


Geoff’s Narrations
The GIST
The Blog
The GIST is at the bottom of the blog.
The authors took the opportunity to address non-drug means to improve oxygen delivery, blood flows, and oxygen uptake by the tissues.
Studies often have a treatment section at the end of the paper, but I’ve never seen anything like the one that showed up at the end of a study Health Rising recently covered. The “Cardiopulmonary and metabolic responses during a 2-day CPET in myalgic encephalomyelitis/chronic fatigue syndrome: translating reduced oxygen consumption to impairment status to treatment considerations” was a landmark study that validated the results of the 2-day exercise tests in chronic fatigue syndrome (ME/CFS).

The study featured some familiar names: Betsy Keller, Staci Stevens (exercise physiologist) and Jared Stevens, Susan Levine and John Chia (ME/CFS experts), Dikomo Shungu and Maureen Hanson (researchers) and had a long treatment section (called “Treatment Considerations”) at the end of the paper.
That was intriguing given the rather stark news out of the study: short but intense periods of exercise one day dramatically affect the ability of people with ME/CFS to generate energy the next day. What to do about that unexpected reduction in energy production? The authors didn’t provide any magic bullets, but they outlined a series of possible non-drug interventions they believe can “positively influence… many, if not all symptoms” found in ME/CFS.
They all centered around the “Fick Principle”.
The Fick Principle formed the basis of the authors treatment suggestions.
The Fick Principle and ME/CFS
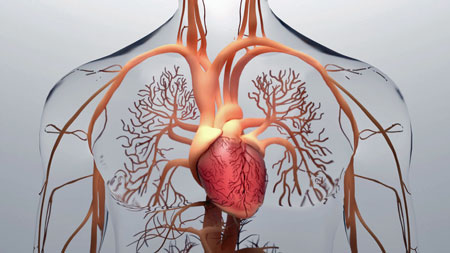
They grounded the interventions physiologically by referring to the “Fick Principle”, developed by a German mathematician/physicist named Adolph Eugene Fick, in 1870. The Fick Principle states, given that oxygen is our main source of energy, energy production is wholly dependent on three things: getting oxygen into the blood (via breathing), speeding the oxygen-rich blood to the tissues that need them, and then having those tissues extract oxygen from the blood.
Almost everything in the treatment review section flows from the Fick Principle in one way or another. Since both blood flows and oxygen extraction appear to be problematic in ME/CFS and long COVID, the question the authors grappled with was: what can be done – without drugs – to improve them?
Finding ways to improve autonomic nervous system functioning plays a major role in this process. During exercise, depleted tissues send signals to the brainstem, telling it they need more oxygen (blood). When that happens, the brainstem and autonomic nervous system usually work together seamlessly to increase breathing (oxygen uptake) and blood flows.
Not so much in diseases like ME/CFS and long COVID, though, where problems with both breathing (the ventilatory response) and blood flows (hemodynamics) impair the delivery and uptake of that mighty molecule – oxygen – into the tissues.
The authors presented a variety of non-drug ways to improve oxygen intake via breathing and improved blood flows
No Drugs Required: Increasing Blood Flows, Oxygen Delivery, and Tissue Oxygenation in ME/CFS and Long COVID
Most of the interventions proposed are not new, but they’ve never been proposed in quite the context that they were here; i.e. exercise physiologists, ME/CFS doctors and researchers prescribing ways to improve oxygen uptake in the lungs and tissues, and blood flows.
Battling “Insufficient Venous Return”, or Preload Failure
Studies indicate that many people with ME/CFS exhibit “preload failure”; that is, they are unable to fully fill the veins that enter the heart with blood. That results in less blood being pumped out of the heart (reduced stroke volume, possibly small hearts) and reduced blood deliveries to the tissues.
Treatment Approach – the authors recommend the use of compression garments (shorts, tights, stockings, shirt, sleeve), which athletes use to aid recovery by increasing blood flows. Massage is another technique that enhances relaxation and, therefore, blood flows, as well as improves mood.
Core Stability Exercises
Core stability exercises can support correct spinal alignment, improve core muscle coordination, and increase intra-abdominal pressure to improve circulation and oxygen delivery.
Both Dr. Rowe and physical therapists working with Dr. Lapp have noticed a tendency for pinched-in chests and rounded shoulders which can impair healthy breathing.
The authors recommended working with a physical therapist, athletic trainer, or strength/conditioning coach first to provide guidance and feedback. Note that local muscle sensitivity when exercising new muscle groups can be expected. Core stability exercises should be performed within the limitations of exertion tolerance, as well.
