I went on to try Berberine which is almost the same thing and had the same problem. I was very disappointed.
was .05 tolerable for you if you stayed there?
yes but it did absolutely nothing. and then .1 put me in the ground. i’ve done all the extended micro tapers for all of my other medications and i could tell that this was not going to treat my fatigue. i don’t have any of the other co-morbidities.
Absolutely. I found an enormous surge in energy and wellbeing (without crashing), and a significant reduction in brainfog. (I barely qualified with a bmi of 31 with clothes on, lol, but so grateful I did). I told my friend who has more severe cfs than myself, and she too has had a significant improvement all round, though interestingly no weight loss (a good proportion of people do not respond with weight loss). I’m a former abc journalist, and have a Phd, all of which to say: I loathe health ‘woo’, am far from a snake oil type. This stuff is revolutionary.
My best advice is to start on a low low dose using advice from your region as to how to do so (in Australia it’s easier with the pen to ‘count clicks’ – google it). And to slowly slowly titrate your dose up – nowhere near as fast as the manufacturers suggest.
Hi Gretchen — also in Australia, is there somewhere (e.g., a social media site) where we can get details from other patients re accessing low doses here?
Hi Elinor,
I haven’t looked for one, but I have found Reddit to be enormously useful with ordinary people working out best use (believe it or not!).
But I can offer this regards dosing: in Australia you get a pen with 4 doses in it (actually 5 but that’s another story – search ‘golden dose’ and you can read about how to get that last dose out of the pen).
Each dose is 60 ‘clicks’ of the pen, regardless of whether it’s a 2.5ml pen, a 5 ml pen, etc. So you can work out the dose per click accordingly.
My friend for eg started on 1.25ml to minimise nausea which she hates. So she counted 30 clicks of the 2.5ml pen, and injected as instructed.
The drug cos will say the contents expire within a month of starting your pen. Most on reddit will say nonesense. Keep the pen refrigerated at all times, and if you start on 1.25 ml you’ll get 8 doses.
Unfortunately, unless you have a truly amazing doctor who might bend the rules for you, you won’t get anyone to prescribe it. But actually 30bmi (which is a bullshit measure but never mind that) isn’t all that overweight 😉
I mean, you won’t get anyone to prescribe it unless you’re classified as overweight, ie 30BMI+
HI what is the cost in AUS? Pls
It depends on the dose but you can google it and find out what you need to know.
In the UK it is extremely easy to get it from reputable online pharmacies with lower BMI. 25-27. Also, most don’t ask for evidence of BMI. Just self-reported. And usually a photo of yourself in form fitting clothing. Unless you are very thin you can get it. The Reddit Wegovy UK has people posting their money off codes weekly.
Hi Gretchen,
in your post: “I have found Reddit to be enormously useful “. I am a registered member but could nt find the section. Could you kindly give me the link or title to serch for it ? Thank you
Try this: https://www.reddit.com/r/antidietglp1/
And this: https://www.reddit.com/user/Vincent_Curry/ – Vincent mapped a few things about how he went on (and tapered off) a glp1. And I also find this useful: https://www.reddit.com/r/FatSciencePodcast/
You can search reddit for terms like glp1 and cfs and see what you find.
ie: https://www.reddit.com/r/cfs/comments/1gckc1x/glp1_could_it_be_a_cfs_gamechanger/
I’m in NSW and also seeking microdosing information. The MJ FB group doesn’t allow discussion on this but I found the UK group does.
A friend is under guidance of her GP with a microdosing regime to treat other conditions and I will ask about her experience. She’s only just starting, so it’s all new to her but it’s interesting that a doctor is working with microdosing.
Hey Gretchen, are you microdosing (not taking the full/normal dose)? What dose did you start on, and are you taking Ozempic/Wegovy or Mounjaro?
I took Ozempic a few years ago due to a high BMI, but it didn’t help my usual/chronic symptoms, and caused a lot of gut side effects. I’d like to try microdosing to see if that has any benefits, and I’m in Australia too.
Hi Karyn,
I started using mounjaro for weightloss, and the wellbeing … took me by surprise! I am not microdosing. I started on 2.5 but that was before I started looking into how to avoid side effects and reading up around it and discovering you could go lower. Luckily I did not respond too badly, bit of nausea, not much.
Normally I’m a ‘follow the instructions” kind of person, but the quality and generosity of the advice on the reddit forums from some people showed it was possible to find your own path with this medication. Ie, get the lowest dose and try half of it for example. If you suffered with ozempic it might have been because you jumped up doses before you were ready to, or needed to, or started on too high a dose. Slowly does it. A good GP will support this.
There’s an excellent podcast called Fat Science that really goes into the science of it all, and also suggests going very slowly.
Using compounded versions of the meds for microdosing as the Americans seem to be into, is not recommended for reasons of qulity control. Not sure you can get the compounded lower doses here, but you can control your dose ‘counting clicks’ with the pen, and start on a much lower dose to minimise side effects. And again, do not go up a dose til you feel any symptoms are well stabilised/or you have reached a weight plateau for a few weeks.
Also, do not calorie count or calorie restrict on these meds! It counters the way they work with your metabolism. Keep eating 🙂
PS Mounjaro has a GIP inhibitor as well as a GLP 1 inhibitor. And new meds are being developed which address various others of these mechanisms.
Thank you Gretchen this is very helpful.
And thank you Cort what would we do without you.❤
Thanks!
Gretchen – so glad it is working for you. I definitely have inflammation. Recent health fright: monocytosis and low red blood cells. Pathologist suggests cmml or inflammation. I’m fairly sure it’s inflammation (ME for 15 years).
I will ask my doctor if he will prescribe it but my weight is probably not high enough? (BMI is 25)
This is wonderful. I hope it works long term. I just started wegovy and I think my brain fog is better. Just on the 2nd dose. I do have some nausea at times. I hope tge nausea won’t increase as tge dose increases.
Remember you do not have to go up monthly.
Just stay on a dose til you feel it isn’t working for you.
And you can go up incrementally by ‘counting clicks’.
It did me so dirty. I was praying I would have this response but I got the exact opposite.
Gretchen, (and Cort!) thanks for all your helpful info on this topic ! I started Mounjaro in the US in April 2025 after other GLP-1 drugs were ineffective for my high blood sugar. I also have mild/moderate ME/CFS, for which I started taking LDN in May 2025. I noticed substantial improvement starting in about June 2025, with energy levels, pain and migraine reduction, and severity/duration of PEM. I attributed all the improvements to LDN as I wasn’t aware that Mounjaro could also have a positive effect on ME/CFS symptoms.
Hi, can you tell a little more about your Mounjaro journey and how you administer it?
I don’t know, there might be something to it. I used berberine, which I believe works on a different system but the first few weeks of taking that were amazing.
It seemed to dampen mast cells and gave me an oxygenated feeling.
I also sometimes microdose viagra and I’ve noticed a similar, but noticeable different effect. Better blood flow, but it seems to really dampen mast cells too. So anything that can work on mast cells might be worth trying.
I guess it’s easy to find out in a few trials
Yes berberine has done wonders for me…berberine and diet.
I did a AI search of my own and asked if tetracycline causes liver damage and fatty liver disease.
YES, is the answer
I was on tetracycline at the age of 14.i was on tetracycline for 1.5 years straight.it never did take my acne away but it dam near killed me. So much like whitney dafoe back in the 90s,2000s.
If tetracycline did do this to me ,why would I take drugs that nobody knows what drugs do decades later.
I’ll stay on my diet and berberine and other natural alternatives like interic coated peppermint oil and L.reuteri home made yogurt to try repopulating the gut and push out the bad bugs Hopefully a cure will be found soon.
What took my acne away was taking my shirt off (acne on my upper back) and lying in the sun….it only took 3 weeks of sun to make the acne go away.
1.5 years of tetracycline ruined my life. I ended up with auto brewery syndrome…drunk without having a touch of alcohol along with a severely damaged liver
That’s super sad about the tetracycline. Really awful. I’m so sorry. I get your reticence. But these drugs have been in the marketplace for a couple of decades, as treatment for diabetes. They are well tested.
Hi, I’m pretty sure that the time I spent on tetracycline, also for back acne, ruined my thyroid. I’ve read research papers that state this happens. I’ve been diagnosed hypothyroid for decades now but I think I was undiagnosed for much longer.
I don’t really know the state of my liver but I have Fibro, MCAS, chemical sensitivity, diabetes, high blood pressure & a almost non existent immune system. I would think that tetracycline was instrumental in most, if not all, of this. There’s no other cause in my genetics or life style that would have been a source.
Berberine is also an Autophagy inducer, so it will work in the same way Intermittent fasting and the new drug trial, Rapamycin. Mounjaro of course, induces a form of intermittent fasting and reduces our desire to snack, which will of course induce autophagy. It is well known that me/CFS affects our ability to create autophagy in our bodies. Exciting times!
We shall see! I don’t think the snake oil reference applies as it refers to people intentionally selling false products to make a profit. Thus far GLP-1 agonist drugs have been approved for glycemic control and reducing cardiovascular risk in type II diabetes and obesity. Time will tell but the fact that trials are ongoing in so many disparate disorders (NASH / fatty liver disease, Heart failure (HFpEF studies completed, strong results), Obstructive sleep apnea (FDA review underway for tirzepatide), Addiction / alcohol & nicotine dependence, PCOS, Alzheimer’s & cognitive decline. Parkinson’s disease, GI dysmotility, Inflammatory conditions & post-viral fatigue (exploratory)) though, suggests they can affect many systems.
Have you tried this type of medication, Cort? If not, I would be interested to know why
Also the snake oil reference is to the peddling of the medication for illnesses that it hasn’t ‘yet’ been demonstrated to be effective for
We have to keep an open mind on this one I think
No, I haven’t but I will 🙂
Hi Cort,
Just wanted to share my experiences with the group. I’m part of the SCRIPPs trial and I did get the real medicine based on all the side effects and improvements. It has definitely made a big positive improvement! I still have a ways to go but I was able to get a part time job since starting the trial in December and there’s no way I could have done this a year ago due to the cognitive impairment. This drug has made more difference than anything else I’ve tried. The biggest thing I want to share is that Dr Kaufman is right – the dosing is way too high in the trial! They want me on 50 units (2.5mg once a week). I started at half that and was so sick for the first 3 months I almost stopped. Then I figured out how to reduce the dose and found through trial and error that 4 units every 3 days works sooo much better! The other trick is to give the injection in your leg vs your abdomen and you get a lot less GI issues. Happy to answer any questions but wanted to share as I think it’s the most promising treatment option available today. But start super low, like 0.1mg like Dr Kaufman suggests, and wait 4-6 weeks before increasing due to the long half life. Hope this helps someone out there!
I have had me/cfs for 21 years. The tirzepatide has given me more symptom-free days per month than I’ve had in 2 decades.
I highly recommend! Even if you start by microdosing.
