


The “Long COVID involves activation of proinflammatory and immune exhaustion pathways” study had almost EVERYTHING. A top research group from Harvard, a comprehensive testing regime (immunological, virological, transcriptomic and proteomic analyses (!), four different cohorts, and … compelling findings. It even had a separate validation arm.

The findings seem to be cohering around a general theme – overactive and exhausted systems – in this case, the immune system.
The only thing it was missing was size. Even though the first part of the study had 142 participants, the four cohorts knocked the size down in each cohort (uninfected controls (n = 35), acutely infected individuals (n = 54), convalescent controls (n = 24), and patients with LC (n = 28). The validation study had a nice time lag (2-3 years) and contained healthy controls (n = 20) and patients with LC (n = 18).
Does it matter? My guess is that it doesn’t. The small validation study with a different cohort was successful, and these findings align so well with prior findings that we can only assume they’re correct.
 Health Rising’s Quickie Summer Donation Drive is On!
Health Rising’s Quickie Summer Donation Drive is On!One of the takeaways from this study is that the research seems to be zeroing in on key themes in long COVID and ME/CFS.
Results
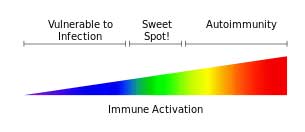
It seems that everywhere we look – whether it’s the brain, or the muscles, or the immune system – we see the same pattern: a system on alert but is too exhausted to deliver – and that’s what they found in long COVID.
First, they found evidence of immune activation in spades. Increased proinflammatory cytokine signaling, activation of the complement system (think innate immune system and mast cell activation), and immune exhaustion suggested that the immune system had put the pedal to the metal.
THE GIST
-

The JAK inhibitor trials aim to calm the immune activation which may be producing fatigue and other symptoms.
The “Long COVID involves activation of proinflammatory and immune exhaustion pathways” study had a lot going for it: a top research group from Harvard, a comprehensive testing regime (immunological, virological, transcriptomic, and proteomic analyses (!), four different cohorts), and it delivered!
- It seems that everywhere we look – whether it’s the brain, or the muscles, or the immune system – we see the same pattern in these diseases: a system on alert but is too exhausted to deliver – and that’s what they found in long COVID.
- First, they found evidence of immune activation in spades but a certain kind of immune activation. The early immune system – the innate immune system – was jacked up and producing lots of inflammation – while the later appearing adaptive immune system (T-cells) was exhausted.
- We don’t know why this is happening. It could be that the coronavirus or pieces of it, or an immune system that’s gotten locked in an activated state, is driving the activation and ultimate exhaustion. Some researchers believe that the innate immune system is activated in an attempt to compensate for the failure of the adaptive immune system.
- In any case, it appears that people with long COVID are: a) stuck in an inflammatory state; and b) have difficulty clearing any pathogens that are present.
- While the amino, fatty, and bile acid metabolism, as well as CRH activity, were at odds with some ME/CFS findings, they point to similar themes driving both diseases. The findings in ME/CFS could reflect a metabolic collapse that takes time to manifest.
- Plus, the study found evidence of epigenetic changes produced during infection that locked immune and metabolic cells into a chronic state of dysregulation.
- Other analyses suggested that premature immune cell aging and genetic instability were present. This was perhaps not a surprising finding in exhausted cells, and other studies have found evidence of premature aging in ME/CFS.
- The end result is a system that’s depleted on many levels – exactly what we’d expected in one of the most functionally debilitating diseases on the planet.
- Several analyses suggested that high levels of inflammation during the initial infection start long COVID off.
- Even before this study was published, the Harvard group initiated a placebo-controlled, randomized trial of the JAK1 inhibitor abrocitinib for long COVID. The JAK/STAT pathway, which upregulates numerous pro-inflammatory cytokines, was found to be activated in this and other studies.
- This trial is one of three JAK1 inhibitor trials currently underway in long COVID (!). One of those trials feature Rinvoq, a drug that quickly returned a severely ill ME/CFS patient to health. Once again, we see long-COVID research leading to trials of potent immune drugs that clinicians have long sought to evaluate in ME/CFS.
- Several studies suggest that this pathway may be activated in ME/CFS and fibromyalgia as well.

Donation Drive Update

If showing how research is driving new clinical trials supports you, please support us.
