


At the 2020 IACFS/ME Zoom Conference, Marvin Medow spoke on a recent study, “The Benefits of Oral Rehydration on Orthostatic Intolerance in Children with Postural Tachycardia Syndrome“.
The study produced an unusual finding for this field – a potentially relatively cheap and easy source of help.
The Study
The study involved 10 patients with POTS and 15 healthy controls. Most of the POTS patients also met the criteria for chronic fatigue syndrome (ME/CFS).
Postural orthostatic tachycardia syndrome (POTS) refers to a condition which produces increased symptoms, racing heartbeat, reduced stroke volume and blood flows to the brain upon standing. Along with the low blood volume found in POTS, POTS patients have another problem – their blood tends to settle in their abdomen and lower body when they stand, reducing blood flows to their brains further. POTS is not uncommon in ME/CFS and can often be ameliorated by increasing blood volume.

Medow used a lower body negative pressure (LBNP) technique to simulate a tilt table test (TTT) over three days. Air pressure was reduced until the participants were feeling faint, asked that the test be stopped, if their blood pressure fell too far, or if the test was concluded after 50 minutes. All the participants made it to a -45mm of air pressure for at least two minutes.
The participants were given the World Health Organization (WHO) oral rehydration solution (ORS) containing glucose (dextrose) (1 liter over 30 minutes) or a saline intravenous (IV) therapy for 30 minutes prior to the LBNP test.
Results
At baseline – without being given saline IV’s or ORS – the POTS patients had 30% of the orthostatic tolerance of the healthy controls.
While studies indicate that saline IV’s are helpful in POTS, the big winner in the study was oral rehydration solution (ORS). Both saline IV’s and ORS were effective at maintaining blood press and both significantly improved orthostatic intolerance (as measured by the orthostatic index) – with the ORS being a bit more effective.
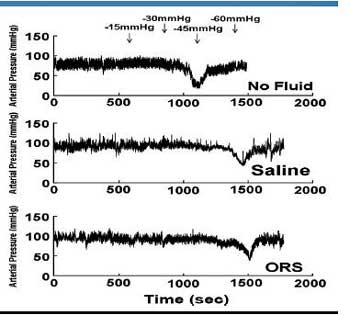
The effects of saline and ORS (bottom two) on blood pressure. Both delayed the blood pressure drop significantly.
Saline IV’s were not effective, though, at increasing blood flows to the brain, increasing cardiac output, and mean arterial pressure. ORS, on the other hand, improved all three – and normalized cerebral blood flows to the brain. That may be quite significant as recent studies suggest that virtually everyone with ME/CFS experiences at least some reduced blood flows to the brain upon standing (or, in some cases, sitting).
Studies indicate that saline IV’s help with POTS, and anecdotal reports of the help they provide to POTS and/or ME/CFS patients are common, but this small study suggests that oral rehydration solution (ORS) may be more effective. It was remarkable to see a relatively cheap and easily available ORS solution prove more effective in this study. The authors concluded that:
“Because ORS is inexpensive, safe, and easily administered, it may be considered an effective alternative to IV saline for rapid resolution of symptoms associated with orthostatic intolerance.”
Why might an ORS provide more benefits? While saline IV’s and ORS both increase blood volume, they do so in different ways. The authors suggested the ORS may be producing a “gastropressor effect or response”, which increased blood pressure, thus helping maintain blood flows to the brain.
Oral Rehydration Solution
The ORS Medow used derived from the World Health Organization formula and contained glucose (dextrose) – not sucrose. Plus it’s vital that the ingredients be combined in the specific portions specified by the WHO.
The glucose/salt combination creates an osmotic gradient consistent which produces “nearly complete fluid and salt absorption via the intestinal Na+-glucose co-transport (GLUT2,symporter) carrier”. Sucrose, it should be noted, does not produce the same effect – many commercial oral rehydration or electrolyte enhancing solutions use sucrose.

The oral rehydration salts from the Jianas Brothers are the cheapest option – if you buy directly from the company.
The ORS recipe Medow uses has proved lifesaving in cholera and other diseases that produce severe diarrhea. Medow recommended using Normalyte or an ORS solution from the Jianas Brothers. He cautioned against buying the Jianas product on Amazon as it is extremely expensive (almost $4/packet). Instead you can buy it direct from Jianas Brothers for 55 cents/packet (plus shipping). Trioral on Amazon also uses the WHO formula (86 centers/litre). I tried it and it works really well. It’s quite cheap when you buy several months supply.
Six packs of Normalyte (two packs per liter of water) cost $8.99 at Amazon. You can buy Normalyte Pure (without additives) in bulk at the Normalyte website (buy 10 and each pack costs $7.19)
David reports that in Canada MEC’s Adventure Medical Kit Oral Rehydration Solution (3x 1litre solutions for $8.75CAD on mec.ca) a good option. David states that MEC contains the original pure WHO formula with no additives and at a higher concentration than Normalcyte. (The original recipe may have more glucose than the updated one.) If you spend over $50 shipping is free.
There is a potential catch – 20 grams of glucose per liter of water. One person in the question period asked if the amount of sugar (glucose) in the ORS solution could pose a problem for people with ME/CFS. Medow didn’t think this relatively small amount of glucose would affect glucose levels, but time will tell how well people with ME/CFS tolerate it.
ORS solution may not need to be taken every day, though, to have an effect. A 2017 study found that simply giving saline infusions (between 1.1 and 2.1 L) every 10 days or so for three to six months dramatically improved the symptoms of young women with postural orthostatic tachycardia (POTS – increased heart rate during standing).
Making the World Health Organization ORS Solution?
Commercially available ORS contains sodium chloride (3.5 grams), potassium chloride (1.5 grams), trisodium citrate dihydrate (2.9 grams) and dextrose (20 grams), all of which is to be added to 1 liter of water.
It is possible to make the solution yourself. Doing so, however, come with a strong warning. Safe sources of dextrose and table salt are easily found. Because some of the other chemicals are used for industrial purposes and contain toxic elements, USP-grade/food grade sources MUST be used if you decide to create your own preparation.
That can be bit tricky. Amazon, for instance, sells potassium chloride that is not food grade. The product description states it’s “used in fluxes, production of other chemicals, heat packs, along with a lot of other uses” – and people are using it as a dietary supplement. Amazon also sells a food-grade potassium chloride (in its industrial and scientific products section) which is actually substantially cheaper – which doesn’t really make sense. Food-grade sources of trisodium citrate dihydrate can be found as well.
All in all, given how sensitive people with ME/CFS are, it’s easier and probably much better to stick to the ORS packets – and use the Jianas ORS if money is an issue.
Other Oral Rehydration Solutions
Many people try to increase their blood volume by adding salt to water. Drinking large amounts of salt water, however, can be dangerous – and Medow reported that “conventional oral hydration” techniques are not effective in improving orthostatic intolerance. Drinking a lot of salt water will cause the water to go into the tissues – not the circulation. Then the sodium has to be excreted – potentially causing declines in potassium.
Many other forms of ORS have been proposed. Dr. Cheney recommended his “Homebrew” formula, which uses no sugar, and a mixture of sea salt and No Salt (available at grocery stores) for those unable to tolerate Gookinaid – now called Vitalyte – which is glucose-based and contains fructose, potassium and sodium chloride, as well as some other factors.
This recipe uses water, salt and regular sugar. The Rehydrate website also recommends water, salt and table sugar. Hydrant – a fancy rehydration mix – uses sugar as well. – Medow would presumably not approve of any of these.
Conclusion
The World Health Organization’s glucose based oral rehydration solution is mostly used to prevent dehydration in cholera and severe diarrhea but it proved surprisingly effective at improving orthostatic intolerance in children with POTS – many of whom met the criteria for ME/CFS.
The ORS was used to increase the low blood volume in POTS. Blood volume is often low in ME/CFS as well.

By improving blood volume, ORS normalized blood flows to the brain and improved orthostatic intolerance.
While both ORS and saline IV’s were effective at maintaining blood pressure, I liter of ORS was more effective at improving orthostatic intolerance (as measured by the orthostatic index). Only ORS normalized blood flows to the brain, increased cardiac output and mean arterial pressure in the POTS patients.