Good to hear and thanks for sharing. What dose are you taking and in what form?
Initially, I was taking semaglutide at its beginner dose with no major side effects. However, after hearing about tirzepatide and how it helps me/cfs patients, I switched over to that. This is when I really started to see more good days.
However, I’ve begun having abdominal tenderness between my ribs & a.little to the right so my doctor suggested taking 2 weeks off of glp1’s to see if it goes away. I skipped my 1st dose yesterday. My abdominal discomfort began reducing late last week as the half life of the drug began to leave my system.
After .y 2 weeks I Will probably resume semaglutide at the BEGINNER dose and see how I feel. If, after that, I’m not seeing as many symptom free days, I will look into microdosing tirzepatide.
I started Zepbound in June, did 2.5mg for two months then have been on 5mg since.
While I did qualify due to BMI, my doctor was willing to try after I sent her info about it being helpful in ME, LC and MCAS.
Starting the second week in Sept my brain fog was a little less. The next week I was able to listen to a webinar for a full hour without significant payback. I also noticed I was cognitively rebounding faster from PEM.
In early October I was able to visit with my BFF for an hour (in bed, while infusing).
Mast cell reactions – I noticed a difference that I haven’t had to use liquid Zyrtec as much, only needing around my menstrual cycle now, and no anaphylaxis since the end of Sept.
I haven’t needed to take meds to lower BP in evenings and haven’t been dealing with adrenaline dumps overnight.
While I have lost some weight, the biggest change has been overall inflammation reduction.
Oh and I am severe, 95% bed-bound
That’s awesome! I noticed the energy effects & faster recovery time but my brain fog was as bad if not worse during both glp1’s.
I sure hope my abdomen gets better soon because I really want to feel like that again.
Try taking it slow. You can stay on a low dose as long as you like, and if you feel you want to increase, do it incrementally by counting clicks, not in as big a leap as the manufacturers say to.
Do you take this every day? Once a week?
Thanks!
Yes, I tried zepbound at all doses, microdose to highest dose and had no improvement in symptoms. I have ME from covid infection. Rapamycin also did not improve any of my symptoms.
thank you for posting, all results good and bad are so useful to hear about.
Hi Michelle what dosing and how long did you try Rapamycin ? Tnx for sharing
Hi Massimo,
I did rapamycin for 6 months. I started at 1mg weekly and titrated up to 6mg weekly.
Tnx. I titrated up to 14 mg, Staude there for 6 months, then to 30 mg without effect. Last trial just starting : 4 mg.
Oh wow, that’s high. Did you have any side effects? Thanks
Actually none, except once on my tongue at the beginning, disappeared soon after
Snake oil is a bit of an overly cynical take. I’m on a GLP1 and GIP with me/cfs. I’ve had some improvement but the mast cell activation syndrome improvement has been great.
It’s been less useful in other parts of me/cfs.
Slight exaggeration perhaps, but it feels quite ‘snake oil’ to me in the way it is being touted by some as a miracle drug that treats every condition under the sun.
I am sure some practitioners advocating for it are genuine. Others? Not so sure.
I have had CFS for 35 years so I am pretty skeptical about these sorts of things. There’s been many false dawns, including from many so called ‘leading lights’ in the ME/CFS.
As I say, I hope my skepticism is proven ill founded this time
Yes and to excellent effect! I was unaware of the benefits in quelling ME symptoms when I started MJ. I’m using it under recommendation of a sleep specialist and my GP to treat sleep apnea by weight loss.
I very quickly noticed improvements in ME symptoms. I have ME as per the International Consensus Criteria, post viral 2012. Am in the moderate to severe spectrum depending on which scale you use.
While I’m still experiencing moderate ME, my symptoms have reduced, I feel the best I have since 2012! I have more stamina, less cognitive dysfunction and am able to perform more tasks or attend social gatherings for longer without inducing post Exertional symptoms.
Cort’s first blog alerted me that benefits within other conditions was actually a thing. As I near my healthy weight range, I’m keen to know if my newfound energy will disappear or not. Also, to learn of microdosing options ongoing. I’ve sent this blog to my GP and hope she can find information and a path forward.
I’m in Australia and MJ is very expensive.
That’s great!
I guess my question would be – are the symptom improvements mainly due yo weight loss? Or working on a key disease mechanism in ME/CFS? Or a bit of both?
Very clearly the drug. It was apparent in the first weeks. Being lighter is helpful but I’m referring to ME symptoms specifically.
Thank you for sharing this info! I’ve had ME for 21 years, also moderate/severe, and reading these accounts makes me eager to try this drug. I’m sorry you had to deal with a question like the above on a site like this. No doubt weight loss helps many things, but how it would touch PENE is beyond me. I started this journey at normal weight and was bedbound for the first 5 years. I’ve gradually improved my capacity for exertion, but have gained a lot of weight over these decades of enforced sedentism. People without PENE can’t begin to comprehend it, it seems.
Thanks for your observation and kind comment Agatha. I tend to cut people a bit of slack on support forums assuming cognitive dysfunction but it was a tad off key… therefore my short sharp reply.
Wishing you the best wellness possible and encouragement to explore GLP-1’s as more data becomes available.
If Eli Lily offers monjaro in vials, instead of trying to divide 10mg into 100 -.01 doses, try doing 2.5 of the vial into 25- .01 doses.
Much easier imo.
Or ADD more sterile saline to the mix to make it less onerous to measure.
I’m starting mj this week – very excited 2.5
We started around the same time! How have you been doing? I have had a shocking improvement in my tolerance for standing activities and it takes more to crash me, but I still can crash especially under stressful conditions. Started getting improvement in my first week on 0.25 and have been titrating up.
You may well have to stay on a maintenance dose for life. I will do that for the wellbeing. You can get a 5mg pen (cheaper by the ml) and dispense half doses for example… makes it cheaper over the long term. You can also get a needle and pull out hte ‘lost dose’ at the end of the pen (it gets called the ‘golden dose’). Various hacks to make it a little less exxy.
I’ve had long covid for 4 years. Within a few days of my first dose of Zepbound my long covid symptoms were gone. Just gone. I have my life back thanks to this medication.
Wow. Congratulations! You are in the GLP-1 agonist subset! 🙂
That’s great.
I hope anecdotes like this are backed up by the studies
Why so negative? We’re all hurting here and any small amount of hope helps us continue to fight for one more day. We get it, you’re skeptical. But quit dumping negativity on every glimmer of hope. If you’re waiting for a cure based on full clinical double blind results, that’s another decade away. Some of us don’t have that long to wait and will try anything. I’m so happy for these people that it’s helped and can’t wait to try it myself as I got accepted into the Scripps Trial. Hoping to start on the med in a few weeks!
Good luck with it.
I’ve had this illness for 35 years. Hope is good. False hope, not so good. I’ve had hope dashed many many times. So apologies for the skepticism.
How many times have treatments been hyped up, only to disappoint.
As I have said, I really hope I am wrong and these drugs provide significant treatment benefits who many / most people with this illness.
Will be good to hear how you go. Also Cort, since he has been promoting this idea.
I guess we shall agree to disagree and we each approach our illness differently. I don’t think Cort has been promoting this idea. He does an amazing job of writing the most up to date blog on ME/CFS and updating all of us on the latest treatment options. It’s here that I found out about Stellate Ganglion Blocks which have definitely helped bring me from severe to moderate/mild. Now I’m hoping that the GLP-1 agonist can push me even further along. Best of luck to you! I hope you find a fully studied, double blind placebo proven treatment that helps the majority of all ME patients and helps you. You might just be waiting a decade or two.
Mary, that is great news! So happy for you! What was your dose? And did you use it daily, weekly? Appreciate your thoughts:)
I’ve had fibromyalgia since the early 90’s. Im taking tirzepatide compound and I take half of the dose early Sunday morning and the other half on Wednesday evening. It keeps things more even for me. My Dr knows I’m doing this and is very happy that something is finally helping me. The day after my first dose, I didn’t need my cane. The reduced over all pain (not my back, hip, sciatica etc still is a pain) and the increased energy has been a blessing. I would use this medication just for that. Weight loss has been slow, guessing that is because I’ve not been able to be active before and my age (65). The only other time I felt this good was a couple days after my Moderna vax. And that only lasted a day and a half. The booster shots didn’t help with that.
Good to hear, Stacie. Continued good luck with it 🙂
I’ve been on it for a year, this month. It has significantly changed my life. No, I am not functioning as a completely normal person, but I’m at a 7 on the energy scale, most days. I have been able to do things this year that I haven’t done in over THIRTY YEARS, like skiing. SKIING!! I am a patient at the Stanford ME clinic, but I got these injections through a different doctor. I fully plan to inform them of what this drug has done for me at my yearly appointment, this Spring.
Hi J, could you share which GPL-1 you use? And also the dose amount and if you take it daily or weekly or…? Thank you:)
I have been using for 3 years on and off due to insurance and then qualification issues. Now that they offer compounded it has been a matter of finding a provide that uses a pharmacy with an effective product. I can promise you this has helped with issues beyond weight. My blood pressure went down along with other weight related issues as the weight came off, but more importantly it began regulating my menstrual cycles. I can say it has helped with inflammation type issues, joint pain, and mysterious issues that i have been looking for answers to with labs. All labs come back with some inflammatory markers high but not enough to say i have an auto immune disorder. Its been a game changer for me, personally. Not to mention the food noise being shut off. I don’t spend a chunk of my day thinking about food and wanting to eat and then eating insatiably.
Hi, just come across this thread while looking for information on GLP-1 and effects on chronic fatigue / ME. I’ve been on mounjaro on and off over the past year (its expensive and i am not permanently employed). I’ve only ever been on the starting dose. I’m literally trawling the internet because of the huge difference its made to my daily life and fatigue levels, we’re talking 4 months ago I was in a wheelchair and 1 month ago I walked round London for the day, no stick, no wheelchair, no symptoms until the very endof the day. Within 2 missed doses the fatigue starts to creep back in, by 4-6 weeks after stopping I am back where I started. I was looking for info to try and take this to my dr without sounding silly, or them considering I was never that ill in the first place OR that this may show some indication of what has caused the overall underlying ME symptoms that we could look to treat without the mounjaro price tag! I’ve found a few threads dotted around from people like myself who has had a remarkable symptom decrease while on GLP-1 meds, and to note, it hasn’t really done a thing for my weight loss so that isn’t the reason for the improvement. This does suggest there may be something tin this, an I’m hopeful it leads to relief for some people with ME and maybe even some indication of the cause of the illness.
Ihave ME/CFS, and started using Wegovy this summer, primarily to lose weight. I have been remarkably well this fall, beter concentration and less PEM. Of course, being n=1, I cannot say whether this is normal variation or the result of the drug. However, I find this really interesting-
May I ask how many doses of these drugs are taken to achieve the effect? Is it a one-time dose or a longer treatment?