Vagus Nerve Stimulation (VNS)
While noting that studies suggest some efficacy of VNS in these diseases, the authors also reported that substantial evidence indicates that VNS can help to rebalance the cardiac nervous system to reduce heart rate.
The largest nerve in the body, the vagus nerve, transmits immune, sensory, and autonomic signals to the brain, regulates autonomic nervous system functioning, and impacts pain.
(We are hopefully on the verge of a breakthrough in this area. The NIH’s SPARC Effort is mapping out the vagus nerve in excruciating detail in order to understand how it works, and how to use it to improve health. Dysautonomia International has funded several successful VNS studies and a European manufacturer will reportedly soon apply to have its product sold in the U.S.)

Short, intense exposure to the cold can rebalance the autonomic nervous system. Fibromyalgia studies are underway.
Cryotherapy or Cold Therapy
Cold therapy is another approach athletes use to recover more quickly. The autonomic nervous system is again the main focus as cold exposure stimulates the autonomic nervous system to increase core temperatures.
The authors noted that a very brief, intensely cold whole-body exposure can re-regulate the ANS toward homeostasis – thus theoretically improving ME/CFS. Indeed, studies suggest that adding stretching to brief whole-body cryotherapy sessions reduces fatigue, and increases sleep and cognitive function. Several fibromyalgia studies are underway and the authors called cryotherapy a “promising approach”. A blog on cryotherapy is coming up.
Manual Lymphatic Drainage
The accumulation of toxins in the brain due to poor glymphatic drainage could, of course, be causing numerous symptoms. Interestingly, a dysregulated ANS could be playing a role here too as alterations in sympathetic nervous system activity could impair the lymphatic system from properly draining toxins from the brain. The authors referred to a study that found that the Perrin technique can be helpful in ME/CFS.
Red Light Therapy (photobiomodulation/low-level laser therapy)
Returning to sports medicine, the authors noted that athletes often use red light therapy to enhance their recovery. Red light therapy has been shown to relieve soreness, reduce inflammation, lactic acid, and oxidative stress, and support aerobic metabolism. This is a big topic and a blog is coming up on red light therapy.
Myofascial release therapy
Restrictions in the fascia – the thin connective tissue that supports our organs, muscles, bones, nerves, blood vessels – you name it and the fascia are likely there – could surely impact blood flows.
Peter Rowe has shown that restrictions in the fascia are often present in ME/CFS. Even simply putting a mild strain on the nerves and soft tissue can result in pain, problems concentrating, and other symptoms of PEM. Besides being painful, restricted fascia can reduce the ability of our muscles to produce force, increase inflammation, and interrupt blood flows.
It’s not clear why the fascia have become impacted in ME/CFS, but infections, prolonged sitting, or bed rest can cause the muscle/nerve system to become locked down or ‘frozen’. (The authors suggested that people who have experienced long periods of low mobility or immobility check out this option.) Once that happens, the nerves cannot elongate properly when we move, causing tension and pain.
Peter Rowe reported that in ME/CFS:
“The rib cage is often very tight, and rotational range of motion is markedly limited. Pressure on the rib cage can give rise to diverse symptoms including vision changes, lightheadedness (to the point of near-fainting), and other autonomic nervous system sensations.”
What to do about it? Rowe states that myofascial release ‘in the direction of ease’, functional technique, and strain and counter-strain and craniosacral techniques, as well as practices like Tai Chi, yoga, and massage can help the body relax, allowing more movement, a reduction in problems standing, and increased functionality.
While these techniques – like those Ray Perrin uses to get the lymphatic system of the brain going again – can be subtle, Rowe noted that this kind of work is one treatment his patients always want to return to.
The authors of this paper reported that “appropriate physical therapy, bodywork, breathing exercises, gentle stretches, stress reduction, acupuncture, foam rolling, FasciaBlaster®, a heating pad or hot water bottle, and/or nutritional support for fascia” may all help relieve pain and tension.
- Check out a series of myofascial release videos from the husband of fibromyalgia doctor Ginerva Liptan. See one of them below:
Blood Flow Restriction Training (BFR)
THE GIST
- A recent landmark study that validated the results of the 2-day exercise tests in chronic fatigue syndrome (ME/CFS) – also, surprise, surprise included an extensive treatment consideration section at the end of the paper. The treatment considerations were mostly focused on improving oxygen intake, blood flows, and oxygen uptake in the tissues via improving autonomic nervous system functioning.