A recent study indicated that most people with ME/CFS, when they have POTS or orthostatic hypotension or not, have reduced blood flows to the brain.
The authors concluded that ORS is an inexpensive, safe, and “effective alternative to IV saline for rapid resolution of symptoms associated with orthostatic intolerance.”
The one possible catch for ME/CFS patients who are limiting carbohydrates is the amount of glucose contained in the preparation.
The WHO’s ORS solution is composed of glucose (dextrose) and salts. Medow recommended two commercial products: one produced by the Jianas Brothers and another called Normalyte. Several other commercial ORS solutions and recipes use sucrose – which is not effective. Salt water is not very effective at improving orthostatic intolerance and drinking large amounts of it can be dangerous.
It is possible to make the preparation but because some of the factors in it are used for industrial purposes, food-grade sources must be used to avoid possible toxic exposures.
Your Support Keeps Health Rising on the Web



Thanks, Cort, for another great article.
Dextrose is corn derived, a problem fir those of us with corn allergies. Sucrose doesn’t work?
It wasn’t clear if Dr. Cheney’s Homebrew formula would work. It sounds attractive, being without the sugar which works against any low carb diet.
Or maybe using pyridostigmine or Huperzine A to reduce POTS symptoms would head this problem off altogether, negating the need for such a solution?
I was just diagnosed with orthostatic hypotension. Would this benefit me?
This sounds great. I wish they made a version without potassium. I have had high potassium levels for several years so need to avoid extra potassium.
It’s certainly possible. The study found that both the saline IV’s and the ORS raised blood pressure and low blood pressure upon standing is what you have.
Krista, You can try making your own without the potassium. That’s what I do. I make each glass as I go. Dr. Rey at NOVA INIM told me I didn’t need the potassium in the mix because I take a potassium supplement. (I’m starting to wonder about that in my case.) Even without the potassium this is very helpful for me.
2 cups water
1.5 level tsp. dextrose sugar
.25 level tsp. salt
What salt do you use, can pink salt be used? Are you still using this formular
Krista, I buy the dextrose on Amazon. You need twice as much of you use table sugar.
It’s unclear to me both from this article and from the published paper how much to drink of this? Is it 1 liter with the specified proportions (20g dextrose etc.)? Most packets I can find in Europe come per 200ml
I’m sure people are helped by Cheney’s Homebrew – he used it for years. He also really liked Gookinaid – now called Vitalyte – which is glucose based. I have the feeling that Vitalyte was his first recommendation but don’t know for sure.
Honey can be used instead of sugar, and the sugar called for in the “recipe” can be reduced according to personal need/preference.
Food grade potassium gluconate powder by NOW is available.
I was wondering about corn for another reason… GMO‘s… Over 90% of the corn and soy grown in the US is GMO. Do any or all of these products use non-GMO dextrose?
I take pyridostigmine and mix my own electrolyte solution with 1/2 tsp of pink salt and 1 tsp of turbinado sugar in a liter of spring water. I drink approx 4 of these a day. I also need to supplement potassium chloride and do it under doctor supervision. I find it better tolerated with meals. My electrolyte levels are good. It gives me some relief from severe POTS/dehydration symptoms but not from PEM.
Hi Sandra, you might try getting some dextrose (glucose) and see if it makes any difference for you. Also please note that the ratio’s of ingredients are important. I have no idea if yours are on the mark or not – I just wanted to mention that.
Hi Cort,
I got so excited when I read this article. I had tried an IV Saline and felt that it helped me tremendously but only lasted a few days. So this article was very heartening. Except that Jainas is OUT OF STOCK. And to get it from Amazon or elsewhere requires paying a premium, of course. But the biggest issue is that the WHO revised the formula in 2006. The new formula is preferred for pediatric use. It reduces the salt and the glucose. The 1975 formula was primarily intended to prevent death from dehydration and did so very effectively for 25 years, but without stopping the diarrhea right away).
The new formula is highly effective for pediatric use, but as near as I can tell, there is not a consensus for adults who appear to be at substantially higher risk of side effects using the new formula, specifically a potentially fatal condition known as hyponatremia. (But it is noted that in studies it did not cause fatalities, but why have a higher risk at all?).
It appears that the original formula may be safer for adults. So we will see if the original formula will continue to be available. Here is an article explaining why the balance of glucose to salt is really important, and why the new formula may not be optimal for adults. It also includes a handy table provided by WHO showing acceptable guidelines for oral rehydration solutions that are broader than the specific formula of the new product (useful if you are making your own).
https://rehydrate.org/ors/expert-consultation.html
It’s beyond frustrating that we find something that might help us and its really affordable and sure enough it’s been discontinued and become hard to find. The Canadian product and most other brands are using the new formula not the original formula. 🙁 Maybe I am overreacting. 🙁
I take potassium supplements, so haven’t included it in my ORS. Do you think this is acceptable?
These days, I only take an ORS if I am dehydrated. Most of the time I drink a bit of saltwater twice a day.
I have decided to try the Normalyte pure. Although the other product may be more expensive on Amazon, Normalyte is the same $8.99 for six packets on both sites. It does get less expensive if you are ordering in bulk from the Normalyte company and they do have a sampling program. I, however, am impatient and my Amazon order will come tomorrow. Normalyte also comes in a flavored product, but it has Splenda which I can’t tolerate. Hoping for the best.
Good luck! Please let us know how it goes. 🙂
I use Trioral rehydration packets when I feel I’m down a few extra pints. This is the WHO formula and comes in at $0.40/packet. Not an ad, just what I use. 🙂
https://www.amazon.com/Rehydration-Organization-Poisoning-Electrolyte-Replacement/dp/B00OG8G9UM/
Thanks Debbie. That looks like a great product. I will add it to the list 🙂
I use Trioral too. I wonder tho how often I should drink an ORS? I’ve been doing one packet with 33 ounces of water daily.
I like this too. When comparing, note that Trioral packets are designed per cup of water, instead of a liter. I don’t have OI or POTS, but likely have neurally mediated hypotension. Hydration really helps with my moderate condition.
The Trioral linked to is the one I use it is definitely for 1 litre of water
Hi! I was just checking, &TRIORAL seems to have less dextrose & salt than indicated for Normalyte or an ORS solution from the Jianas Brothers. Did I miss something?
TriOral is based on the updated WHO formula.
Will that give you to much potassium?
Thank you Cort!
I wasn’t sure after reading the article- are the Jianas Brothers’ packets as “clean” as the Normalyte packets, or is there a compromise of purity for the lower price?
I don’t know why they wouldn’t be. Maybe some of the price difference could be due to the packaging – Normalyte has a fancier website, packaging? If you get Normalyte you probably want to use the Pure formulation which doesn’t contain additives.
Hi Cory, I’ve purchased the packets from Jianas Brothers. The packets are very sturdy. You cannot rip it open, scissors or knife are necessary. I’m on my second week drinking 1 liter of it out of my 3+ liters I drink daily. I’ll continue and keep you advised on some hopefully positive results.
Best Regards
Lee
Looking forward to hear how it goes. Good luck and thanks!
I’ve used Marty Kendall’s ”Optimised electrolyte mix” for a while:
https://optimisingnutrition.com/electrolyte-mix/
It has a higher proportion of potassium, and adds magnesium which might be relevant for many with ME/FMS/POTS. For me it seems to be much more helpful with the higher proportion of potassium.
As far as I have understood it the mainstream formulas are keeping the potassium low due to some people having imbalances that can make potassium supplements harmful (too dramatic an effect). It seems important to be careful and see how one’s own body reacts to potassium supplementation, but it may be useful for many to use much higher proportions of potassium since most people need more potassium to get the sodium/potassium ratio optimal.
This is exciting!
There is a woman, her site is primarily about MCAS. She has the trifecta (+hEDS, POTS). She takes potassium bicarbonate + sodium bicarbonate (baking soda) as an antihistamine as an antihistamine; she found it greatly helped her POTS as well.