I checked and in Germany, one dose of ozempic (if not applied for its approved treatement of type 2 diabetes) looks to be about 104 EUR.
Some people notice benefits right away. Others it takes up to a month if I remember correctly. The drug is taken once a week at the starting dose for 4 weeks; then people who are benefitting or who are not having side effects usually titrate upwards – see how that goes for a while – and then repeat
The starting does to T2D is far higher than the dose these doctors are using. If you can find a way to take it at those low doses the drug will be much, much cheaper.
.
Cort thank you for this blog post! I’m fascinated and I’m in the process of titrating up Zepbound. It’s the first prescription medication that I’ve ever tolerated (shockingly easy) in 11 years with ME/CFS…. but only time will tell if it actually improves me.
Micro-dosing is easier than you think. Most docs seem to start with the 2.5mg vials, which I noticed you did not mention. That way you get through each vial quicker (within 1-2 months, depending on your dose. I would not want to keep an opened vial in my fridge for any longer than that!). And thankfully the un-opened vials have a 2 year expiration date (but must be refrigerated).
For anyone else that is GLP1-curious but wants to know how to get it and the hard costs, let me save you the math headache since I already had to do it for myself:
Each 2.5mg vial is $87 (sold in 4-packs for $349). Doctors orders it here and ship it to your home: https://www.lilly.com/lillydirect/medicines/zepbound
So the cost for the dosing range that Kaufmann is working within are:
0.25mg injection = $8 per week
0.5mg injection = $17 per week
0.75mg injection = $29 per week
1mg injection = $43 per week
1.25mg injection = $43 per week
It sounds like many people settle in at the 0.5mg dosage. But it does get pricey if you end up requiring a higher dose.
The syringes cost is negligible, and I even got my insurance company to pay for them by having my doctor call the syringes into Walgreens as a prescription 🙂
Thanks for all the info! Good luck!
Thank you Dakota and Cort! So I take it you had to learn how to handle syringes and give yourself injections?
I guess that I would not easily be able to access these
vials from Germany; at least online German apothecaries list only pens, starting from 0.25 mg/dose. However, some pens seem to have more than 1 dose (for example, the 0,25 Ozempic pen at 104 EUR including 4 doses). I’m not sure if doctors are allowed to prescribe it for anything but the approved conditions though (even at my own cost), or if compounding pharmacies could prepare vials.
JR, I did have to learn how to use a syringe to draw the medication out of the vial and self-inject (I asked the nurse at my doctor’s office to show me how) — but it is incredibly easy and painless, and the instructions included with the medication are clear so you can figure it out yourself (view here if you are curious: https://uspl.lilly.com/zepbound/zepbound.html#ug1). You just do NOT inject the full vial (which is what the instructions say to do). Instead, your doctor tells you what micro-dosage to inject (which means you’ll get several doses out of the same vial).
I’m sorry that I don’t know about access outside the US. Here, doctors are able to prescribe Zepbound directly from the manufacturer’s website (Eli Lilly – https://www.lilly.com/lillydirect/medicines/zepbound), and then it’s shipped to the patient’s home. The only option for micro-dosing is the vials (because the pens they sell do not have the ability to adjust the dose — no “clicking” feature).
I do not have diabetes or obesity, so my insurance company won’t cover the cost. I have to pay for it all myself — but at the current micro-dose that I am on (0.75mg weekly), it is costing me $29 per week (which I can bring down to $21 per week by moving up to the next vial size on my next order).
Hope that helps; I’m sorry that I don’t know more about access in Germany, but maybe you’ll come across a manufacturer that has a similar model?
Thank you for taking the time to write it up. It is much appreciated :-)!
Thanks for sharing. So how does the microdosing work? Do you repeatedly draw from the same opened vial with a fresh syringe?
Let me rephrase as you’ve already made clear in your previous reply that you get several doses out of the same vial: Are there special hygiene precautions that need to be taken so you can repeatedly draw from the same vial?
P.S.: Sorry for not saying thank you for your prevous reply (I was in a crash). I appreciate it a lot!
I’m not a medical professional so I’m not sure that I should give advice about the proper disinfecting/hygiene techniques, but yes they are super important so you should ask your doctor for instructions when they prescribe the meds!
Yes, I do take 4 doses out of one vial. But I want to be totally transparent that this is somewhat controversial, so you should consult with your doctor before proceeding (as I did). Using these vials more than once runs the risk of vial contamination; and then giving yourself an infection. These are “single-use” vials, which means they do not contain preservatives (and can get contaminated after opening). Which is why Lilly says to throw them away after one dose:
https://www.consumermedsafety.org/safety-articles/single-dose-vial-means-one-time-use-only
https://medical.lilly.com/us/products/answers/can-the-zepbound-tirzepatide-vial-be-split-into-smaller-doses-241673
(Click “YES” to view)
That said, many doctors (including some of mine) are not concerned AS LONG AS you keep the open vial refrigerated, and throw it away after 1 MONTH. So, I throw out my open vial after 4 weeks (i.e. 4 doses) … even if there is some medication left. Personally, I am super conscientious about practicing safe hygiene measures, and I am not terribly concerned about contamination … but perhaps that is cavalier! I have been injecting for 6 months without any issues.
I hope that helps!
Lots of hacks on this, including not going up every month. Which makes it cheaper, also, if it’s working at a particular dose, stay on that dose! (also, buy a higher dose pen but do half doses – makes it cheaper by ml)
Fat Science podcast explains why it isn’t necessary to jump up so often (which has such big effects on the body – nausea etc, which puts people off). No need.
Ozempic doesn’t work in the same way as tirzepatide does. I’ve been on both. It was when I got into the higher doses of tirzepatide that I really started noticing a difference. My family did, too! This was the first year in decades that my mom asked me to make food to bring to Thanksgiving. I made 10 lbs of mashed potatoes! And cornbread…made from CORN I GREW in my backyard, last summer! Oh, yeah, cause I’ve taken up gardening and my yard now looks like a farm! This has been pretty close to a miracle drug for me.
I’ve now been on it for one year. I’ve gone from a 3-4 (with dips down to 2) on the energy scale up to a 7, most days, with some dips down to 4 if I really over-do it.
Thank you! I’m glad for you! Would you like to add some dosage information to compete the picture? What daily dose you’re on right now, how many times per day you inject, and how high do you estimate was for you the daily dose where you really started to notice a difference?
This is so interesting. I was reading patient reports on the Mayo Long Covid list serve and ran across a promising report on the use of cromolyn sodium as a mast cell stabilizer. Since my first and some of my more serious symptoms have related to reactions to foods, medications and chemicals, I asked my ND to let me try it. It comes in ampules and after two tries, it seemed too strong. I remembered that Nasalcrom nose spray is the same thing, but in a much smaller dose. I have been using it for about a week and it has already reduced sinus and nasal allergies. The manufacturer says it can take two weeks to get the full effect of blocking mast cells.
Now here is a hint I learned from my son. I was able to listen to this entire paper using an app called Speechify which you can put on your Chrome browser. There is no charge for a trial and for a nominal amount you can subscribe for a year and choose from a large number of readers. It works on anything that is on your computer screen and phone.
http://speechify.com/
Betty, I’ve watched the shorter version of oslers web with the link you provided.
For whatever reason it won’t work anymore.all that comes up now is
Speechify sign in
Hi Betty, if you have gastrointestinal issues you could also trial oral cromolyn sodium (the product in Germany is called Allergoval). But probably you know that.
Compounded GLP-1 is easily found legally in the US through many telehealth providers. Search Reddit: r/compoundedtirzepatide
That’s good news! Thanks for sharing that 🙂
I’ve been in Zepbound almost a year and have had great results from it. I’ve had cfs for about 13 years, going from mild to severe back to moderate. Zepbound has caused weight loss, plus my kidney disease, mild diabetes and high cholesterol have all gone back to normal numbers. I have more energy and less brain fog. I’d say the one thing not improved is muscle function. I have more energy to try, but even the lightest exertion causes aching muscles the next day, and tbh I’ve had PEM enough times that I’m afraid to push it. That said, I do have less PEM since starting Zep, and have been walking 10 minutes a day. It’s 100% worth the nausea adjustment week to try it.
Adding to clarify; when I started Zep I was moderate, now I’m somewhere between mild/moderate. I started at 2.5 dosage pen weekly, and used that for about 8 months to lose 50 pounds. Then I went to that dose every 10 days or two weeks, which was enough to maintain the weight loss and energy/health benefits. I’ve tried to go back to once a week to lose another 10 pounds, but it makes me lose all interest in food to the point of not eating enough. I’ve not developed a tolerance, except the loss of nausea as a side effect. I’m not worried about slowed gut motility, as I’ve had IBS most of my life and the slow down is welcome. Ask me anything 😄
I have CFS. I also tried Mounjaro and it was absolutely horrible from day one. It reversed my sleep wake cycle, so I had insomnia and was completely out of it in the day, not just from less sleep but because I felt like I had low blood sugar all the time, despite eating. I was counting for the days to pass and I really didn’t start to feel better until day 7. Hands down the worse brain fog I’ve ever had.
Sorry to hear. Dr. Dempsey said this sometimes happens and it’s not unexpected that some people with react poorly. That seems to be par for the course for these diseases. Can you say what dose you were taking?
Thank you. I’m not sure the dose. I believe it was a starting dose that my doctor had samples of.
You might ask him. If he/she had samples they might have been at the standard dose; i.e. much higher than these ME/CFS doctors are starting out at.
I actually found out today it was 2.5mg.
That’s too high for people with these types of illnesses. This article discusses how the starting dose should be lower for those with CFS, ME, Fibro etc as we cannot tolerate the side effects as well. So a lower dose would offer less side effects but still helpful for our conditions and/or weight loss.
It’s easy to micro dose if you’re drawing from a vial via a syringe, or using the dosing pen that’s used in Australia and Europe.
Robin did you ever actually check your blood sugar level during this time because I wonder if the drug pushed it too low in your case and it wasn’t sufficient for you to be able to function? It would be very interesting to know if that was the case.
As part of my very long standing ME/CFS I have been extremely sensitive to my blood sugar levels and I literally cannot cope with anything if it drops very much. .It is complicasted now because I am steroid dependent and of course steroids push your blood sugar up and now my brain cannot tolerate it if it drops to around 5.8 which is a perfectly normal level.
I have to be so careful with carbs and diet in general and never add sugar to meals.
I wonder whether I would be able to tolerate these drugs to help with better blood sugar contral because of this and also I don’t need to loose any weight as I only weight 112 lbs.
I am not overweight enough to qualify for coverage of these drugs, but I was struggling with weight gain and thought it would help give me some momentum. It felt terrible, but I typically have hypersensitive reactions to a lot of meds, except ironically pain medication.