- The authors didn’t provide any magic bullets, but they outlined a series of non-drug interventions they believe can “positively influence… many, if not all symptoms” found in ME/CFS.
- Studies indicate that many people with ME/CFS exhibit “preload failure”; that is, they are unable to fully fill the veins that enter the heart with blood. That results in less blood being pumped out of the heart (reduced stroke volume, possibly small hearts) and reduced blood deliveries to the tissues. The authors recommended using compression garments (shorts, tights, stockings, shirt, sleeve), and massage to improve blood flows.
- Core stability exercises can support correct spinal alignment, improve core muscle coordination, and increase intra-abdominal pressure to improve circulation and oxygen delivery. Doctors have noticed a tendency for pinched-in chests and rounded shoulders which can impair healthy breathing in ME/CFS/FM. Note that local muscle sensitivity when exercising new muscle groups can be expected.
- The authors reported that substantial evidence indicates that vagus nerve stimulation can help to rebalance the cardiac nervous system. The largest nerve in the body, the vagus nerve, transmits immune, sensory, and autonomic signals to the brain, regulates autonomic nervous system functioning, and impacts pain. With a great deal of study underway and a European company (hopefully) bringing a new vagus nerve stimulator to the market we should see progress in this intriguing area.
- Cryotherapy / cold therapy – the authors noted that a very brief, intensely cold whole-body exposure can re-regulate the ANS toward homeostasis – thus theoretically improving ME/CFS. Fibromyalgia cryotherapy studies are underway.
- Myofascial release therapy can release restrictions in the fascia – the thin connective tissue that supports our organs, muscles, bones, nerves, blood vessels, etc. Peter Rowe has shown that restrictions in the fascia are often present in ME/CFS. Besides being painful, restricted fascia can reduce the ability of our muscles to produce force, increase inflammation, and interrupt blood flows. Appropriate physical therapy, bodywork, breathing exercises, gentle stretches, stress reduction, acupuncture, foam rolling, FasciaBlaster®, a heating pad or hot water bottle, and/or nutritional support for fascia” may all help relieve pain and tension. See the blog for some videos on myofascial stretching.
- Manual lymphatic drainage (aka the Perrin technique) can help to relieve toxin buildup in the brain.
- The authors stated, “Given the broad-reaching impact of improved breathing mechanics, this low-risk, low-cost, non-pharmacological approach to symptom mitigation should be a first-line approach.” Health Rising will cover breathing techniques in an upcoming blog.
- Blood flow restriction training involves restricting the blood flow to trap the blood in specific muscles. BFR can increase strength and muscle size and improve blood vessel functioning. While work on BFR needs to be done in ME/CFS, the authors called BFR “a promising approach to reduce fatigue and improve muscle function”.
- Noting that “effective pacing can reduce fatigue, psychological distress, depression, and improve overall physical function”, the authors supported using basic journaling of symptoms to understand when the symptoms of post-exertional malaise emerge. Various ways to determine an appropriate heart rate are discussed in the blog.
- Mindfulness training can help rebalance the autonomic nervous system and help to move patients away from ‘sickness’ and towards ‘health’.
- Noting that multi-symptom diseases like ME/CFS are often treated using multiple drugs, the authors asserted that many, if not all, symptoms can be “positively influenced” using these non-pharmacological approaches.
Activity Pacing
Noting that “effective pacing can reduce fatigue, psychological distress, depression, and improve overall physical function”, the authors supported using basic journaling of symptoms to understand when the symptoms of post-exertional malaise emerge.
An exercise study can help determine at what heart rate things start to go south physiologically for people with these diseases. A heart rate monitor with an alarm set to 10 beats per minute below the indicated heart rate can then be used to avoid PEM. (Check out the Workwell Foundation if you would like to have these exercise tests done.)
For people who have not had an exercise test done, a Rating of Perceived Exertion (RPE) scale can help. An upper exertion limit RPE of 10–12 (for the Borg scale) or an RPE of 2–3 (for the modified Borg Scale) is recommended to start with.
This kind of exertion runs from non-taxing and very gentle in which you can easily maintain a conversation to “comfortable” in which you can maintain a conversation without getting out of breath.
Using journal entries, you can assess if the activity is causing increased symptoms or is helping to reduce them.
Another way to pace is to add 15 bpm to your resting heart rate (RHR + 15), and stay below that. Resting heart rate should be measured after 5 min of seated or supine rest in a quiet environment.