Thank you to the hundreds of people who have contributed to Health Rising, bringing it to over 40% of its goal!
This blog represents a core commitment of Health Rising: to link the research findings to the clinical trials they’ve inspired. I didn’t know that long COVID was in a JAK1 inhibitor clinical trial boom until I looked – and there it was. That’s a signal that the medical research field is taking long COVID seriously enough to try potent immunotherapies.
This represents a paradigm shift in how post-infectious diseases are viewed, and findings from respected research groups are driving it. That suggests it’s only a matter of time before the same studies and the same drug trials show up in diseases like ME/CFS, FM, and POTS. If you appreciate reading about how research is translating into new clinical trials, please support us!
HEALTH RISING IS NOT A 501 (c) 3 NON-PROFIT
The key factor may be inflammation. While that’s not exactly news, the ability to document it and trace its origin is. (Hence, the immune drug trials are underway.)
Interestingly, that combination tends to result in a sleepy, somnolent, underactive adaptive immune system. (The adaptive immune system (T and B cells) kicks in later to clear pathogens.) Indeed, the reduced activity of a factor called granzyme B that T-cells use to kill infected cells suggested that the T-cells in long COVID were exhausted.
Because the innate immune system produces so much inflammation, while the adaptive immune system clears pathogens, long-COVID patients appeared to have the worst of both worlds. They have too much inflammation, but can’t clear or fix whatever is activating their system.
The next finding – chronic upregulation of IFN-Y which correlated with reduced T-cell activation and increased T-cell exhaustion – clinched it.
Thought of as a key danger molecule, IFN-γ levels rise during an infection as they alert T-cells that danger is present. That works great for a couple of weeks, but when signals to activate keep coming at them, T-cells do what we’ve seen other cells do. They start larding the surface of their cells with inhibitory receptors and start to shut down. The high IFN-y levels in the long-COVID patients – some of whom had long COVID for years – indicated their immune systems were still on alert.
An earlier Cambridge study proposed that the high IFN-γ levels they found, in some cases, more than two years later in long COVID, were highly correlated with fatigue. Those high IFN-γ levels could have been caused by multiple cells (NK, NKT, MAIT), but the study found they were coming from cytotoxic T-cells, which had been turned on by monocytes. A 2024 study found exhausted T-cells that had been specifically produced to respond to the coronavirus, as well as “systemic inflammation”.
The monocyte connection is fascinating, given the Hanson group’s surprising finding suggesting that, of all the immune cells, monocytes – an innate immune cell – are playing the key role in ME/CFS. That study suggested, as did this study, that monocyte interactions with T (and B) cells were particularly important. Bruce Patterson also fingered monocytes in his long-COVID work.
Cytotoxic T-cells triggered by monocytes may be producing high IFN-y levels.
This suggests that the immune systems in long COVID are in a kind of “unresolved war” – an idea that’s been kicking around regarding ME/CFS for quite some time. The early innate immune system is activated (possibly to compensate for a dysfunctional adaptive immune system) while the big guns (T-cells) are turned off.
Whether viral fragments are driving the immune system bananas or whether the system has simply gotten stuck on the “on” position is unclear. Still, these findings suggest that both sides – the innate and adaptive immune systems – are dysregulated, and not in a good way. Inflammation increases while the ability to clear pathogens decreases.
Metabolic Connection
A “decrease” in amino acid metabolism suggested that amino acids – which make up the proteins – and are thought of as “the building blocks of life” had been depleted. Because T-cells need amino acids to get into “action mode”, the reduction in amino acid metabolism could contribute to their somnolent state.
Meanwhile, the increase in fatty acid metabolism – a less efficient means of producing energy than the preferred method of glucose metabolism – suggests that the mitochondria are struggling to use oxygen and sugar effectively.
The amino acid finding was similar, but the other metabolic findings differed in several respects from those observed in ME/CFS. The same themes showed up in both diseases, but in different ways. The increased fatty acid and bile acid metabolism and CRH activity in long COVID were at odds with reductions in these factors in ME/CFS.
It’s possible that, over time, the systems that were upregulated in long COVID become exhausted in ME/CFS. Indeed, Hornig and Lipkin found that duration dramatically affected cytokine levels in ME/CFS.