Her site hasn’t been running for a while unfortunately
https://www.mastcelldisease.com/my-new-all-natural-rx/
maybe on the wayback machine ?
(this was from a doctor/naturopath that specializes in histamine/allergies, from what I remember, her name sounds a lot like Cornejas?)
I looked into where to source it from, and found that in Germany this is known as a base powder. Often with calcium, magnesium and zinc added.
That is, to make the pH of the body/cells basic.
https://www.saeure-basen-forum.de/en/acid-base-balance
That made sense to me:
oxidative stress changes the charge of the cell.
I don’t quite follow but the talk of NADH+ and NADH also sounds like a charge problem.
We had a bit of a conversation going on the more recent posts on POTS,
regarding lactic acidosis.
I looked that up and see it has overlapping symptoms with POTS:
“Symptoms of lactic acidosis include rapid breathing, excessive sweating, cool and clammy skin, sweet-smelling breath, belly pain, nausea or vomiting, confusion, and coma. See whether the right amount of oxygen is reaching the body’s tissues.”
I start to wonder:
Is what happens in POTS lactic acidosis? In a subset, in all?
Hypoxia can also be a cause of lactic acidosis.
Some inherited metabolic disorders – the severe and not so severe, the mild when sick – can also present with lactic acidosis.
I myself I’m taking the base powder.
I’m not sure how it’s going, as I may have a transport problem with calcium.
My taurine is my lowest plasma amino acid,
and taking it eliminates the brain fog, and stabilizes my pulse pressure.
One of the things taurine does is modulate calcium in the cell.
So I may need to take both.
I’m still tinkering.
* Glucose I’m not sure about, many of us report having problems with this *
For sure, potassium bicarbonate and sodium bicarbonate can be tried.
Inexpensive, (no side effects?),
http://www.allergynutrition.com/wp-content/uploads/2014/06/Alkaline-salts.pdf
* salt alone makes my nerves go bonkers and my heart flutter…
(feel welcome to dig through the comments on the recent blogs on POTS for a bit more details on the exchange)
I was told by a doctor to drink sodium chloride for POTS. It helped with the POTS symptoms, but I started to get really sick and no one knew what was wrong. I had swollen joints which never happened before and felt like I was being poisoned. One day I decided to add fresh lemon juice to the water and after just 2 days of the lemon juice all of the symptoms subsided. My joints immediately felt better and I no longer felt like I was being poisoned. I googled lemon and salt and found out that people with gout drink fresh squeezed lemon juice after eating because the salt increases their uric acid level. I do not have gout but do have autoimmune problems. Dr klimas mention uric acid testing for something else recently. A lot of doctors will recommend just sodium chloride tablets for POTS and I think people need to be aware.
Salt actually *decreases* uric acid.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5161245/#:~:text=In%20this%20ancillary%20study%20of,systolic%20and%20diastolic%20blood%20pressure.
How much taurine addres you taking, and how often?
Taurine was my lowest amino acid on plasma test.
I recommend getting levels checked out before taking it.
Always be safe and start at small doses – I find the need to remind myself this over and over again.
At last something simple and useful for some. Thanks Cort. A good user friendly summary as always.
Apparently there’s a glucose pathway which pulls water in as the glucose is pulled in. The same thing doesn’t happen with sucrose. I wonder if there are any non-corn glucose products. Also – given that this is just dextrose – I wonder if it’s missing whatever factor is giving you problems with corn. Corn, after all, is made up of different molecules. (???)
I see the packets of ORS on the Jianas Brothers website for 1.10, not 44 cents as stated above. Just sharing as an fyi. Thanks for an informative article, Cort.
I recently bought a package of Hydrant to try it. It’s expensive. You have to subscribe to get a lower cost. I got a discount (I must have subscribed) and paid $30.00 + tax and free shipping. Original price was $37.49. The 30 servings are in individual small packets that you pour into water. I got lime, and it’s tasty because they use actual lime juice powder, tastes like fresh squeezed. Hydrant does come in several flavors.
The Hydrant package says: “Developed by an Oxford scientist, Hydrant provides the optimal blend of electrolytes with just enough sugar to activate your body’s sodium-glucose cellular uptake.”
One small serving contains: 20 calories, 260mg sodium, 6g sugar, 200mg potassium, 30mg magnesium, and 2mg zinc. You’re supposed to drink on an empty stomach first thing in morning, and then you can drink throughout the day. I can’t tolerate on an empty stomach, but I can’t tolerate much of anything except food on an empty stomach. I drink it at other times. I’ve only used a few packets; still have a bunch left. For orthostatic intolerance, I’d think a person would have to drink a few of these throughout the day, and with only 30 packet servings, that might require two or three Hydrant packages. At $30 a pop, that’s way too expensive. I sent them a message saying “If I have a subscription, please cancel.” I can’t afford another ding on my small budget each month. However, I would recommend giving it an initial try if you have a budget that can afford it.
Hi Cort. Thank you for this information. Is there anything wrong with Trioral brand? It says it’s WHO formulated and it’s without citric acid, which I react badly to. Thanks.
Christine,
I use TriOral as well. It uses the formula that WHO recommends for rehydration. The only thing I’ve noticed is that it doesn’t always taste the same-the level of saltiness is different at times. I wonder if the ingredients are not always mixed well. I have found this to be the most cost effective brand with the WHO formula.
As to how much to take for OI, (I have neurally mediated hypotension, not POTs), my doctor recommended 1 liter in the morning and a second in the afternoon if needed.
I need to get back with the program after reading this. With other treatment, my OI is better than it was. I believe that getting my folate levels up to normal helped me.
Currently on Amazon, if you buy a box of 100 packets (1 packet/liter water), it’s 40 cents/packet. By the way, they have a lemon with stevia flavor as well which I thought tasted gross. (I can’t remember for sure, but I think it was super sweet.) The unflavored just tastes like mildly salty water and the flavor doesn’t bother me.
Karen I find the saltiness taste changes even if I make a batch myself(yes I got all the stuff theWHO use from brewers/baking supplies and make the powder). What we worked out is I don’t taste sodium as much when I need it most. ie I can eat VERY salty food or drink salty water and it does not taste salty. The next day I can drink the second half of a litre and it now tastes salty. (I often split into 2 x 500ml bottles and fridge one for later)
It will be interesting to see how one of these products will affect my blood pressure which is high in the morning. This has come on since I am now an older patient. I have POTS and my blood pressure plummeted on tilt table. While PYRIDOSTIGMINE is great for me, it doesn’t do the job fully.
Thank you so much for another great write up, Cort.
Good luck!
Hi Anne, I too, have hypertension unlike many of us who have the opposite. Mine drops when I move too suddenly but it can get scary high, too.
What I remember reading about the IV saline (written by Dr David Bell) was that he tried the IV saline on a patient with high blood pressure and he was nervously pacing the whole time. But as it turns out, the treatment not only dramatically reduced her symptoms of ME/CFS, it also dropped her blood pressure, because the effect of increasing blood volume reduced the need for the body to compensate with higher blood pressure – I think that’s what he said. I have no idea if the same thing happens with oral solution, but I will monitor it, to be sure.
Thanks Cort, just came out of another PEM. I only get POTS during a PEM, but it’s bad. I’ll try this next time.
Interesting. They’ve also found exercise induced POTS -which is temporary as well. Good luck!
Thanks Cort for this, does anyone know if any products are available to buy like this in the UK? It’s hard comparing them all, and I am unsure of what to buy. Are these the same as sport electrolyte drinks?
They are definitely not sports electrolyte drinks – which use usually use sucrose or table sugar instead of dextrose. Look on Amazon.uk for Oral rehydration solution and look for one based on the World Health Organization formula. That one will use dextrose (glucose) for the sugar. Good luck!
Same question for Australia.
Common products used in MECFS Aus community are aqua force and hyradlite sports.
Which I’m not sure they fit the WHO ORS specs.
I gather dextrose and glucose can be interchanged in the incredients?