Another metric to look at is heart rate variability. (I use the Oura ring to determine resting heart rate, activity levels, sleep, HRV, and others). A decrease in HRV indicates the sympathetic nervous system has been activated (fight/flight) and more pacing is needed.
- Check out “Your Crash in a Graph? How Heart Rate Variability Testing Could Help You Improve Your Health“
Pacing is not a panacea – it will not cure these diseases – but the authors reported that “Effectively pacing over time may allow for a very gradual escalation of physical and cognitive activities“.
- Learn more about how to pace effectively at the Workwell Foundation.
The authors asserted that focusing on breathing should be a “first-line” approach to mitigating symptoms. Many different breathing techniques are available and Health Rising will cover some in a future blog.
Breathing
“Given the broad reaching impact of improved breathing mechanics, this low-risk, low-cost, non-pharmacological approach to symptom mitigation should be a first-line approach.”
Breathing was the next to last non-pharmacological approach addressed, but it was not the least. In fact, the authors believe that everyone with these diseases should give breathing techniques a try. Why? Because “impaired respiratory function is universal in ME/CFS”. In order to get oxygen to the brain and tissues, breathing must be addressed – but increasing oxygen levels aren”t the only reason to address breathing.
Voluntary slow or diaphragmatic breathing can quickly improve heart rate variability (which is low in ME/CFS), improve respiratory function, reduce stress, anxiety, constipation, migraine, and other autonomic nervous system maladies, help with postural stability, elimination and metabolic balance (!).
Many different breathing techniques are available and Health Rising will cover some in a future blog.
Mindfulness Training
The authors even brought in a little mindfulness training at the end – not a lot, but some. They asserted that understanding the role the autonomic nervous system (ANS) plays in the “fight or flight” response, pain, infection, and stress is at the core of integrative approaches that seek to move patients away from ‘sickness’ and toward ‘health’. (The focus on the ANS is reminiscent of Dan Neuffer’s approach in “CFS Unraveled“.)
Noting that increasing evidence indicates these approaches can be helpful in “many diseases”, they cited a study showing that meditation can increase resilience to the coronavirus.
Conclusion
Noting that multi-symptom diseases like ME/CFS are often treated using multiple drugs, the authors asserted that many, if not all, symptoms can be “positively influenced” using these non-pharmacological approaches.



Thanks for this. Its interesting to have all these treatment approaches brought together.
Re VNS: “a European manufacturer will reportedly soon apply to have its product sold in the U.S.”
Can you say who this is please?
Parasym – here’s from the blog:
A presentation at the upcoming Dysautonomia Conference will show that vagus nerve stimulation helped pediatric POTS patients with Ehlers-Danlos Syndrome (EDS). Another study found that NEMOS – a European vagus nerve stimulator – reduced symptom severity and functionality. In all, three different Dysautonomia International-funded trials have shown efficacy in 3 different groups with POTS – a nice track record. If Parasym, a European VNS company, gets approval for its device in the US, people in the US will have more options. Parasym will be presenting at the DI’s international Conference this year (June 28-30, 2024).
https://www.healthrising.org/blog/2024/06/30/lauren-stiles-dysautonomia_international_whats_up_doc_/
Thank you. I tried Parasym ear clips with a Tens machine (no longer an option as you need proof of purchase of the whole kit to purchase the clip) but I couldn’t get it to stay on my tragus. The conductive gel is really slippery and the clip just slipped off. Without the gel no connection. Water worked very briefly until it dried. I gave up with tVNS as the hassle of trying to set it up each time vastly outweighed any benefits of use. I may have a smaller tragus than most, but it’s something to bear in mind for anyone thinking of splashing out on a device.
The Nemos electrode looks very different and I’d be interested in trying it if it was available at a reasonable price.
suspect that would be nurosym, it’s the only one I am aware of specifically targetting LC/ME. See https://nurosym.com/
These don’t sound like very serious treatments for such a severe disease.
I know what you mean but they did not say they could cure ME/CFS they asserted these different options can “positively influence” virtually all the symptoms in it.
It might help that the authors are not new to this field: Staci Stevens is an exercise physiologist who has ME/CFS, who created the Workwell Foundation to support people with ME/CFS and who has been doing ME/CFS disability tests for decades, Susan Levine and John Chia are long-time ME/CFS experts and Dikomo Shungu and Maureen Hanson are long-time ME/CFS researchers – so, while no one is in any way suggesting these approaches are curative, I think they’re very serious when they state they can “positively influence” most if not all symptoms.