The Initial Trigger – Inflammation
High levels of inflammation early in the disease appeared to have started long COVID off.
Analyses conducted during the acute infection suggested that scads of inflammation early in the illness started long COVID off. Gene expression analyses revealed early activation of proinflammatory pathways, innate immune cell signatures, and coagulation cascades.
A proteomic analysis (gene expression produces proteins) validated these findings by showing significant increases in proinflammatory pathways (IL-6 signaling, complement cascade, leptin signaling pathway) in individuals who later developed long COVID.
Two more analyses (random forest and feature importance) confirmed what the study had found so far – that activation of the complement system, the proinflammatory response, and the JAK-STAT, IL-6, IL-6-JAK-STAT3, IFNβ, and IFNγ signaling pathways set the stage for long COVID.
Additionally, the study found evidence of epigenetic changes (chromatin regulation and DNA methylation) triggered by the infection that locked the immune and metabolic cells into a chronic state of dysregulation.
Genetic Instability as Well
Gene repair mechanisms did not appear to be working.
Things got a little more harrowing with the telomere findings. The decreased telomere maintenance, DNA damage recognition and repair, chromatin regulation, and DNA methylation found suggested that premature cellular aging and genetic instability were present. That’s not anything anyone wants to hear, but it’s no wonder that “exhausted immune cells” would look older than expected, and, indeed, reduced telomeres have been found in ME/CFS before.
This genetic breakdown may occur when oxidative stress generated by chronic inflammation degrades DNA. If our already depleted cells can’t repair that damage, they commit suicide (apoptosis) and need to be replaced, which takes up more energy, which we don’t have.
The result is a system that’s depleted on many levels – exactly what we’d expected in one of the most functionally debilitating diseases on the planet.
Striking at the Root?
These findings probably wouldn’t have spurred a clinical trial in ME/CFS, but they sure did here. Once again, we see long-COVID research triggering something we’ve almost never seen in ME/CFS – strong immune drug trials.
The JAK inhibitor trials aim to calm the immune activation which may be producing fatigue and other symptoms.
Even before this study was published, the Harvard group initiated a placebo-controlled, randomized trial of the JAK1 inhibitor abrocitinib for long COVID. This drug’s ability to target early stages of the JAK1 pathway may help calm a hyperactive immune system.
The study, which began in December of last year, is assessing several doses (50, 100 mg) in non-hospitalized (yah!) adults with long COVID over 12 weeks. In a nice sign, Pfizer agreed to provide the drugs.
It’s no longer recruiting and is expected to complete in mid-2026. The trial is part of a JAK inhibitor boom currently taking place in long COVID (LC).
The “Citinib” Boom in Long COVID
These drugs are able to tamp down the JAK-STAT pathway and reduce IFN-γ levels.
In August, the Sick Times (who else?) reported in “Three clinical trials for Long COVID are testing JAK inhibitors to treat immune dysregulation” that two other JAK inhibitor trials are underway in LC. Health Rising has reported on the big Baricitinib LC trial many times. This trial is notable for the substantial resources being invested in it and the high expectations for this drug.
The LC-REVITALIZE trial may be the most curious one, though. It features Rinvoq (upadacitinib), a drug that returned a severe ME/CFS patient to health. This trial, which is also assessing the anti-inflammatory drug pirfenidone, came out of Western University in Canada (which is in western Ontario – not western Canada :)). It plans to assess patients in, get this, Brazil, Canada, Italy, Uganda, Zambia, and the United States. (It’s currently recruiting in Canada and the US in San Diego. See the link for contacts.)
Note that these are very strong drugs that can result in, among other things, infections and cardiovascular problems. Anecdotal reports indicate that some patients can handle them and may do better, whereas others cannot. A major goal of these trials is to identify who benefits and who does not.
Possible ME/CFS and FM Connection
ME/CFS researchers have been interested in the JAK/STAT pathway in ME/CFS or quite some time. The Sick Times (which does its homework!) pointed out that Vincent Lombardi received a Solve M.E. Ramsay Award to study the JAK pathway in ME/CFS back in 2018 (!). Lombardi is apparently still plugging away at his work.
While there’s no definitive evidence linking ME/CFS or FM to JAK/STAT signaling, several studies point in that direction.