It is interesting what you said about your blood sugar, because i am similar. I am very sensitive to blood sugar changes. I think that is also why I cannot tolerate some steroids, especially methylprednisolone. I cease to function at all and can only lay in bed. I don’t have a problem with prednisone unless on it for weeks, then I start to have the same reaction. I have not been able to figure out the problem. One doctor said it had to do with cortisol. I think blood sugar is also the cause.
I just say I’m allergic to Methylprednisolone the reaction is disabling. A trigger point injection or spinal injection of steroids is by far the worst.
I can say, even though I had a terrible reaction to Mounjaro, I had an incredible results with pain relief from Aimovig— not just migraines, but also multiple other areas of chronic pain… all mostly gone. That did help my fatigue, because chronic pain is so exhausting. I am on disability but I can manage to live independently with support now.
I can’t wait to see where a this latest research goes and might try micro dosing a GLP-1 as mentioned above as a possible route. My doctor is very receptive to my suggestions! Something else that has helped me a lot. Compassion and respect go a long way.
I am extremely skeptical of these results. There are still no long-term well-crafted studies on these drugs. In the low quality studies we do have, so many of the trial patients dropped out from the unbearable side effects. And, too be honest, I’m deeply skeptical of how willing the medical society is to sacrifice fat people’s quality of life for some measure of (almost never permanent) weight loss. Pharmaceutical companies are so very eager to create new clients to generate more money, and we already know how unethical so much of medical history has been and is.
Which studies are you referring to? I’m not aware of ME/CFS, FM or long COVID studies that have been completed.
Pharmaceutical companies are not pushing these low doses or pushing this drug in these diseases. If anything, they’re getting in the way by cracking down on compounding pharmacies. This is all coming from the doctors.
So (some) doctors are cynically cashing in, not the drug companies
Totally agree.
But there us something to sugar abd mast cells as I’ve found with berberine. Really helped me. That’s why I’m curious about tgis. Usually I’d be cynical but it seems like it may help key parts of our diseqse
Maybe read the responses of people who have had a really positive effect? And for whom the initial side effects haven’t been unbearable?
I went on it for weight, and wasn’t expecting or even thinking of improved wellbeing for my CFS. The wellbeing kicked in almost immediately (ie before I started losing weight).
It is possible to start on a lower dose – an ME/CFS friend who was also overweight started it and started on half the min dose to minimise side effects as she was prone to nausea. It’s been extremely effective for her.
Don’t diss those who do want to lose weight: those people have their own reasons and their own life stories and they’re not fatshaming people who don’t want to lose weight.
There are long term studies on overall impact of these drugs for people with diabetes, by the way. They’ve been around for 20 years, and have been a gamechanger for many. Side effects can be horrible. But there are ways to mitigate. And the vast majority take the meds just fine.
Which is not to say I disagree with you wrt pharmaceutical companies and profit. However two things can be true at once.
How does metformin compare? I’m trying rapamycin now, and my doctor is interested in adding metformin too. I’m just over the edge into diabetes, so I guess Medicare would pay for these drugs? Very confused about what to try next.
Perhaps look into berberine. It’s the natural metformin.
Ask your doc about studies comparing the twos performance
Thank You!
I hope someone can determine if these drugs are safe for already underweight ME/CFS patients who struggle to gain weight. In California at least I cannot be prescribed any dose, even the microdose, without a BMI over 30. I know Kaufman says weight loss has not been a problem in his patients, but I’d like more reassurance before I pursue this.
Thanks for the question Corey. I have the same concern. Has anyone out there with normal or a little underweight had success w ME/CFS symptoms (specifically fatigue) without bad side effects?
I am taking .25 Zepbound, and began seeing positive effects around weeks 6 to 7. Don’t know if I’m allowed to say this, but I am using Empower Pharmacy, a compounding pharmacy which appears to serve practitioners.
So far, my “crashes” have been shorter and less severe, and I am having less arm and hand pain. I’m encouraged about the future!
I started Zepbound 2.5mg (full starting dose) last Tuesday for obstructive sleep apnea. I had finally reached the $2000 out of pocket max for Medicare for the year and could try it. Two days later I went to an in person all day conference locally and was able to sit feet-on-the-floor from 9 am to 5pm with only a 30minute rest period lying down midday. That was incredible for me! AND THEN I came home and went to standing dinner date with friends, which surprised all of us! Barely any PEM. By Saturday I was planting trees as part of my fall gardening. Four trees later I ran into some PEM the next afternoon (go figure!) But OMG! Even if this doesn’t last I had a heck of a week! And I lost two pounds 😀 No significant side effects. I haven’t been this functional in years.
This is very close to my experience— and I only started on .25mg. I went to a standing concert days after my first dose expecting to pay for it in exhaustion and a crash, but walking out only my legs and feet hurt and I had great energy. I was shocked. Spent the next couple of weeks baking for the first time in years. I’m not cured— a pest issue at home is taking 100% of my capacity and really showing me that I still have limits and can still get PEM. But my baseline is in a different dimension.
The semaglutide (Ozempic) pens can be click dosed even when the first marked dose is much higher. I’m not sure if this is true for tirz or not though as the pen is different. But this may be a reason to start with semaglutide first.
That sounds interesting! What does click dosed mean exactly? And how d’you sterilise needle when using pen more often than intended? Thanks!
If you google, there are lots of videos which will probably be clearer, but every time you turn the dial on the pen it clicks…a certain number of clicks and you arrive at say 0.25mg. So then you divide that dose by the number of clicks it took to get there and you can know approx how many mg per click and just click that many times instead of the full dose. You can buy generic pen needles on Amazon so you don’t have to reuse.
Trialing such a high dose for patients with MCAS who are already very sensitive is a disaster waiting to happen. I’m one of the unlucky few who had severe side effects even at 0.1 mg of semaglutide weekly.
The REVERSE-LC baricitinib trial landed me in the hospital. I don’t think I’m that special, so there must be others who will also suffer.
Sorry to hear that Nita! I wonder if this – the desire to use the normal starting dose – is going to be an ongoing problems as clinical trials explore these powerful drugs. It’s amazing how difficult it is to get people to really listen to patient’s experiences.
I started Mounjaro 5 months ago (got pen from a friend on Mounjaro). Microdosing using the click pens. My sweet spot is 1.67mg. Anything higher makes me feel a bit ick. I’m not overweight and I’m not losing weight.
I record my health stats on my visible armband app and my health has definitely slowly improved over the summer. But, it generally does improve over the summer, so this winter will be key to understanding the improvements I’ve noticed.
I recently did a 3 day water fast and every single symptom disappeared. This led me down a path of Autophagy and Dr Kauffmans video on Rapamycin. Us ME/CFS people struggle with creating adequate autophagy in our bodies. Sugars, Alcohol, processed foods all increase our inability to achieve an adequate level of autophagy. Is this why we feel worse in winter? All the eating to keep us warm and deal with our worsening symptoms (cyclical effect).
I’m starting Rapamycin today (with oversight of private doctor and blood tests etc). Got it from alldaychemist.com.
I’m still taking LDN (1ml), Mounjaro (1.6mg) and wearing Nicotine Patches. No contraindications either. Fingers crossed 🤞🏼.
Hi Nick,
How did it work out combining Mounjaro and Rapamycin?
Did you get on with them both singly first, or only ever try them together?
I thought of mixing the two as a potentially bad idea since they work similarly?*
I ask because I have been thinking of starting this combination myself (as far away from each other in the week as possible)
How did you get on with Rapamycin? I can’t seem to get past 1mg. The first and second time I took it, for a few hours I felt absolutely amazing. Like Superwoman.
That was 2 months ago. I’ve been really really slow at titrating – was on 1mg weekly for 6 weeks and didn’t see any improvements.
I tried 2mg in week 7 and 8 (now end week 8) and have been absolutely wiped out with an horrendously sore throat (not red and sore internally, but my actual physical throat itself, without it being glandular. Very strange . Can’t stay awake and feel kinda fluey. However; life has been very stressful recently, so it’s hard to tell if I’m not just worn out.
I’m currently trying to work out if it’s worth continuing with even 1mg, especially as I want to try microdosing Mounjaro for health reasons (i’m not overweight, just have an uncomfortable perimenopause belly).
I have my first prescription on its way to me now.
What’s been your experience with both Rapamycin and Mounjaro together and apart?
Many thanks in advance for your time 😃
*Despite its shortcomings, I asked Claude, since my own shortcomings are worked right now 😆
Issue 1: Mounjaro affects rapamycin absorption
This is the most practically important finding. Mounjaro delays gastric emptying and has the potential to impact the absorption of concomitantly administered oral medications.  Rapamycin is an oral tablet, so this matters directly.
Issue 2: They work on overlapping pathways
This is the more scientifically fascinating part. GLP-1 receptor agonists stimulate mTORC1 signalling via PKA phosphorylation  — meaning Mounjaro is actually activating the same mTOR pathway that rapamycin is trying to suppress. They are working in opposing directions on the same system.
Researchers found substantial overlap between the effects of GLP-1 and rapamycin in terms of how they influenced biological pathways, with effects similar to calorie restriction. 
What this means for your dosing:
These two drugs should probably be on different days for two reasons:
• Avoid Mounjaro interfering with rapamycin absorption
• Avoid them directly competing on the mTOR pathway on the same day
My suggestion: Keep rapamycin on Monday, and take your Mounjaro injection on Thursday or Friday — maximising separation between the two. This gives rapamycin clean absorption and reduces pathway competition.
What day are you currently taking your Mounjaro?
Hi Abz, I stopped Rapamycin after a few weeks due to really bad mouth ulcers. I haven’t started it up again. I’m not sure if Rapamycin is a good idea for people with low iga.
I’ve actually stopped microdosing Mounjaro too. I had my usual decline in the winter months and just felt I needed to look elsewhere.
I’m now on several MCAS meds to deal with my histamine issues. They’ve working, just need to fine tune the dose.
I have been leery of trying these drugs, due to years of dealing with nausea and IBS-D. But I have had good results so far with two nondrug GLP1 agonists: Akkermansia (in the Pendulum probiotic) and allulose (products from RxSugar and others). I have dropped around 20 lbs in the last couple years without food restrictions. Have you heard anything about these?
Almost everyone in the comments reporting benefits state that they were overweight and/or had blood-sugar problems. Of course if these medications are helping these specific comorbidities, your overall health will improve.
I’m therefore less then enthusiastic for pushing these meds on ME-patients in general. Especially as most of it is coming from Dr. Kaufman, who lately was involved in pushing rapamycin and oxaloacetate for ME, which have been tried by many people without any meaningful success, at least here in Europe.
I simply cut out all sugars and carbs and lost 30 lbs.
Very quickly
ITS THE LIVER FOLKS
Can you elaborate? My liver function tests are fine. Genuinely interested
Oliver….I used AI and asked if tetracycline causes fatty liver disease. The answer is “yes”
My liver tests are fine also but the internal medicine doctor keeps saying its my liver.my ND also states the same.
The internal medicine dr. Asked if I was a heavy drinker.
I stated I never drank anymore than anyone else.