I don’t know there are these different names but dextrose is apparently the common name for glucose.
https://www.bing.com/search?q=dextrose+vs+glucose&cvid=6b66d67c80d043d3a3cd9e9692652338&pglt=547&FORM=ANNTA1&PC=U531
I believe that dextrose is the name for dried glucose.
There are two forms of glucose, L form and D form. The D form is dextrose, which is the form found naturally in foods and is the form that the body can use. The L form is apparently not something the body can use, from what I understand. So, yes, dextrose is glucose. And dextrose is not as sweet as sucrose, fructose, etc.
I like the comment above where someone found all the ingredients and mixed them up herself!
I just ordered it to belgium, verry easy
Good luck Konjin!
One problem that often comes with POTS is Digestive issues. I was unable for years to drink enough fluids (and salt) to treat POTS. My doctor had me get 3 Saline IVs/week for 2 weeks. (1.5 bags each). Miraculously this helped my stomach so much that I can now drink 2.5 L/day fluid without the pain/ bloating I had before! I also use Liquid IV drink solution and Vitassium Salt pills.
It’s interesting the diverse effects that increasing blood volume can have.
Wouldn’t coconut water if you add salt due the trick?
Does midodrine pills work too?
How long ago was it that you had the IVs? I was much better for several months after a hospitalization that included 48 hours of continuous IV fluids, but the effects on digestion as well as POTS gradually wore off.
I’m still having too many digestive issues to be sure I’m
absorbing oral electrolyes. Magnesium, for one example, gets added to my monthly IV and the impact on my tense muscles is almost immediate that way, whereas very little effect orally no matter how much I take daily in my oral solution
.
Since POTS and other autonomic issues are prominent in Ehlers-Danlos, rehydration drinks have long been on my radar. One of the most popular is NUUN, but I think it a bit more expensive than what you have featured, Cort.
I remember on several occasions while in Mexico, having a horrible bout of tourista, and using the Mexican Coca Cola (different formulation than in the U.S.A.) plus table salt to save the day. Works if nothing else is available…
I have heard of people who have benefited from NUUN. There are several formulations of NUUN; it appears to contain electrolytes, vitamins, nutriceuticals, etc. It does not contain salt or dextrose – and doesn’t appear to be directed to increase blood volume. I think its mainly an electrolyte enhancer and vitamin booster.
Saline is mostly water with some salt, NaCl.
If I get what Cort is saying, both IV saline and ORS help to increase blood volume while taking a saline equivalent (water with NaCl) orally is harsh on the stomach and / or gut and the fluid accumulates in the interstitial space. In more plain words: drinking something very similar to saline increases edema rather then blood volume.
A key to ORS is that it contains plenty of glucose and that activates the, as Cort writes it “intestinal Na+-glucose co-transport (GLUT2,symporter) carrier”.”
Why is that important? Absorbing salt from the gut, and with it directly related absorbing water from the gut does cost (plenty of) energy or ATP. (POTS) Patients with reduced blood volume likely have a significantly reduced blood flow to the gut and with it a likely significant decreased ability to produce ATP in the gut. Most ME patients have on top of low blood volumes an obvious difficulty in producing enough ATP to make things worse.
If so, they have a significantly reduced ability to absorb salt and water from the gut and get it into the blood stream.
The gut has many different mechanisms to absorb Na+ or sodium. Absorbing sodium is the first step to absorb water from the gut and deliver it to the blood flow.
Very likely not all mechanisms to absorb sodium do cost equal amounts of ATP. However, some can only be used when a certain combination of nutrients is widely available. This is the case for transporting sodium and glucose in a single go with a specialized “co transport”. I can imagine that this co transport does cost less ATP then separately transporting the sodium and the glucose from the gut to the blood.
If so, when being poor at producing ATP then having this combination available for uptake is a clear plus.
The important question: why would ORS mainly increase blood volume while “oral saline” would mainly increase edema?
The answer may lay in the lymphatic system. The gut has *two* distinct systems of food (and water) absorption:
A) Absorbing food and water directly into the portal vein (or blood stream).
B) Absorbing food and water (mainly a mixture of a fatty watery liquid called chyle) via the lymphatic system in the gut.
Route A) puts the absorbed food and water directly in the blood and directs it to the liver.
Route B) puts nutrients and fluid first into the lymph system and empties its contents into the “left subclavian vein”. See Wikipedia(Lymphatic_system) and the explaining figure Wikipedia(File:Nutrient_absorbtion_to_blood_and_lymph.png) (written like that to avoid WordPress’ spam filter).
Now route B “dumps” its liquid into the blood stream too, but now near the left shoulder area. So it should increase blood volume too shouldn’t it?
I think there is a snatch. The lympathic system depicted in the picture does not only “drain” the gut but also many other parts of the body. Now *IF* route A), direct uptake of nutrients and water into the bloodstream is “slow” due to too few ATP, then very likely more of it has to be processed by the lymphatic system or system B).
Still, also nutrients and fluids processed by system B) end up in the blood stream. So what’s the difference? I believe that it lays in the capacity of the lymphatic system. If quite a bit more volume of fluids has to be taken up from the gut by the lymphatic system, it’s already quite busy. Then absorbing water from the gut takes up more capacity from the lymphatic system then “what is meant to be”. So that almost naturally leaves less capacity of the lymphatic system left for draining (much of the rest of) the body from excess liquid, from preventing edema to happen.
In turn, I believe if the capacity to drain excess fluid from the body by the lymphatic system decreases then the supply of fresh blood to the cells has to be decreased. Two “good” ways to do that is to reduce blood volume and blood pressure. I’ve written about that in Cort’s previous blog on “saline-chronic-fatigue-syndrome-cardiovascular-functioning”.
I did found this interesting article titled “Salt and water absorption in the human colon: a modern appraisal” published in BMJ journals written by “G I SANDLE”; again no clear link to avoid WordPress ‘ spam filter.
It details some very difficult processes to absorb Na+ in the gut. The interesting part however for us is:
“Salt and water absorption in the diseased colon
INFLAMMATORY BOWEL DISEASE”
“Decreases in net Na+ and Cl− absorption, resulting in impaired water absorption or water secretion, are the main electrolyte transport abnormalities in ulcerative colitis and Crohn’s disease of the colon.”
“This reflects a notable (>70%) decrease in basolateral Na+,K+-ATPase activity, and possibly also a defect in amiloride sensitive apical Na+channels.”
” It is presently unclear whether inflammation impairs electroneutral NaCl absorption in the human colon, but this seems highly likely as basolateral Na+,K+-ATPase is also an essential component of this Na+ transport process.”
=> Now we don’t generally have an ulcerative colitis or Crohn’s disease diagnosis, but plenty of us have a gut in a very poor and or inflamed condition.
=> *IF* I get it correct the sodium and water absorbtion by “method A)” described in previous comment is far slower then in healthy people.
=> *IF* I get it correct, that puts a strong extra burden on the lymphatic system, increasing problems with edema (and indirectly possibly low blood volumes as too much liquid is not recycled well back into the blood stream).
Oh gosh dejurgen, I wish I had my old brain and could follow your detailed explanation, but I can’t.
Do you think that the oral solution in the research paper will work or won’t work?
Thanks for all your excellent contributions!
dejurgen, that is very interesting about (my paraphrasing) impaired water handling in the colon. I have a very dry colon despite however much electrolyte-balanced fluids enter my body orally or through IV. I’ll need to look into this further.
dejurgen What you write is extremely intresting. I’ve tried for about a half year to drink more fluid (not salty) and add more salt to my food. And I believe that it to some extent have helped. I have a suspiscion that I might have lipedema, though I haven’t sought for yet another suspiscious diagnose. But what you write about the lymph system and its roll is interesting.
Also your article Cort, is interesting. I had no idea that glucose was so important for instance.
Thank you both!
Me neither. That was eye-opening.
@Birdie: My estimation is that:
* ORS will likely increase blood volumes of ME patients with low blood volumes (not all have it!) for a short duration after intake.
* Likely part of the patients will feel better each time after taking ORS.
* Some may benefit long term.
* It likely will have clear short term downsides and / or delayed long term consequences for many patients.