Conclusion
This study had an awful lot. Inflammation took center stage with the high levels of innate immune activation and evidence that high levels of inflammation during the initial infection triggered long COVID. The collapse of at least a major part of the adaptive immune system suggested that the immune systems in people with long COVID were both activated and exhausted – a common theme in both long COVID and ME/CFS.
Amino acid, bile, and fatty acid metabolism – three common themes in ME/CFS – were dysregulated (although in different ways) in long COVID.
Quickly jumping on their findings, the Harvard researchers joined an ever-growing JAK/STAT inhibitor club. Thus far, these powerful immune drugs, which aim to tame immune system overactivation, are the subjects of three long-COVID clinical trials.
While there is no definitive evidence that the powerful JAK/STAT pathway is activated in ME/CFS or fibromyalgia, several studies indirectly point in that direction.
Donation Drive Update
If showing how research is driving new clinical trials supports you, please support us.
Thank you to the hundreds of people who have contributed to Health Rising, bringing it to over 40% of its goal!
This blog represents a core commitment of Health Rising: to link the research findings to the clinical trials they’ve inspired. I didn’t know that long COVID was in a JAK1 inhibitor clinical trial boom until I looked – and there it was. That’s a signal that the medical research field is taking long COVID seriously enough to try potent immunotherapies.
This represents a paradigm shift in how post-infectious diseases are viewed, and findings from respected research groups are driving it. That suggests it’s only a matter of time before the same studies and the same drug trials show up in diseases like ME/CFS, FM, and POTS. If you appreciate reading about how research is translating into new clinical trials, please support us!
HEALTH RISING IS NOT A 501 (c) 3 NON-PROFIT


This really seems to reinforce that immune dysregulation is at the heart of this illness. The underlying trigger remains the million-dollar question, but it’s encouraging to see solid research translating into clinical trials so quickly. More of this, please! )
Yep.
I have long been skeptical of chronic viral
Involvement in ME/CFS – strongly favouring a viral ‘hit and run’ theory. But I have come around to the idea that viral reactivation is quite a plausible explanation.
I am interested in seeing how PolyBio go with their antiviral studies.
I also understand that there might be further studies on Inspiritol which has showed some promising initial results.
Inspiritol seems to be just a combination of different supplements and herbs: glutathione, methylcobalamin, N-acetylcysteine, eucalyptol (1,8-cineole) and β-caryophyllene.
Yes, but the mode of delivery could make a difference. Also, some of those substances are not readily available. Finally, the substances might be working in combination in some effective way, synergistically.
Sure. But like I (and many others) have seen in the past, many times these are just marketing and for profit, charging 100-300$ for a single bottle of simple ingredients. And studies made by the manufacturer where even 1% of temporary improvement is marked as “symptom free”.
But hopefully I’m wrong this time and this will be something that does lead to a considerable improvement in symptoms and the price will be right.
I took all of those individually for years, orally, before I went into remission. They are all readily available. Glutathione, Vit B12, NAC, Ginger and CBD. 🙂
I also found that taking Solgar amino acids helped my fatigue. 🙂
Don’t forget that an overactive autonomic nervous system suppresses the immune system, which can allow the reactivation of viruses, especially herpes viruses, to become (partially) active. The immune system then becomes exhausted because it becomes overstimulated, as has been proven. Conversely, I am not aware of any infections that cause the autonomic nervous system to become overactive.
I’m not sure whether the problems with the autonomic nervous system that some people have with ME/CFS are actually a good starting point to understand pathomechansims.
It is only a minority who has POTS and similar problems.
Plus, you can have some form of Long Covid with POTS but not be an ME/CFS patient.
I therefore wonder whether autonomic nervous system problems are spefically a result of certain infections like Covid and others that can also lead to ME/CFS.
Have you seen this study Cort?
https://link.springer.com/article/10.1186/s12967-025-07507-x
I hadn’t. Thanks for the link 🙂
Would this mean that there is something underlying that is maintaining the immune reaction or the initial trigger left the immune system “stuck” in an activated mode?
I hope is the latter as this would be easier to address than looking for the underlying cause for each ME/CFS case, that also wouldn’t explain why some people get ME/CFS due physical trauma.
What would happen when the patient stop taking the JAK/STAT inhibitor? Does the disease come back or the improvement remains?