I know friends that drank way more than I did and they continued to drink long after I quit….they don’t have me/cfs.
I had to quit decades ago because early before all hell broke loose one of my first problems was, I would have a drink or two and be hung over fir more than a week, so I quit…then, all hell broke loose
As stated by the researcher Robert navauix, tetracycline is one of the bad ones listed
Interesting. And thank you for your explanation.
Many people are exposed to that antibiotic. Why us? I’m certainly not discounting what you’re saying. I don’t have a fatty liver as I has it scanned 2 years ago I love bob naviaux s work.
There’s some weakness in us that allows these kinds of injury surely
I HAD a white furry tounge.
I WAS a person that HAD auto brewery syndrome
I also HAD the swollen brain and spinal cord.possibly still very slight now
I know i had auto brewery syndrome because I went to a drinking establishment that had a breathalyzer and blew over 3 times
Thanks for pointing me in the direction of supplements: Allulose and Akkermansia both seem easy to access and try. And I saw that there are dedicated GLP1 booster supplements in the market, too.
Gah, I’m at my energy limit again, being your “own doctor” is really exhausting.
Akkermansia has a lot of promise, and is likely missing in the guts of most chronic inflammatory patients. One must get the gut into better shape in order to modulate the inflammation pathways – I’ve spent a year and review of hundreds and hundreds of journal articles to better understand the interplay.
A protein in this bacterium, Amuc_1100, activates TLR2 and TLR4, stimulates GLP-1 release by the body, and increases levels of beneficial bacteria like Firmicutes and Actinobacteriota. The increased bacteria produce Acetate, Butyrate, and Propionate (and live Akkermansia also produces Propionate) in the colon, and these Short Chain Fatty Acids are anti-inflammatory, feed the colonocytes, and also enter systemic circulation where acting as Histone Deacetylase (HDAC) inhibitors, they can lower levels of pro inflammatory cytokines, lessen microglial activation, etc. Akkermansia also helps to lower insulin resistance which has been indicated in ME/CFS research as a potential disease factor.
The GLP-1 also inhibits Mast Cell Degranulation and mediator release, by binding to receptors on the mast cells. Recent research has shown Fibromyalgia to likely be a mast cell mediated disorder, too.
Some studies show pasteurized Akkermansia may be more effective for some uses and have lower side effects, including impacting other gut microbes. Pendulum’s is live, and that can be beneficial as well – though unless the gut ecosystem is repaired (and even in that case), colonization of any probiotic in the human adult gut is highly unlikely to succeed due to the interplay of the ecosystem. Probiotics may, however, get trace levels of similar resident species to be able to re-bloom.
Also of interest, Akkermansia can redirect Tryptophan metabolism in the gut away from the Kynureine pathway that has been implicated in other ME/CFS research, as well as studies showing a reduction of depression symptoms.
Powerful stuff! Worth noting as well, one study showed that supplementation of cranberry extract in rats caused Akkermansia to re-bloom within 7 days. Again, this is all dependent on the condition of one’s individual gut ecosystem. My hope is continuing research will further explain what differentiates responders to non-responders of these various therapies, and how they play a larger role in various diseases.
Thank you for your comment, Corey. This is certainly one of these interesting comment sections :-).
Pasteurised Akkermansia? Does that mean dead bacteria do something in the gut, too?
There seems to be research by now on whether cranberry extract can stimulate Akkermansia growth in humans, too: (https://www.nature.com/articles/s41522-024-00493-w , search Results section for “A. muciniphila” to see results). If I understand it correctly, the answer seems to be you’d have to already have the bacterium for it to be increased by cranberry extract, and it nevertheless also decreased in some of these individuals. Also the composition of the cranberry extract matters.
Yep, there are all sorts of things that dead bacteria can do in the gut. Hence, the value of fermented foods that likely are mostly killed by the stomach acid. There is now a lot of research on postbiotics, and how they can change the gut composition even without being alive.
The cranberry extract is really curious – and I do wonder if other pathogenic species just crowd out Akkermansia during gut and immune disturbances, or if somehow it gets eliminated in total in autoimmune or auto inflammatory diseases. This could easily be why the impact of good diets is blunted, as the synergy is lost.
Thanks for sending me down that rabbit hole. I see that Cranberry Extracts that are solely PACs and sold as capsules. Makes me wonder if the cranberry capsules I bought earlier, while incredibly potent, are the wrong kind to provoke a bloom. Certainly didn’t get Akkermansia back from them. Also, that one study showed concurrent administration of Akkermansia probiotic and Quercetin resulted in colonization, which is rare and hard to do in adults!
And worth noting too, GLP-1 drugs seem to bloom Akkermansia in responding individuals (which may be part of their mechanism of action). Which makes me curious if those that don’t respond were to take an Akkermansia probiotic in conjunction with GLP drugs, if that would change the presentation as it may create a habitat suitable for colonization.
In an article on Alzheimer’s, Akkermansia was also shown to inhibit the microglial activation in the Hippocampus via IL-10. So, this could allude to some of the profound effects of GLP drugs!
Hello Andrea, based on your comment I’ve just gotten allulose to try. Would you have some information on how much allulose you’ve been taking per day?
Thank you and thanks for pointing me to that supplement. I wonder if it might possibly have a use for diabetes prevention in severe ME/CFS patients like me, too.
Poke around the rxsugar.com site and see what they recommend.
Thanks for your reply! I’ve had a look and it seems they don’t recommend a daily dose. I was wondering if you simply used it to replace sugar in your diet or took it like a supplement, like x teaspoons y times a day?
If you can’t say, it’s not a problem, I’ll try to google studies then :-).
I use allulose as a sugar substitute, mostly – the syrups are good in lattes and over plain Greek yoghurt. But I also take 2 of RxSugar’s allulose gummies to quickly shut down cravings, between meals or after eating a good meal that leaves me restlessly wanting something else even when I can tell i’m not hungry any more!
Once again, treatment without knowing what they are treating.
“Kaufman believes that by reducing systemic inflammation, GLP-1 agonists are targeting one of the root causes of these diseases and helping fight reactivated pathogens such as EBV.”
Did I miss something…what root causes? What is causing the inflammation, the reactivation of EBV?
All of these GLP-1 agonists can have serious side effects in some patients. Rarely, thyroid cancer. It might be worth the risk, if they were sure what they were doing but I don’t think so.
It is time for everyone who has ME/CFS or is attempting to treat it to go back and either read the 700 page book or listen to a shortened version of Osler’s Web by Hilary Johnson, an investigative journalist who spent nine years researching the history of ME/CFS, a condition that she also has.
Here is the condensed version you can listen to on Speechify
https://docs.google.com/document/d/1qWhHxKxxwM1tUCpFRYmDDiAlZ7fZLalhT3VeNDk7_8s/edit?tab=t.0
Speechify.com
I absolutely agree with you Betty. Honestly, I think there are some individuals who know exactly what causes this disease (at least for some individuals) but they will never admit it as there would probably be a ton of lawsuits.
A very telling patent by a Tulane University researcher: https://patents.google.com/patent/WO1995031531A1/en
This recent condensed book by Hillary Johnson is also excellent and very eye opening: The Why: The Historic ME/CFS Call To Arms
Do they know what is causing ME/CFS? I think so.
In 1986, a new virus was isolated in the USA from patients with AIDS as well as lymphoproliferative disorders. Initially designated “human B-lymphotropic virus (HBLV)”, the virus was renamed human herpesvirus 6 (HHV-6).
In 1987 and 1988, independent isolates were obtained from AIDS patients in Africa .As other strains were isolated from various geographic regions and clinical settings, it became gradually apparent that all HHV-6 isolates could be included in one of two well-defined groups, differing in their molecular, epidemiological and biological properties.
An Ad Hoc Committee on HHV-6A & HHV-6B Genomic Divergence was formed in 2009 to generate an official proposal to recognize HHV-6A and HHV-6B as distinct viruses, which was submitted to the ICTV in 2010. In 2012, the ICTV officially ratified the classification of HHV-6A and HHV-6B as distinct viruses.
You can be tested for HHV-6B at Quest Labs and the national prevalence rate is estimated to be as high as 90%. Not so, for HHV-6A which can only be tested for at specialty labs. Because of this, the prevalence rate is unknown.
While HHV-6A and HHV-6B are both neurotropic, there is evidence suggesting an increased severity of HHV-6A over HHV-6B in cases of clinical neurological disease. In addition, although an overwhelming majority of post-transplant reactivation occurs with HHV-6B, HHV-6A DNA and mRNA are found more frequently than HHV-6B in patients with neuroinflammatory diseases such as multiple sclerosis (MS).
Marmosets inoculated with HHV-6A intravenously exhibited neurological symptoms.
HHV-6A is a type of human herpesvirus that can cause a lifelong, latent infection and reactivate later in life. While it doesn’t have a single characteristic illness, its reactivation is linked to various neurological and other health problems, including encephalitis, multiple sclerosis, and chronic fatigue syndrome.
Metformin has been shown to inhibit HHV6A.
YOU GO BETTY MEKDECI. !!!
Know that you are an true hero digging for truth in this world
You’re certainly right to point out the actual root causes are not known yet.
My bet is on ME/CFS being a disease with a very strong epigenetic component, both in the initial trigger mechanism, and in push-crash-cycles. My guess is that a trigger event of systemic (immune) stress so-to-say flips an epigenetic switch to trigger ME/CFS, and possibly what flips that initial switch could be viruses that get reactivated by the immune stress event and – without necessarily replicating themselves – influence cell metabolism epigenetically at cell level (that’s something viruses do, as far as I know).
I’m thinking of Prusty’s work here, who not only looks at how herpes viruses influence cells, but also at how just a few infected cells can influence others via cell signaling, and how there are stages of viral reactivation that mean the virus becomes active without necessarily replicating.
In my opinion, all known initial triggers in my opinion have in common that they are immune stress events (even mental stress, due to its connection between stress and immune systems. We all know how for example mental stress can cause a cold sore (Herpes simplex) to erupt.)
In my opinion, ME/CFS is likely a cascade regulation failure in the body. And I strongly feel there should be more epigenetic research into ME/CFS to identify what’s the possible first epigenetic domino(es) in this cascade.
I somehow feel this idea might be related to your work with veterans which looks at environmental factors triggering disease.
As an alternative to the injectables, I’m wondering if anyone has opinions or experience with GLP-1 oral drops? It seems these would be easier to adjust and microdose than the injectables, especially if you don’t want to lose weight. Any thoughts?
They’re not recommended as who knows who made them? Anything could be in them. Absolutely not recommended by doctors.
The injections are not as awful as you might imagine, just fyi.
As it seems that there are many indications (both reseach and patient reports) that glp-1 agonists can in cases significantly reduce inflammation, I followed an educated guess: maybe glucagon is not only primarily a glucose messenger but maybe it doubles as a secundary immune messenger?