As Cort said, supplying such amounts of glucose might be a tricky thing for many patients. Just think what it could do with patients with, known or unknown, problems with yeast, candida, SIBO…
I’ll add to that: It could further increase Cerebral Fluid Pressure for some patients, something that is too high for many already. That can have damagaing long term effects on the brain. Many patients might also have weakened blood vessels and increasing blood volumes and pressure might increase the chances for internal (brain) hemmoraghe.
So we don’t have a clear winner yet by simply taking ORS, especially looking at long term trade offs. Some might improve long term, others might deteriorate. It however sure deserves a lot more research!
@Birdie, Jayne, Kajsa:
If the lymphatic system in the gut is an important factor in these low blood volumes, or like that paper says Na+ and water uptake is quite difficult in an inflamed gut (in inflammatory bowel disease) then it makes sense to try and put extra effort into healing the gut.
Unfortunately that is a very difficult thing to do. For me however it has been rewarding too. I now have worked two years mainly on trying to heal my gut.
Before that I thought my gut was the only thing that still worked fine. I could change diet and it didn’t impacted me the least. Oh boy how was I wrong!!! It appeared I am intollerant to about 90% of the food I ate. Even going to a (mild) exclusion diet one has to find still a few diverse food sources one eats regularly. I tried and have a source of everything. I daily ate an apple for semi fast sugars. An apple a day keeps the doctor away they say. Boy, when I left that one out for half a year as there were small signs that might not be true for me and ate two really small apples again as breakfast one day my stool was blood blood red and the water in the toilet was deep red too. It took months to get my gut even a bit balanced again even quiting eating any fruit. Sorry for the visuals, but I am trying to make one thing clear: don’t just dismiss and underestimate the role the gut can have in (your personal case of) ME/CFS!!!
Two years later and having a far stricter diet and trying to find other ways to improve my gut and I still am nowhere near halfway in improving my gut health. Unfortunately things that commonly improve and support gut health plainly backfire, often in a big way. And what works after carefull planning and considering is often devastating for another patient.
So when it comes to the gut, try and hunt for food intollerances even if you think you don’t have any. Then try and adjust your diet but keep it balanced. That is already very challenging. Then, when making changes go low and slow! One single mistake can set you so much back.
BTW: my skin color and wound healing (and general health too) has improved quite a bit since doing that. That indicates better blood flow. But keep in mind: what works for me can backfire badly for you!
I’ll plan to resume writting on what works for me on the forum but Issie and I try and work out better and safer ideas first. That’s quite energy consuming to say the least. We have learned so much since we started working together over a year ago.
@Jayne: My gut / stool has a tendency to oscilate back and forth from diarrhea to constipation again and again. I managed to get it more stable but it remains a work in progress. I think it may be related to two distinct ways to keep toxic stuff from the gut from entering the blood flow: a) flush it as fast as possible out of the body, b) make gut contents dry and hard so few of it crosses the gut barrier.
To have a dry gut may seem to be good at absorbing water from it.
Things are more complicated however. The gut recycles water several times. For example when food from the stomach enters the gut, it is “showered” with a waterly liquid with sodium bicarbonate in order to neutralize the strong HCl acid that otherwise would burn holes through the gut. That is water that had been absorbed by the gut previously and is reused and dumped with a packet of salts into the gut later again.
Compare it a bit with a dishwasher. A dishwasher manages to use only about a bucket of water to wash plenty of dishes. It does that by recycling the same water with soap again and again. Just imagine how long you could spray the dishes with a single bucket if it didn’t recycle the water…
So having a dry gut could mean you absorb water (and sodium) very well from the gut OR it could mean your body refuses to give up and recycle much of its hard won water and chose to be very stingy on using stomach acid (another use of previously absorbed water), water with sodium bicarbonate to neutralize the stomach acid and…
Dejurgen – I’m leaning towards the role pancreas has in these gut issues.
Putrescine – ornithine decarboxylase – wonky ALP function – accumulation of free B6 in the blood (and possibly resulting in aldehyde toxicity) – 1-carbon metabolism – taurine – high amylase and pancreas issues:
All these are connected.
it may be for more people than we realize.
Protease plays a role in wound healing.
Putrescine modulates potassium. Also has a role in the intestines, immune system and inflammatory response. Repair of tissue. Apoptosis. more
https://www.frontiersin.org/articles/10.3389/fnut.2019.00108/full
Not enough space to go over the literature and findings.
Will make it to a post on the forum at some point soon…
I hope you get to share what is working in treatment too.
@Meirav:
you mentioned “high amylase and pancreas issues”
Mine and my mothers blood amylase is always very high for non-alcoholics. The first time my doctor tested my mothers blood for it he just redid the test as he said it was obviously wrong. It wasn’t and he never found a reason for it.
The best reason I found so far is amylase’ ability to break down pathogens and biofilms. See a paper titled “Enzymatic degradation of in vitro Staphylococcus aureus biofilms supplemented with human plasma” from “Chase M Watters, Tarea Burton, Dickson K Kirui, and Nancy J Millenbaugh” for more info on it.
What clear connection with amylase do you see here?
As to sharing what works with me so far: it’s not witholding but rather being very careful to release info that can backfire very strong with many patients before we get safety better.
Both Issie and I have reacted poorly to very poorly to things that work well for the other and we both have a well above average sensitivity and knowledge on how or why things could work and what to take care of.
We go low and slow too, far lower then most would even consider. Still, we get some unpleasant surprises now and then. Knowing how (understandably) desparate to try things that work for someone else many ME patients are, we are well aware of the risk of puting out info before it’s ready.
I know very little.
https://europepmc.org/article/med/19444716
https://ajp.amjpathol.org/article/S0002-9440(10)62074-3/fulltext
https://pubmed.ncbi.nlm.nih.gov/18235212/
– there are more studies if you scroll to the bottom of the last link.
My amylase is also elevated.
I do have pain in abdomen area, corresponding to pancreas.
I have realized I’ve had a few episodes of this over the years.
Does your/mother’s present with pain?
Episodes are preceded and followed by odd changes in bowel movements and digestion.
(and the increase of the foul smell)
Have you had your PLP plasma levels checked?
Repeat testing, as our condition is aleatory, our disfunction ‘dynamic’.
Have you had a look at your ad mother’s ALP levels through out your lifetime?
Per the Hypophosphatasia guidelines for what is considered low?
I posted those ranges on a forum thread.
P.S. It may or may not be HPP. It is easy to rule/check out.
Wonkiness may be related in some way.
I’ve been reading in on putrescine and spermidine. I did find some things related to edema, brain NO synthesis and destruction of the BBB. That seem quite relevant to the blog.
The paper titled ” Polyamines induce blood-brain barrier disruption and edema formation in the rat” from “L Glantz, J L Nates, V Trembovler, R Bass, E Shohami” says:
“When injected into the carotid artery, rapid increase in BBB permeability was found 1 min after putrescine and spermidine (p increase BBB permeability after !!1 minute!!
=> edema formation in the brain (increased CBF pressure)
From Wikipedia(Spermidine):
“Spermidine synchronizes an array of biological processes (such as Ca2+, Na+, K+ -ATPase) thus maintaining membrane potential and controlling intracellular pH and volume. Spermidine regulates biological processes, such as Ca2+ influx by glutamatergic N-methyl-d-aspartate receptor (NMDA receptor), which has been associated with nitric oxide synthase (NOS) and cGMP/PKG pathway activation and a decrease of Na+,K+-ATPase activity in cerebral cortex synaptosomes. ”
“Inhibits neuronal nitric oxide synthase (nNOS)”
=> messes with NA+, K+ -ATPase: impaired fluid balance
=> decreased neuronal nNOS: contraction of neuronal (= brain and nerve) blood vessels: decreased neuronal blood flow
From a paper titled “Increased Red Blood Cell Polyamines in ALS and Parkinson’s Disease” with authors “Gomes-TrolinI.NygrenS-M.AquiloniusH.Askmark”:
“Over 70% of circulating polyamines are associated with red blood cells (RBC).”
=> Putrescine and spermidine are polyamines (diamines to be correct) and associated with highly neuronal degenerative diseases. RBC seem to spread theses very well.