“There is something underlying that is maintaining the immune reaction or the initial trigger left the immune system “stuck” in an activated mode?” It could be either one. There’s evidence that pieces of the virus are left in some long COVID patients and this study found evidence of epigenetic changes that could have gottethe system stuck.
I assume the symptoms would come back but don’t really know.
I got ill after a non COVID, traditional vaccine. Would that mean I am screwed if the vaccine antibodies are what is maintaining the illness or that is more asking to an initial trigger and stuck state?
More excellent research, this time from Precision Life, which points to some treatment possibilities. Ending the year positively!
https://www.medrxiv.org/content/10.64898/2025.12.01.25341362v2.full-text
Yes – what a nice summation in the abstract !
“These findings allowed identification of many existing and novel repurposing opportunities, including candidates linked to several genes with shared etiology for long COVID.” 🙂
Let’s hope they’re on the right track!
Thanks for this. I’m in daily conversation with Grok for performance monitoring. I fed him this article and we’re making a couple of changes: increasing black seed oil to 2 tsp/day and increasing Pure Encapsulations Hist Reset to 8 capsules/day. Loved all the details he provided as to what would chemically be impacted (JAK/STAT support, strong mast/JAK synergy). Grok is now my primary medical advisor. I take his recommendations (with evidence/studies) to my practitioners.
I’ve got the JAK2 V617F mutation it showed up in my direct to consumer DNA tests when I uploaded them to Promethease.com
Great article Cort — thank you. This study used INMEST (intranasal mechanical stimulation) to vibrate in the nose at a specific frequency which induces a nerve reflex to the vagus nerve nuclei in the brainstem. This in turn improved “disease tolerance” resulting in less inflammation and a 30% reduction in symptoms in ME/CFS.
https://www.biorxiv.org/content/10.1101/2020.02.20.958249v1.full.pdf
So it ties in many themes discussed in Cort’s recent posts: overactive immune system (or, chronic inflammation), brainstem and autonomic nervous system. Interestingly, the treatment caused a reduction in heart rate variability which suggests an increased sympathetic action — also a recent topic of late.
Seems any treatment that can calm an overactive, overly sensitive immune system would be a worthwhile adjunct to other treatments. And by working on the higher centers of the brain, a resetting effect appears to be more lasting than other vagus nerve stimulating methods.
Interesting! Thanks! 🙂
When I first read of INMEST, it reminded me of epipharyngeal abrasive therapy (EAT). EAT also impacts the brainstem via mechanical and chemical (zinc chloride) stimulation of vagus nerve endings in the epipharynx.
In doing so, EAT balances/improves autonomic nervous system function, reduces systemic inflammation, modulates the immune system and thus, the HPA axis (another recent topic of yours).
So it isn’t surprising that EAT can be effective in POTS, LC, autoimmune conditions and ME/CFS when epipharyngitis is present. Interestingly, though, it has also been found effective (especially in LC) when clear epipharyngitis is not present. Meaning, subclinical or microscopic inflammation may be there, but obvious visible inflammation is not (and so, may easily be missed if it’s even checked for in the first place).
https://pmc.ncbi.nlm.nih.gov/articles/PMC12476287/#:~:text=EAT%20has%20been%20reported%20to,the%20innate%20immune%20control%20mechanism.
From the above study…
“A review of the existing research literature shows that EAT stimulates the autonomic nervous system through changes in parasympathetic activity mediated by the trigeminal-vagus reflex and has an immediate effect of inducing inflammatory reflexes. In addition, as a long-term effect, the autonomic nervous system balance is reestablished due to changes in the plasticity of the reflex pathway, chronic inflammation is controlled, and the immune response is normalized. Furthermore, continuous EAT stimulation influences the immune and endocrine systems, leading to the resynchronization of the body’s homeostasis network.”
It seems the nerve endings/branches in the nasal area are an effective target for positively impacting the limbic system and ultimately the overactive immune system and more.
Also like INMEST, EAT appears to improve sympathetic nervous system function…
https://www.jstage.jst.go.jp/article/ans/61/2/61_159/_article
so exciting information maybe there is hope for me! Covid took my life as i knew it
thank you so much
i am a physician who got it from a patient first couple times
anyway i can help let me know and i am in a long covid clinic and hope i have access to meds
my dr raised just my Estrogen dose to fight inflammation after my last covid in December 2035 hope it helps!