This is what I found:
https://pubmed.ncbi.nlm.nih.gov/30661789/
with title : “Toll-like receptor 4 is necessary for glucose-dependent glucagon-like peptide-1 secretion in male mice ”
Saying “We found that the TLR4 deficiency impaired the glucose-induced GLP-1 release and prevented an increase in IL-6 and TNF-α levels in plasma and ileum following glucose stimulation.”
=> Well, actually my initial thought may have been wrong. It seems without the (very important) immune receptor TLR4, glucose doesn’t even moves GLP-1 or glucagon levels.
=> Why I say my initial thought was wrong? Because glucagon does seem to refuse to play it’s supposed main role of glucose regulator without any action of immune receptor TLR4. So basicaly there is indication that glucose regulation may be the secondary effect of glucagon, and immune regulation the primary effect.
=> If so, that would be a rather important / huge change in concept with plenty of ripple through effects on how to look at the relationship between metabolism and immune functioning.
=> If so, the hypothetical primary role of glucagon and glp1 as an immune signal more so then a glucose metabolism signal would explain a lot of how glp1 agonists have such broad effect on immune related disseases. The side effect would be that administering them would lock a main immune signalling molecule in a ‘fixed-always-on’ setting, taking some ability away to help catch types of infections.
See also
https://www.cell.com/cell-metabolism/fulltext/S1550-4131(23)00420-5
with title “Central glucagon-like peptide 1 receptor activation inhibits Toll-like receptor agonist-induced inflammation”
and
https://cellandbioscience.biomedcentral.com/articles/10.1186/s13578-025-01486-8
figure 1: glucagon helps regulate a majority of immune cell types.
It seems the primary food sensing action of GLP1 is on the gut (lumen, ‘food side of the tube’), not on the blood / plasma.
GLP1 is secreted by intestinal L-cells. https://en.wikipedia.org/wiki/Glucagon-like_peptide-1.
It regulates gastic emptying, by sensing new food by bowel L-cells in the duodenum and jejunum (first parts of the small intestine).
But according to the same article, GLP1 is mainly secreted by L-cells in the distal ileum (last part of the small intestine) and colon (large bowel). While I could still see a role of ‘sensing food content’ at the distal ileum, in order to regulate food passing to the colon depending on digestion state, it increasingly become places heavy in beneficial gut microbes (very low numbers at the start of the small intestine to massive numbers at the end of the colon).
By all I did found our body only produces GLP1 in cells facing the ‘inside’ (‘food facing side’) of the digestive tract. I can see more then one role for regulating digestion and absorption of food, but for sensing how rich the blood / plasma is in nutrients like glucose and fatty acids, it is simply the wrong side to do this measurement.
Then what does it measure? IMO the combination of food amount and type, amount of digestion of the food, gut bacterial content and gut health.
A) food amount: obvious role of L-cells releasing GLP1 when they sense various foods in the digestive tract.
B) food type: there is various info to be found on L-cells responding with GLP1 secretion to a different degree depending of the food type they detect
C) L-cells react heavily to bacterial components and bacterial fermentation products
D) inflamed / ‘flattened’ bowels produce considerably more GLP1 then healthy bowels (that have plenty of very small structures that are ‘erased’ when there is excessive inflamation)
for B) and C): look at https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2019.00082/full, figure 1 for the large amount of different food and bacterial (and immune signals going with microbial pressence by the many TLR’s) signals that are combined by gut L-cells to decide how much GLP1 is secreted.
for D) (very short version): https://en.wikipedia.org/wiki/Glucagon-like_peptide-1
“Endogenous GLP-1 is rapidly degraded primarily by dipeptidyl peptidase-4 (DPP-4), as well as neutral endopeptidase 24.11 (NEP 24.11) and renal clearance, resulting in a half-life of approximately 2 minutes. Consequently, only 10–15% of GLP-1 reaches circulation intact, leading to fasting plasma levels of only 0–15 pmol/L.”
The thing is: by all I found L-cells are not found in the brush border of the bowels. In simple speak: they are not located in the ‘branched endings’ giving the bowels plenty of surface area. Cells producing DPP-4 enzyme are by what I found much more spread over the bowel surface, including the brush border part. That is the part that gives the bowel massively more surface area.
Severe bowel flattening due to excessive bowel inflammation hence strongly reduces DPP-4 producing cells (as a rather large portion of them is in the ‘shaved away’ part of the bowel) while most of the L-cells remain intact (by being dominantly locted in the parts that remain even after bowel flattening).
=> combining the strong effect of DPP-4 on how much GLP1 remains intact, this combo makes for an attractive sensor of a healthy bowel with large bowel surface area versus an inflamed and flattend bowel with poor health.
=> since in near all research GLP1 agonists are painted as anti inflammatory, this combines to a negative feedback on bowel inflammation: when there is too much inflammation, DPP-4 production drops a lot and surviving GLP1 increases a lot. That acts as an anti-inflammatory signal probably helping to contain the excessive bowel inflammation and preventing it ‘eating the entire bowel away’.
Combine that with A), B) and C). Knowing the nutritional state in the bowel, when *specifically looking for what nurtures a healthy gut microbiome* (rather then what feeds the human) and what microbes are pressent and you end up with a signal rather helpfull at determining how healthy / stable the gut and its microbiome is. And with it how resilient much of the gastro-intestinal tract is and what is an ideal setting of gut immune and inflammation.
There is information to be found about beneficial gut microbes that learned to increase GLP1 in their favor too, further helping with GLP1 as a gut health sensor.
When searching for clues on this hypothesis:
https://pubmed.ncbi.nlm.nih.gov/36296337/
with title “GLP-1 and GLP-2 Orchestrate Intestine Integrity, Gut Microbiota, and Immune System Crosstalk”
=> So the idea of GLP1 being important for gut health is nothing new. What I propose (if it is not done yet) is that this immune function is a primary (not secondary) function of GLP1 and that it’s food sensing abilities are optimized to determine what is optimal for our microbiome more so then directly ourselves. Given the huge impact of gut health on the global immune system and countering chronic disease, it may help painting a picture of what GLP1 agonist can do (at the cost of constantly signaling: ‘poor gut health! reduce inflammation now!’ and with it become poor at certain classes of pathogen detection).
Thanks for pointing me in the direction of supplements: Allulose and Akkermansia both seem easy to access and try. And I saw that there are dedicated GLP1 booster supplements in the market, too. They contain for example reducose which is I think a mulberry leaves extract.
Gah, I’m at my energy limit again, being your “own doctor” is really exhausting.
I have been taking Mounjaro for weight loss for 6 months.
Although I did have a slight improvement in symptoms for the first few weeks this was short lived and my ME returned to its normal levels
tried tirz, sema, and reta. first 2, lots of side effects like bad constipation or loose stool, nausea, hair loss, low mood, and the worst was the fatigue. I lost 40 pounds in 1 year though. allergy symptoms improved but no decrease in pain. switched to reta a few months ago. my only side effect is hair loss with minimal weight loss but I’m not at the therapeutic dose yet. no improvement in brain fog. I do like the blood sugar control–I tend toward hypoglycemia.
What dose did you take with tirz and sema? Good luck with reta 🙂
.25 mg twice a week sema. 4 mg tirz. due to side effects, I could never get higher.
What is reta? Thanks.
retatrutide. it’s another glp-1.
Thank you!
https://www.healthandme.com/nutrition/feast-famine-and-fat-loss-new-diet-trend-better-than-intermittent-fasting-could-help-you-lose-weight-faster-article-152142965/amp?fbclid=Iwc3J0YwZhcHBfaWQPMjc1MjU0NjkyNTk4Mjc5AAEeszEk-vbVmc464vna4iFq5GCugVNeBp7re00Pht3-Z_TlPi0CpUwxSkuJqm0&brid=wDlYFqZbaAMP0rZn5OPhMQ
Drugs or fasting??
Re: GLP1 and increased cap blood flow comment in the video
It.s a real effect and some effect is via nitric oxide and also there are NO independent effects.
John Haughton MD, MS
Renegade Research CMO
and “unidentified commenter”
Happy to discuss further if questions arise.
Below is an example reference.
Vasodilatory Actions of Glucagon-Like Peptide 1 Are Preserved in Skeletal and Cardiac Muscle Microvasculature but Not in Conduit Artery in Obese Humans With Vascular Insulin Resistance
Nasui Wang 1,2, Alvin WK Tan 1,3, Linda A Jahn 1, Lee Hartline 1, James T Patrie 4, Shaoda Lin 2, Eugene J Barrett 1, Kevin W Aylor 1, Zhenqi Liu 1,✉
Author information
Article notes
Copyright and License information
PMCID: PMC7035589 PMID: 31888883
G’day John,
Thank you so much for this comment. I have OCHOS (as described by Peter Novak), and upon looking on PubMed after reading your comment I found this article:
https://pubmed.ncbi.nlm.nih.gov/33942194/
“Glucagon-like peptide-1 (GLP-1) receptor activation dilates cerebral arterioles, increases cerebral blood flow, and mediates remote (pre)conditioning neuroprotection against ischaemic stroke”
(I do not have CFS but follow Cort’s blog as he often covers OI, autoimmunity, etc., which are relevant topics for me.)
Dr Novak has hypothesised that autoimmune-type OCHOS is caused by the cerebral arterioles being abnormally constricted. I have been trialling steroids and DMARDs with limited success. As I am currently overweight, maybe my GP will try me on a GLP-1 agonist for that indication. (I won’t mention the blood flow or autoimmune possibilities.)
I just saw a Jarred Younger video in which he very strongly advises against using these drugs. Until papers are published etc. In the best of times, those take..what, a decade? And the vast majority of funding has been slashed here and etc. He also didn’t seem aware that doctors are using microdosing. He didn’t say that directly but it was conspicuously missing in his discusssion, and he seemed to be going on the side effects profile of the weight loss dose.
Then seeing the limitations on NIH funded trials… I cannot see how all of the hurdles to research can possibly be met to prove this is safe for use in MECFS. I was extremely skeptical about the hype on this, but have a friend with MECFS who began it at very low doses, can’t really afford to lose weight or bone density (neither can I) and she’s reporting really positive intimal effects. I have no idea, I’m so tired of being a guinea pig and gettng my hopes up. The risk seems far lower than spinal surgeries, for certain.
This isn’t news but we really are in such a bind with this. Sick, debilitated and in honestly agonizing intractable pain for 18 years… and I’ve tried some really horrific drugs. It’s very hard for me not to want to look into and try this. The Younger video was such a definitive ‘no do not try this’, it threw me.
Micheal…I will tell you what i did.
I took it upon myself to try ivermectin. Ivermectin is a very very safe drug. In fact I don’t understand why they even call it a “drug”
Ivermectin and fenbendozole pulled me out of a deep hole so to speak.