@Meirav:
I’ve potentially / plausibly linked many topics you mentioned here and previously this night: vit B6, putrescine, ornithine, SAMe, methionine, homcysteine, ammonia, liver and pancreas dysfunction (related to ALP and amylase), gut dysfunction…
If you’d be interested could you open a topic on the forum titled “Diving deep: excess B6 levels”? It’ll be too lengthy and way too much off topic to dump here.
I prefer to keep private health science communication limited to “fixed buddy” Issie as we are working very efficiently together, are very complementary and that connection is already more then I can handle. Other people might have an interest in your excess B6 take too and or add to the (very technical however) conversation.
Ha!
I can relate:
I can feel the wheel cogs of my mind clunk clunk clunking as they reconfigure themselves and change direction.
I have been meaning to open this up in the forum.
I think AcH Influenced would be interested as well.
Working out in output format all the steps I have taken to get to the understanding I have today, that one is real slow.
What is happening to me I think may well be happening to… many?
I think it is tied to what you and Issie are studying,
hence, bringing it to your attention.
See you in the forums.
I submitted a comment today but it went to moderation and never got posted.
I find a lot of this very confusing; however, is it possible that no one has thought to mention the kind of salt they use, or does anyone know that table salt should not be used as it is isolated….. would it not be a must to use Celtic Sea Salt, that is total real whole salt.. Also would it not be possible to use xylitol made
from beech tree bark in the US (not the corn one from China} if you are going to
make up your own potion – or even if you are using salt at all, or any form of sugar?
I could never tolerate normal table salt, it is gives high blood pressure, and xylitol is
a perfect form of sweetener for me.
So, I found a recipe, maybe for those of us in other countries: I am hoping this will help my dehydration, which is so obvious and getting worse. Hopefully that will help me with POTS, and make CFS/ME a little more bearable. Just experimenting, and with limited funds some of us have to.
1-1/2 cups spring water, juice 1/2 lemon; 1/4 test. sea salt, 2 tsp honey (I am using
xylitol)
Does the xylitol contain dextrose? That is the key to effectively carrying the salt into the bloodstream.
Im sure the glocosis IS the reason it helps perfusion to the brain! Saline did not. Why don’t they try with glocosis infusion also. I guess they will see the same. Because I feel our POTS/ME brains easily get hypo-glycemic intra cerebrally and we need sugar to not faint. At least that is so for me. Only water and salt dont help. And if I don’t get sugary things, or wait too long between meals, I colapse. But i’m still gaining weight. So it’s a very bad catch 22. Need someone to do research on these things. Please researchers!
Actually I’d like to see them use Hartmanns or 4%in1/5 or alternate bags of 1/2 litre dextrose and saline….
I was the same way for years. My doctor told me to eat a bit every 3 hours. I believe it was 15 grams of carbs and some protein or fat. I think it was 5 or 10 grams for the protein
or fat. This was preventative. If I waited until I felt the low blood sugar, I needed to eat a lot more.
This is exceedingly interesting! It will be very interesting to see if it may benefit ME patients, that do not have significant issues with POTS. It is after all well known that saline IV has a conciderable effect on many ME Patients, but it is a regime that is diffucult to administer and bear the risk of infection from the iv line.
I feel the need to point out one thing though: the ORS formula presented here is not the current ORS formula recommended from WHO, it is the old one. This may present a future problem of sourcing ready made solutions, as the manufacturers probably will adhere to the current reccomendation, going forward.
Perhaps you Cort, may be able to get some expert’s take on the efficacy of the old vs new formula, in POTS (and me/CFS)?
I might be pregnant. Is it still safe for me to use ORS?
Marianne, do you have problems with salt, potassium or sugar? These are the ingredients in an ORS, along with water.
Yes, thank you! We need to understand the difference and it would be important to know which ones were used that helped the ME patients! There are potentially negative side effects for adults with the newer version. If any adult is likely to have a side effect, it would be an ME patient. 🙁
I’ve been making my own ORS but without glucose for the past year or two. I’m not sure it helps with POTS, but it seems to improve my water retention – without it anything I drink seems to pass straight through and I am always peeing. I’ll try adding the glucose and see what difference it makes.
My recipe is based on the new ORS recipe from the WHO:
https://apps.who.int/iris/bitstream/handle/10665/69227/WHO_FCH_CAH_06.1.pdf
They say you can substitute sodium bicarbonate for the trisodium citrate. The latter improves shelf-life in tropical countries, so isn’t strictly necessary. I’ve also swapped potassium chloride for potassium citrate. So my recipe is:
Sodium chloride 2.5 g/L
Potassium chloride 1.5 g/L OR Potassium citrate 2 g/L
Bicarb soda 3 g/L
Glucose (optional) 13.5 g/L
If you can get Salt Skip (potassimj chloride), then all the ingredients can be bought from the supermarket, and the cost is negligible.
Cooking supplies sell the Trisodium citrate. Potassium citrate is more palatable than chloride. I found all the ingredients as food grade or pharmaceutical grade but then found the Trioral which is cheap and easy. We also give the Trioral to our friend who has MS and is on feeding tube only but still dehydrates and ends up in ED regularly. Her ICU nurse sister will run trioral in the feeding tube when she appears to be funking out with almost immediate response. Previous to this idea(her sister and I came up with it) she was regularly hitting ED and then being in hospital for 4-5 days on IVs and perhaps antibiotics with suspected UTIs (she has bladder issues also). I know MS is not ME but there are things we seem similar on and this low volume seems similar with this girl and I. We both pep up quickly if folks work out we are dry and need our “IV replacement”
How much a day are you drinking a day? I find I wee all night up to 9, 10 times! I also have low blood pressure, but not Potts.
How much a day are you drinking a day? I find I wee all night up to 9, 10 times! I also have low blood pressure, but not Potts
I drink about 1-1.5 L of electrolyte per day.
thanks Garth, What ard you taking. I have tried to take hydralyte which is all I can easily get in Australia but last night I was weeing every half hour. I am clearly not retaining anything. I also hate this level of suger. Being a bad insomniac I am finding it quite overwhelming. I do have low blood pressure so thought this may help.
My recipe is above.
thanks Garth, can you please post if you notice any difference with the glucose.
Nerida I was the same – until Orthostatic specialist physician made me lift head of bed by 6″ and gave me ACEI or Sartan at bedtime to drop my night time blood pressure. He says you are “dry” all day(brain and kidneys think) and they pee less than they need… then at night you lie down and they see a sudden increase in perfusion – “Ah ha – high blood pressure(compared to daytime)” so they proceed to pee it all out. The above strategies a) Let me sleep better and b) have me waking less dehydrated feeling
Janis, thank you for that share on raising your bed!!!
Does anyone know if this still works if taken with food?
Merida – try xylitol made from beech tree bark instead of any form of sugar…
available in Australia from company called Naturally Sweet. I use it for sugar.
Have started mixing my own sea salt, mineral water, xylitol and lemon juice,
and have within two days had one night where I don’t wake up to pee.
That is amazing for me. Hope this helps. Billie
Nerida …. left you a message but the PC auto correct called you Merida???
Hope you get this message, here’s what I do anyway-
Recipe :
1 1/2 cups mineral water
Juice 1/2 lemon
1/4 tsp sea salt (Celtic Sea Salt the real ting)
1tsp xylitol
or if you can’t get it 2 tsp honey, but honey is not good with me
I sometimes put more salt and and one glass water
Thanks Billie, How has it helped you? and how much a day do you have, or is it just what that amount makes?
Nerida, sorry to take so long, maybe you won’t see this. I just take
that amount per day…. sometimes, because of all that I take, I just
sip it during the day, and other times I drink the lot….. see how you
go….. there seems to be a discrepancy about xylitol and whether it
contains glucose, I can’t answer that scientifically……I use a pendulum.
I know that xylitol doesn’t effect me as badly as sugar or honey.
It has helped me not to be up so much at night wanting to wee, which
for me is a plus; I don’t see any signs in my skin improving. Good luck.
Just spent hours researching quality ORS options in Canada. They’re surprisingly difficult to find.
I’ve concluded that the two best options are the flavoured Normalyte (6x 500ml solutions for $11CAD on Amazon Canada) and MEC’s Adventure Medical Kit (3x 1litre solutions for $8.75CAD on mec.ca). The MEC option sounds expensive. But if you consider the precise ingredients, you’ll note that it contains the pure WHO formula with no additives and at a higher concentration than Normalcyte. Plus, if you don’t have a MEC store location nearby, you can have it shipped all over Canada for free if you spend over $50. A great option for those who want to try it before buying in bulk.
Thanks David – I will put MEC in the blog.
thanks. Billie
Hi David. Thanks for the Canadian content. Still wondering, though, what is the recommended dose and esp, frequency for the salts?
I had an experience recently which might be of some interest here. I lost maybe a litre of two of blood, which brought on a fairly severe POTS symptoms, for a few days, until I rehydrated. I’ve had only fairly mild symptoms of POTS over the years so it was quite interesting to experience what it can be. However, besides the classic symptoms, and putting aside feeling unwell in other ways, what I noticed, immediately, was a distinct relief of the CFS fatigue/malaise. That started before I started to rehydrate but it has persisted for about a fortnight, now. I got out, yesterday, for a few hours of walking, which is more than I have managed for a year or two. My point is that maybe it isn’t a matter of increasing the blood volume with the saline but rather a case of decreasing the concentration of the SITB (Something In The Blood), at least temporarily. Has this been looked at by these researchers? I’ve not heard it suggested. I am aware of bloodletting being good for sufferers of hemachromatosis but, so far as I’m aware, I don’t have that. Has anyone else had a similar experience?
@Colin,
Yes, I have had this experience too. This is an old thread on the POTS forum I used to participate in quite regularly.
https://www.dinet.org/forums/topic/15826-blood-letting-blood-draw/?tab=comments#comment-145409
You will see that blood viscosity may be a huge issue and thinning the blood is what helps. I have since found that I also have Collagen Binding and Factor 8 blood issues and those also cause too thick blood. Instead of using blood thinning medicines, I’m using enzymes to thin my blood. It has made a big difference for me. It seems to help break down fibrin and also helps with a type fungus they found in my blood and organs. And that has helped all around.
I DO NOT, salt load. Don’t believe it to be at all helpful. I too have HyperPOTS and EDS.
Many POTS docs no longer RX regular IV infusions any more. Way back in the early days of discovery, many of my POTS friends got ports and had them regularly. It helped the day of, but wasn’t lasting.
Soooooo, you are not alone with blood letting helping and it took many years for me to find too thick blood as an issue. I also find a need to vasodilate rather than constrict and this may be one of the causes. If you clamp down the veins on too thick, sludge blood, it will hinder the flow even more so. Thinning the blood and vasodilation has been of benefit to me.
Issie
Thanks for that, Issie. I was not aware of much of what is on that thread. But I see that you have been on the case regarding the poor, blood supply to the brain for quite some time. It is all so complicated, what with the red-cell-deformabilty thing, poor perfusion, stress-system problems and all the rest of it. It is probably too much to hope for a magic bullet that can strike at the heart of it all but who knows? Maybe with the new nanoneedle, Davis et al will come up with something.
But, meanwhile, I can report that, as expected, things have returned to normal for me, less than two weeks after the blood-loss episode (and gastric fluids, if that matters). I had remarkably-little PEM after my Big Day Out (which was a week and a bit after the episode) but today, after just a little too long at the computer last night, I was knocked flat on my back. And, having had no prior experience with rehydration salts, I did overdo it and ended up with bloated, lower legs and feet. It got me out of the emergency situation but I can now understand that it is problematic, as you say. I will still try the W.H.O. type as it is supposed to work differently, but I shall be more careful with it. (I used Hydralyte, the most commonly available brand in Australia, which is not made to the W.H.O. standard.)
I shall look into the possibility of too-viscous blood, as you suggest. But meanwhile, I’m pleased to see that ginger is supposed to thin the blood. I’ve only recently taken to ginger infusions (just ginger root, sliced thin, in hot water with a little honey; and I eat the ginger when it is sufficiently washed out) and I do like it.
You’re welcome. Will be interesting to see if your blood is too thick too. There is another thing with too thick blood called APS. I also showed positive with that one time, but not the next. You have to have 2 positives for offical DX, but I was on blood thinning herbs and enzymes then. So probably had thinned it out and got a false negative.
Ginger is nice and good as a tea. Just be aware if needing surgery that they recommend being off certain things before that.
Great article!
Does anyone have any idea of a UK source for suitable ORS? The most commonly used here is Dioralyte, which has the same ingredients but in a slightly different ratio. I wonder if they would be recommended?
Each sachet contains Sodium Chloride 0.47g, Potassium Chloride 0.30g, Glucose 3.56g, Disodium Hydrogen Citrate 0.53g
Also contains Silicon Dioxide, Saccharin Sodium
You should update the blog post to mention that you can get a sample pack (6 sticks) of the Normalyte for free (one pack per household, $4 Shipping) if you go to their website.
https://normalyte.com/collections/free-samples-program/products/free-normalyte-pure-sampler-pack
I have well-controlled diabetes and sometimes yeast infections but I do eat sugar. Is one formula for this better than others for diabetics? Thanks
As you write in this blog about to drink the salt with water to improve the blood volume is right, but if someone have the high blood pressure then it is effective to drink the salt with water or taking the oral rehydration solutions are better than this one.
I ordered Normalyte a few weeks ago. I take it for my Pots and OI. just started and I get pain in my intestines a lot and much gas:-(. just took 0,5 litre with one pack of normalyte.
what can I do with this problem?
Pedialyte a children’s formula for hydration seems to be a good copy with dextrose. At Walmart it sells for different prices depending, lowest $4 per Liter.
Hi
one question from Greece. I have found Commercially available ORS that contains sodium bicarbonate (3.4 grams), potassium chloride (1.5 grams), sodium chloride 4,5 garms and dextrose (27 grams), all of which is to be added to 200 ml of water based on the latest W.H.O. standard (as it is mentioned on the package). I am a bit confused as the relative article mentions 1 Liter of water. Which is the correct quantity of water and how often should be taken (the article mentions that it had good results even every 10 days. I am asking as i suffer from OI and i am worried about possible side effects. Thanks.
Since this study was on children, how much and how often would be effective for an adult? I got the Normalyte samples, but haven’t tried it yet since I don’t know if I should double the amount or frequency for an adult. Any help with this info would be greatly appreciated.
Hi Cort,
I came over this great article,
I am just wondering, has jianas brothers an onlineshop ?
I couldn´t find anything on the internet
Thanks
Can anyone tell me if there is an ORS that matches the WHO recipe available in Australia? I have tried searching and contacting various companies, but either the formulation didn’t match or the company couldn’t (wouldn’t?) tell me whether it did or not.
Sorry, everyone. I still don’t understand what the dosage is for cfs/me. I got the idea that one does every 10 days was all that was needed, from the article. But seems most peeps are dosing daily.
Definitely daily. The blood volume increase does not last. It needs to be done daily.
Hi Cort,
I just purchased the food grade ingredients and started making the ORS myself. It’s super easy and tastes ok.
I normally drink 3 liters water/day with salt and dextrose. This was advised by my daughter’s doctor for her CFS a few years ago, as the dextrose carries the sodium directly into the blood, bypassing the liver.
My question: If we drink one liter of water/day with the ORS, is it necessary to add salt/dextrose to our water the rest of the day? I’m wondering if the small amount I’ve been using is beneficial or if it must be in the exact proportions. Or maybe I’m over thinking this lol.
I’ve recently discontinued Florinef (after 5 years of fairly controlled OI symptoms) due to unexplained high blood pressure during the day. So I’m back to the the drawing board in trying to figure out what works.
Thank you for all you do!!
Thanks, Cort. Really enjoyed your summit interview with Lorrie Rivers. This is where I got the heads up on the salts.