I HAD pain so severe
In no way I’m I telling you how to treat yourself or giving you medical advice
I can see why someone might say that for full dose, and it is true that a minority of folks have bad effects even on tiny doses, but some people (myself included, but also as per this article ) have had very positive effects on doses so tiny they do not provoke many side effects. It seems that for many the potential benefits could far outweigh the risks, for very small doses.
just started this today so I can’t speak to the effects yet,
But in addition to Australia, in Europe (Netherlands) Mounjaro click-pens with which you can administer microdoses (I take .25 mg which is six clicks) are available at pharmacies. just FYI
Good to know! Thanks 🙂
Hi Annabella — so is that the 2.5mg Mounjaro Kwik-pen? (6 clicks = a 0.25mg dose?)
yes, exactly.
Thanks. I’m about to try the same thing/same dose.
Can I ask if ( assuming it helps) you intend to use beyond 4 doses?
I’m unsure about keeping the pen beyond a month, although I assume the 1 month expiry date is extremely conservative … and if refrigerated it should be fine.
I probably will make the pen last a little longer, it seems like pretty common practice on YouTube with people to cut on cost… anyways I saw this doctor explain the mechanism, but it could be just a guy with a lab coat for all I know!
Haha! Very true. I also think I’ll probably extend it for more than 4 doses (cost here in Australia was $280 AUD for the 2.5mg pen). I hope it helps you. I’ll let the chat here know my response too. Starting first dose at 0.25mg in next couple of days.
I’ve been doing this with the pen and having it last at least 2 months. (ie half dose of 10mg pen for me, to save costs). Just keep it in the fridge, use alcohol wipe on the top of the pen each time, don’t reuse needles.
If it goes cloudy (not condensation) then I’d throw it out.
Thank you — makes sense.
Following up with my experiences with tirzepatide (Mounjaro): I started at 0.25mg. Injected a second dose of 0.25mg a week latter. Then increased to 0.5mg a week after that. My intention is to stay at 0.5mg for a month at least, depending on response. Positives have included improved sleep, cognition, drive, reduced anxiety, reduced PEM. Negatives have included some sleepiness/fatigue, slowed digestive function. Overall pros easily outweighing cons, and I’m cautiously optimistic. Has helped me manage better at work (part-time). (Note — the dosages I’m trialling here reflect what the dosctors have said in the YouTube clip and on Reddit.) IE start at 0.25mg and carefully/slowly titrate up based on response.
Hi Annabella, I am German + live in France. I checked in both countries + called Dutch pharmacies, asked for pen where you deliver 1 dose in several clicks (clickpen)
nowbody nows of anything! my question is, from which pharmacy you got yours from?
Does it say click-pen on the product? .
I give you my e-mail address, don’t mind it being published: stephaniepotratz@gmx.fr
Thanks so much for your help 🙂 Stephanie
Reading and writing here five days after a mild ME/CFS flare-up. Since I had to travel on the third day I resorted to good old aciclovir, first synthesized in the 1980ies, that I have in stock for emergencies.
The 3x800mg a day did their job of suppressing the inflammation immediately and reliably.
In between flare-ups I rest and pace as good as I can and am recovering slowly.
I look forward to the day where the role of herpes in ME/CFS will be understood.
Sometimes when I read here in the comments I wonder whether ME/CFS patients – just as anybody – are running after only ever the newest things on the market instead of thinking and analying which drugs should have been thouroughly investigated for decades.
Hi Roonie,
I am sorry that Speechify isn’t working. My son installed it on my computer so I am not much help with the technical side.
I thought I should chime in since success stories are always reported by the happy patient, but not so much if it fails. Not only did Tirzepatide not help me it made me WORSE. I do not mean just side effects, I mean way less energy. It felt as if my body did not have normal access to carbs to process the little energy I have and the result was getting weaker and weaker. I started at 1 mg and increased weekly slowly topping out at 2.5 mg week. I had to call it quits at 5 weeks as it was going the wrong direction.
I also agree that Dr. Kaufmann is promoting this medication with too much anecdote and not enough research. He is not a Ph.D researcher, just an MD, who has anecdotal evidence of his successes and no placebo control on any of his work. Sorry but that is not science.
Agree that Kaufmann’s stuff is not science, but I’m having a happy experience with Zepbound and I’ll take it.
Not surprised with inconsistent results. I’m not aware of any other chronic conditions that have as wide a range of symptoms as ME/CFS, Long Covid, and FM. Though ME/CFS, for example, has a few common themes between patients, the symptoms have a huge variability between patients. It’s very individualized, almost like each patient is a unique manifestation of a very generalized classification of an illness, and different patients will react differently to treatments.
Perhaps researchers are trying too hard to find solutions for many, when it may require a “custom” solution for each, while acknowledging that the patients all fall under a the same broadly generalized classification. This is very hard stuff, and no wonder it’s tough sledding.
Who is claiming it is ‘science’? Where in the spectrum of pharmaceuticals tried for ME/CFS is there ‘science’ by your criteria, noting there is not a single pharmaceutical treatment that is indicated for this condition? And there is peer-reviewed research about their role in reducing inflammation, including neuroinflammation. If anyone is claiming that GLP-1s are the answer or cure for CFS, then they can rightly be criticised. But if patients and doctors are simply stating that there are a good number of anecdotal accounts of positive responses to these medications, then that in itself is a good news story … and if trialled at low doses it may represent a reasonable idea for someone on a risk/reward basis, if they do so in partnership with their doctor. I don’t understand a lot of the negativity in these comments. It’s like criticising someone for going to have a hit of tennis by saying ‘I warn you, there is no evidence you will ever win Wimbledon’. Noting some of us have been sick for decades, why on earth wouldn’t we trial something like this at a low dose? Critical comment is welcome, provided it makes sense!
I just found out today that I have been accepted into the Scripps LoCITT trial. I will keep everyone posted on my progress (hopefully I get to have the medicine — they are doing 50% Zepbound and 50% controls)
Have headaches as a symptom of ME/CFS and brief experience with Wegovy was that headaches doubled in intensity.
Now trying Zepbound, and after first full day fatigue seems considerably improved, orthostatic balance issue is virtually gone, cognition improved, brain fog reduced. Headaches slightly better.
I’m from Canada and have fibromyalgia and osteoarthritis. I went on wegovy for two months and had total remission of all my horrendous symptoms. Felt I had a new life. I wish the trials were available here
Cort, have you seen this study on Rapamycin and CFS? Also posted an article discussing it.
https://link.springer.com/article/10.1186/s12967-025-07213-8
https://agelessrx.com/what-chronic-fatigue-teaches-us-about-aging-immunity-and-cellular-repair/?lid=uw95v62xv9uy&utm_source=braze&utm_medium=email&utm_campaign=ARX_LongevitySpotlight_November2025_ActiveCustomer
Thanks Steve. A blog is coming up on that. Thanks for the links to the articles!
Your welcome. The study mentions insomnia as one of the main adverse symptoms which I can attest to. After reading about the study I started on Rapamycin a couple months ago at 1 mg (the beginning dose in the study) and had anxiety and couldn’t sleep for a week so I had to ratchet back to a quarter dose and slowly move back up to 1 mg where I am now. I wonder if the insomnia was a reason so many of the participants dropped out (about half dropped out). Anyway, it seems there is some momentum behind Rapamycin due to the growing belief that, for a certain cohort of those with ME/CFS, mTOR over activation may be at the root of their ME/CFS (at least that’s what Google AI says when you google mTOR activation and CFS). FYI, in the US you can get Rapamycin through AgelessRX and Healthspan. Good luck and I look forward to your article.
Here are a couple more videos. One by Solve M.E. on the Rapamycin study and one by Kauffman and Ruhoy on Rapamycin as a treatment in their practice. Kauffman says he sees improvement in 2/3 of his patients with Rapamycin. They are both very high on it and even use it personally for its longevity benefits. Apparently mTOR becomes over active as we age so that’s the reason it’s used for longevity. It would also explain why some (most) of us with ME/CFS slowly get worse as we age. If our ME/CFS is caused by mTOR over activation, and said over activation gets worse as in everyone as they age, it’s just an impossible battle to win. All the little secrets/biohacks we try help some but it’s like swimming against the current and you just continue to lose ground over time.
https://www.youtube.com/watch?v=n5KghnVAIAU
https://www.youtube.com/watch?v=LRXHPmuDPnc
My daughter (22) is suffering from ME/CFS and POTS after an infection with influenza virus in 2018. She is so far treated with Mestinon 180 mg retard, Propranolol 10 mg 2xd, Ivabradine 5 mg 2xd.
2022 she was on a good way of recovery, finished school, started part-time university, lived mostly on her own, but was unfortunately hit by a bacterial cystitis two years ago. She didn`t recover for weeks, had to move back home and was housebound/ often bedbound since then.
We started Oxaloacetate, which helps a little bit. We added a TVNS:device, which helps a little bit. She takes some supplements. She weatrs compression socks for upright activities. She stays hydrated and drinks a lot. Everythings helps a little, but not enough to get some life back.
Without showing the typical GI-symptoms, we didn`t think about MCAS. This summer we started MCAS treatment out of despair. Starting with Levocetirizin 10 mg, her joint pains dissappeared within days. In the following weeks we added Ketotifen 1 mg 2xd, Quercetin 1g 2xd, Famotidin 20 mg 2xd. Over the weeks she improved in a surprising way, so in October she was even taking up 90- minutes- lectures at university twice a week which she had to pause during the last 18 month.
But: Starting lectures were only possible with me driving her to University, waiting outside, driving her home in a reclining seat position, staying in bed pacing afterwords and for the following day, We did this twice a week for a full month. No other “out of bed”-activities were possible. Not really convincing…..
I read your blog. I got very excited. I read more about GLP1. I read patients stories.
I am a pharmacist. I like to rely on studies. My eldest daughter is a physician. She prefers studies , too. We talked and decided to give it a try. My youngest daughter was in a really poor condition and we wanted to give her a chance.
Four weeks ago my younger daughter got her first 0,25 Tirzepatide injection. Nothing remarkably happened.
The following week we increased the dosage to 0,5 mg of Tirzepatide. It was on “crash day”, the day after lectures at university. A few hours after the injection my daughter felt “kind of strange”: the exhausted feeling was gone, she was almost feeling “normal”, not at all the feeling she should be experiencing the day after exhaustion.
Now she is feeling so much better. She is able to concentrate for a much longer time. Lectures aren`t so exhausting any more. She even drove to university on her own by bus twice “just to try it”. She is way more active, sitting and walking a lot, she feels less exhausted, the brain fog is much improved.
Two weeks ago (after two weeks on Mounjaro) she took part in a family birthday meeting, which was exhausting but a lot of fun after being mostly isolated for so many months. This weekend she met with friends and even went to a christmas market! No big crash!
Tirzepatide does amazing things for my daughter. We are going to experiment with the dosage and we will see what happens. 0,5 mg has so far no negative side effects, no weight loss, no nausea.
We use an insulin syringe with a Mounjaro vial which wont`t be available much longer in Germany. We will then continue with the Mounjaro kwikpen and count the klics.
So far, Tirzepatide is the best medicine and the best help for my daughter we ever had. I cant`t describe the change this drug is doing. I am constantly reminding her to keep on with pacing, to be careful, to not exaggerate. But at least some life seems to be possible for her!
I decided to report our story because for me it is so important to read about the experience of other patients.
Thank you so much for your blog! You have a huge impact on our success story!
Isn’t that something! Thanks so much more sharing that. 🙂 So nice to see this coming from two members of the medical profession 🙂
Hi Simara — so glad to hear of the positive response to Tirzepatide for your daughter. Following on around 1 month after your post: Can I ask if she has continued at the 0.5mg, if it is at the 1 week dosage interval (or less?), and if the benefit has continued?
Thank you in advance!
Hi SP,
we are still experimenting with the dosage and it is getting even better. My daughter went up to 0.75 mg once a week and noticed a “CFSish” feeling coming up around day 5. After watching this repeating recline for three weeks without seeing a reasonably action causing it, we yesterday decided to go up to 1,0 mg. It will be interesting to watch day 5.
Tirzepatide so far makes life SOOOO much better!
My daughter is much less exhausted and it is much easier for her to follow 90 minutes lectures at university twice a week : she now gets tired only during the last ten minutes (I would think that this is the case for most of the other students, too) instead of getting in brainfog trouble after 30 minutes. She doesn’t have to rest afterwords and the following day. She embraced christmas activities with lots of family and lots of noise wholeheartedly without any crashes.
She went sledding for an hour and had much fun in the snow. She went to thermal baths for over two hours and just loved it.
We will go and buy her a new ski jacket and she is dertermined to use it!
Tirzepatide thankfully makes a huge difference for my daughter. We will try higher dosages because it would be a pity if the results with a lower dosage around 0,75-1 mg weekly would leave her at a Bell-Score around 40-50 (which is fantastic compared to her life with a Bell-Score around 20-25) when even more quality of life might be possible.
As a pharmacist I have no problems with experimenting and finding out what is the right dosage. Every individual reacts differently. We are still far away of the starting dosage for weight loss (2,5 mg), haven’t seen any side effects so far and are very curious to go on with this fantastic journey.
It is a balance between risks and benefits. so far we have so much benefits!
It is such an overwhelming joy to see her life come back!
Hi Simara,
It’s exciting to read about your daughter’s improvement. That must be so lovely for your whole family!
I’m wondering if her improvement is persisting. One of my fears about trying a new medication is that I will eventually crash from cumulative activity over many weeks, even if I’m feeling well enough at the time to do things. Is your daughter’s improved health holding up over these 4 months?
Thanks so much for sharing your story!
Hi Agatha, my daughter’s improvement is definitely persisting. She is right now at 1,25 mg of Tirzepatide every six days, has no significant weight loss and no significant side effects. She has lost her “extra stomach for sweets” after lunch. She experienced an infection with some virus which is normally a small catastrophy for some weeks but it only lasted a few days. That was really interesting to watch; her immun system has obviously improved. She is much more active, enjoys her new freedom, tries to improve her strength with yoga. She is careful with her pacing and is integrating time for meditation and transcutan vagus nerv stimulation in her daily routine. There was no big crash since starting with GLP1. She definitely had situations which were very exhausting (yes, she went to her exam in software engeneering and absolutely rocked it!) and that would normally have led to a bigger PEM-episode, but Tirzepatide seems to lower the intensity of a crash and to shorten the exhaustion. Of course it is very tempting to test the limits, but I’m glad she is mostly very cautious.
We will go skiing next week, and I don’t know what the snow will do to her cautiousness……
So far there was a lot of cumulative activity during the last weeks. I believe it is very important to keep a good eye on pacing, even if it is very hard to be careful with the new possibilities of life. She isn’t cured, but it is a huge change. I hope and pray that this success with tirzeptide will persist .
Thank you so much for replying. I’m delighted to hear your daughter is doing so well. It will be wild if she can actually ski safely! The changes you describe are truly remarkable.
Hearing such a detailed account helps me a lot with my decision-making about GLP1, because I can tell that your daughter’s illness behaves very much like my own, with all the reclining, pacing, planned days in bed, brain fog, prolonged recovery from infection, etc, plus the (mild) helpfulness of hydration, compression socks, and TVNS. Based on this story and other reading, I am going to go forward with requesting a prescription from my doctor. Thank you so much! Sending best wishes to you and your daughter!
Hi Agatha,
mission accomplished: skiing was great, my daughter took her chance on four of six days, reduced relaxation to two days because the sun was shining and the mountains were calling very loudly. It was a relaxed kind of skiing: a lot of resting with apple strudel and enjoying the view, but she was actually skiing. (Mostly bedbound and sensitive to sunlight 9 month ago….)
What is the notable difference since starting with tirzepatide:
She can tolerate and enjoy sunlight
She can be in an upright position for many hours (with compression stockings)
She can be physically active without crashs
She can tolerate and participate in noise, discussions, games
It is such a huge change for her.
i hope you will have similar improvements when you start your medication. Don’t forget pacing, and enjoy!
Best wishes, Simara
Oh Simara,
Thank you for your message! I am sitting here with tears of happiness for you and your daughter. That is such wonderful news. I hope and pray this improvement continues. It’s a terrible disease, but especially terrible when it steals so much from a young person.
I am seeing my doctor later this month, and I feel pretty confident she will help me with a prescription. Is your daughter still on 1.25 mg?
Thank you so much for keeping me updated!
Best, Agatha
Agatha, isn’t it nice that we can have happy tears? Isn’t it nice that CFS helps us to believe in wonders? That’s the first positive side-effect of this awful desease.
My slim daughther is on 1,25 mg every five or six days, that makes 1,75 mg of Tirzepatide a week. We will rise slowly, and see what happens. When she feels a little bit “CFSish” on day five or six, she takes the next shot. Even if she should drop a little bit of weight on the way to a healthier life, I will happily support her shopping trip for smaller sizes.
Agatha, you will rock it! Stay positive!
Best, Simara
Hello again, Simara! I hope your daughter is continuing to do well! I would love an update on her dosing and her progress. I am finally starting tirzepatide on Monday. I am planning to start with a dose of 0,5 mg and increase by 0,5 mg weekly, up to 2.5 mg. Do you think there are any downsides to that approach? I am overweight (20+ years of inactivity will do that), so I’m looking forward to perhaps dropping some weight as well. Please let me know how your daughter is doing. I think of you and your daughter often, hoping you are well!
Hi Simara,
Great to hear of your daughter’s improvements. Thanks for coming back to report on them 😃
I hear people who feel the benefits taper off over the course of a week take Mounjaro twice a week instead of once.
Have you tried this twice a week approach with your daughter? It might work better than continuing to increase one dose.
I hope she is doing well and you are too. I have ME and so does my 18yo daughter now (as of this year), so now I have to think of her as well as me, making a miracle even more desirable!
I’m going to be the family guinea pig and start Mounjaro myself next week. Wish me luck!
Wishing your daughter ongoing good health x
I have been following Cort’s blog for a long time but I’ve never commented. I am an orthopedic surgeon who has had MECFS for 11 years after a respiratory virus. The same thing happened to my brother who is an Internal Medicine physician. Like most of you, I have tried many different treatments including Mestinon and rapamycin. I did not get any long standing relief, although I will probably retry rapamycin at some point.
I recently had to do a cardiac stress test on a treadmill and had multiple out-of-town guests that put me in one of the worst crashes ever. It had been going on for two months. So after reading this blog, I decided to try Tirzepitide. I am doing .25 mg weekly. After the third dose I was out of my crash and back to baseline and the heavy malaise that I call my chemo days because it feels like someone’s injecting me with chemotherapy has lifted. The results really felt palpable. It is early and we all know that sometimes the effects are not sustained, but I am hopeful and the risk profile seems very low.
I just wanted to share this in case others wanted to follow suit and also express how grateful I am to Cort for this blog. I have gotten most of my ideas for treatment from his posts even as a physician. It has also been a great source for sharing stories and providing hope. I know some get discouraged and feel that these treatment stories provide false hope after trying so many different solutions with very little established guidance. It can be very overwhelming and discouraging. I would just say that I feel hope keeps us going and until the scientific community catches up, which I do think is occurring after Long Covid, we need to stay hopeful and share our experiences to help one another.
THanks so much Rob for your kind words. Conratulations on your success thus far! May it continue and thanks for sharing it 🙂 I’m looking forward to trying it.
Thank you for posting this information. I was wondering whether you are able to update as to whether it has continued to help.
Sarah, thanks for checking in. I continued to increase my dose and got significant heartburn that was keeping me awake at night. As I went up in dose, I did not see the same effect as early on. But I confused the issue by also starting on rapamycin. Still unclear of the result of the new drug. I guess my advice would be what was previously mentioned in some other posts regarding the GLP ones; more is not necessarily better and maybe keep the dose very low at the beginning. I stopped it completely due to the G.I. upset but will probably return to it again.
Good morning, Agatha! Great news, that you will start with GLP1-RA! 0,5 mg starting dose sounds good, but I would be really careful with going up with the dosage too fast. Maybe you should wait a little bit longer with higher amounts of tirzepatide. But you will find out for yourself how you react, and you can decide wether it is already time for a little bit more of happiness:)
My daughter has reached 2,5 mg by now, once a week, is very stable and content and embraces life. She is not completely healed, but is in a surprisingly good condition. We have stopped feeling anxious when she is doing “normal” things, and that is a really nice experience.
I am so happy for you that you can start! I hope it works for you soon. Keep us updated! Best regards, Simara
Hi Abz guinea pig :), so sorry to hear that you are fighting this desease as a duo! My daughter isn’t very strict with the timeline of dosage. Tirzepatide has a halfline of 5 days: after 5 days there is still half the dosage in your body. She had the first noticeable symptome relieve at 0.5 mg, only a few hours after injection. The positive effect faded off after five days, and we decided to go by that timeline: new dosage after five days or when the positive effect slowed down. Then we increased the dosage slowly and could stretch the good days. She is now at 2,5 mg every 7 days, helps herself to an earlier shot if necessery (she won’t do exams on fading tirzepatide), and she enjoys all the new possibilities that her new life offers: much less brainfog, more strength, a lot more active time, stronger immun system). She isn’t completely fine, but she can do a lot. I hope it will work for you (and maybe for your daughter, too!) Best regards, Simara
Does anyone have links to the studies referenced or the protocol these doctors are using? I’m wondering how fast they titrate the dose up, and where they start and what the maintenance dose is.
Hi Everyone, I’ve had ME/CFS symptoms since 2020, Tomorrow, I will do my fourth injection of Zepbound at the initial 2.5 mg dose. Congratulations to all who have had good results right away. I’m wondering if others have experienced increased fatigue during the early stages of taking GLP-1s.
Thanks.