Cool! I tried the salts, stopped them, and tried them again, and am really appreciating them now. I’m using Trioral.
Cool back at you, Cort, Trioral is what I’m using, too! My hubby was able to pick some up locally at MEC, a total of 10 packages. Now, the thing is : I don’t have POTS but do have cfs/fm and brutal PEM. We bought a total of 9 packs so, a supply of 9 days. Now I need to know if the benefit is supposed to work right away or take some time? I’ve looked through the comments (and re-read the article) but don’t quite understand. The reason I need to know is I would like to order it online next time to save my hubby the trip.
Reporting here that I had a very similar experience with Trioral. I started them and found it was a big boost. Then it seemed to taper and I stopped them. Then I really slumped and I’ve re-started it and really appreciate it now.
Overall, I’ve found it:
* Greatly helps with the cognitive impairment
* Significantly helps with the orthostatic intolerance
* Does NOT help with post-exertional malaise
The last two points are in tension and important. While “rehydration” makes me more able to move about and increase my activity, it doesn’t make this advisable! I have to use my (relatively unimpaired!) mind to keep limiting my activity.
D-ribose instead of glucose or xylitol and Dr Myhill’s “sunshine salt”?
I’ve just been diagnosed with Dysautomonia… breathing is the major part even though I play tennis every day but anxiety is also is a problem.
What’s the best recommendation for me regarding ORS
I’ve seen a lot of people with kids who have POTS recommend ‘Banana Bags’ oral solution. Would these be as good options as the other ORSs mentioned in this study? They have “electrolyte ratio (sodium + dextrose) formulated to WHO standards for maximum intestinal absorption of water” plus “750 mg of Vitamin C plus a high dose B-Complex with L-Methylfolate & Methylcobalamin”.
For those of us with dysautonomia who can’t take in large amounts of fluids orally, or who don’t respond to them, IV fluid therapy is vital.
If you are an Aussie, please sign this petition:
https://www.change.org/p/medical-community-make-intravenous-fluids-a-standard-treatment-for-dysautonomia
I am one of those patients now considered “medication refractory”. I may have a faulty RAAS (the system that regulates blood volume) that won’t let extra fluids in via the GI route. Salt and water loading hasn’t worked for me, yet my doctor says I show signs of hypovolemia. (And let’s not forget that dysautonomia treatment could be greatly improved if patients could get their blood volume tested. Right now doctors have to guess and surmise whether their patients might benefit from volume enhancer medications, such as fludrocortisone.)
The only way to find out whether IV fluid therapy would help me is to try it. I’ve spent two years trying everything else, and now my doctor wants me to have a short course of IV fluids. Research has shown that this improves POTS symptoms, and, in a significant proportion of patients, the improvements continue for up to six months after the therapy. (That’s where follow-up ended, so the improvements in those patients may continue to this day.)
But because I live in the country, my GP and doctor have to ask the local hospital to do it. This has opened up a nightmare of bureaucracy for my family, and, I’m sorry to say it, downright lies in a couple of instances.
If I lived in the same city as my specialist, I could have the fluids at the hospital where he works. He can order me a blood test that I can at my local pathology centre, physio at my local physio practice, and medication that I can get from the pharmacy over the road, but he can’t order the simple and possibly life-changing treatment of four weeks of IV saline.
I don’t even need a port or special access for this short-term trial. Hospitals administer IV fluids hundreds of times a day every day on the wards and in emergency. They are even administered in the infusion centre alongside other mediciations, such as IVIG.
Why can’t I trial a vital treatment that is inexpensive, and, in this short trial format, low risk? All I need is a bag of salt water, a needle in my arm, a pole and a chair.
I’m on a keto diet (extremely low carb). So how can I increase blood volume then? Can I? I though sodium worked as well.
Oh holy cow. My health has taken dramatically in the past three months. I worked out it was from switching to sorting Easter from two water. Did some research and ended up here quickly as usual. Bought some undisputed electrolyte blend (bulk nutrients Australia) and added it to my water today. Bam, horrendous fatigue improved dramatically within hours. Very similar to how I’ve felt before getting sick when getting an IV for severe dehydration and exhaustion (yeah I was an athlete once like many of you). Glucose powder on the way to add (I i baulked a well as some of you others in the comments but I’ll give it a go, it’s only a little bit and gets absorbed fast). All this info is a game changer and makes so much sense. My heart felt bad for ages. Relief on day one as well. I can’t wait to see how I feel after doing it for weeks or months. One million thanks and hugs for you Cort. You’re awesome.
Thanks and good luck!
I am in the UK, kind of new to this site, although I have popped in and read a few articles over the last few years.
I do not know if I have low blood volume, such things are not routinely measure or investigated in the UK, besides I am too ill to travel to hospital even of I could have tests, as I have severe ME and been totally homebound for 12 years.
Recently I developed tachycardia, had it for about 3 weeks, fortunately it appears to have settled last few days, whether it will start up again I dont know. I have dizzy spells especially in bed at night so i have started to take my BP and its appears low. Lowest was 83/53 and that was when I wasn’t at my worse with the dizziness and feelings of being drunk and so forth, so its likely to be lower when I am at my worse. I am waiting to get a second BP machine to compare as I have no idea if the BP monitor I am using is accurate, my friend gave it me and said the hospital told him it was reading approx 10 points to high. If that is the case then my BP would be even lower, a second machine will give me an idea how low my BP is dropping. My Bp during day appears normal, on average 110/75, can drop and can go up slightly, but that is average, but I get dizzy during day as well.
Ive got a feeling I may have low blood volume, all the research ive done indicates that. I do not take any medication for anything so that isn’t affecting my BP. I eat healthily, but of course I dont move a lot and haven’t for 12 years, i try my best but its just small amounts of moving around a small bungalow, few steps and I cannot sit upright for long, im mainly reclined. So obviously years of lack of exercise isn’t great but what can you do when your severely affected.
I started to have a reading of low blood oxygen, at times going down to 87 once or twice 85, but I am not sure that is correct because medically it doesn’t make sense as I dont have breathing issues. When I get that reading I dont feel great, weird sensations of feeling like I am going to black out and dizzy and some other strange feelings, usually I attribute it to ANS, but no breathing issues. This is why I started to take my BP, seeing if that was the culprit to these sensations and thinking the low blood oxygen levels is a red erring, faulty finger monitor! Unless anyone else knows why I would get low blood oxygen when there are no breathing issues, the thing is with ME as everyone will know, strange things happen.
So came across this article on low blood volume and want to try and make a solution but I dont understand exactly what is needed. I am not sure just drinking salt water is right way because will it increase my apparent normal BP during the day to the extent that it then goes too high! Although until I test my BP on a second monitor I cannot be sure my BP is normal during day, but from my understanding anything between 90/60 to 120/80 is normal.
So has anyone in UK managed to source ingredients for a solution for increasing blood volume? If so where form and do you have a recipe please?
I am thinking from what I have read in comments that it may be worth a try of mixing salt and dextrose, making sure the dextrose is food grade. I just saw some on Amazon that says food grade derived from grape. Is this ok? What type of salt does it matter? Can pink salt be used or does it need to be sea salt, or another salt? Do you need to add potassium or anything else?
Sorry for all the questions but its all a bit confusing for my mushy brain at the moment and a lot of comments appear to come from people in US i think, is anyone on here from Uk and have they tried a solution and found any benefits please.
I am a bit late to this – thank you to Cort. I found the article when googling, as I had an appointment with a private Dr in the UK about 3 years back when I was having a bad patch, and during it he, believing I have POTS, recommended Oral Rehydration Solution in a letter to me and my GP.
He also suggested a DIY/cheaper alternative of this known as St Mark’s Solution – recipe given here….. https://www.royalfree.nhs.uk/patients-and-visitors/patient-information-leaflets/st-marks-solution#:~:text=The%20St%20Mark's%20solution%20helps,and%20lost%20from%20your%20body.
I plan to try this out – just waiting for the glucose to arrive! I don’t actually believe I do have POTS, but have low BP, especially my Diastolic which is at present below 60, and often in the low 50s. I also suspect that I have Orthostatic Hypotension.