Why would we respond in a positive way to such methods, used by healthy athletes, when our bodies respond abnormally to CPET, especially when we don’t know the physiological mechanism of the disease? From experience, all the proposed “treatments” sound like a great way to shoot ourselves on the foot.
Because they are things that inherently strengthen the ability to exercise or recover from exercise…A lot of treatments for diseases that work, work despite the fact that we don’t know exactly why they are working or what exactly causes the disease and that makes sense that treatments. We don’t wait until we’ve figured out a disease to start trying things.
Perhaps your experience Ruben – but please note that ME/CFS experts who either are or have treated 1000’s of people with ME/CFS wrote this paper. They apparently have had different experiences.
>Because they are things that inherently strengthen the ability to exercise or recover from exercise…
For healthy people. What is the evidence regarding ME patients?
>please note that ME/CFS experts who either are or have treated 1000’s of people with ME/CFS wrote this paper
Until they provide reproducible experimental data with a measure of effectiveness stratified by severity, their experience remains anecdotal.
Here’s an anecdotal experience! I have used multiple modes of improving autonomic nervous system function, such as diaphragmatic breathing and tVNS that has caused my fibromyalgia to completely resolve and ME/CFS to improve (from bed and house bound to able to mow the lawn weekly). So I’m a believer!
When I read your comment I actually misunderstood and thought you were referring to the study itself being anecdotal (I understand now that you’re referring to recommendations people might make about treatment). So I wanted to just note the following, in case there was anyone else like me who was confused.
The study itself is very robust and wholly reproducible, and the data are available. The authors draw attention to the point Rubem is making in the treatment considerations and conclusion sections. They are also clear that the treatments have been “proffered variously by many with ME/CFS, trial and error, practice, and some clinical evidence that center on non-pharmacological opportunities to possibly mitigate pain and inflammation, and enhance blood flow, oxygen delivery, and/or tissue oxygenation.”
As I say, not disagreeing with Rubem’s concerns, I’m just trying to clarify for anyone else who misread/misunderstood/was confused by the comment 👍
And to say that even though the evidence behind the recommendations isn’t wholly robust, I’m still in a fortunate enough position to try them – while many will be put off by the non-clinically-validated recommendations, I think they are still of value to many others who want to or can give them a try.
Wow, this is amazing! I have a “mild” case of long covid, in that my crashes (varying degrees of heaviness/draggy feeling, reduced energy levels, difficulty getting up in the morning, cognitive fatigue) seem to be brought on less by physical exertion and more by excessive social stress.
One additional pattern the I’ve noticed is that on days when I feel heavy and low energy, I usually feel better – and often dramatically more energetic – within a very few minutes of leaving the house to walk somewhere, often briskly. So reading about the importance of improving oxygen delivery to the muscles through breathing exercises and other methods makes a lot sense to me. It also may explain why I often feel
the most heaviness/draggyness after lying or sitting down for a long time (I don’t have POTS). Thanks for the helpful information.
It may be of interest that my daughter, who has recently been diagnosed with ME/CFS, has a similar pattern. She has no problem with long hikes, but has had to take early retirement from her part-time work as a veterinarian, because the stress of focusing on her work with the animal patients while having to interact with the owners leads to 2 or more days of PEM.
Well said. Thank you.
I don’t think they’re trying to down play the severity. Non-invasive options to support improvement are always welcome, because they can provide relief to multiple body systems simultaneously, with little drawback (when practices with discernment and guidance for your particular situation).
Often times lifestyle shifts, such as these, can be underestimated, because their benefits only come with dedication and time. Trying it once or anything less than two weeks won’t do much. The change can be significant improvement for some people, that takes place gradually over time.
They help with pain. I use all of them and they work but do on address the underlying illness. I still have a lot of fatigue. The lymphatic drainage is helping with my bloating. I was so bloated in the face. I was holding a lot of fluid. The vibration plate and MFR really helped with my fascia restriction, especially in my hips which assisted in my mobility. I can stretch now. I just wish I could help my mitochondria.
Are there currently any decent vagus nerve stimulators on the market?
What is the name of the new one that is coming out?
Dawn Wiley runs a Facebook group that has information on different types of vagus nerve devices.
https://www.facebook.com/share/g/CVo8kYDgZzovv1U8/?mibextid=K35XfP
I only skimmed the Gist so maybe I’m missing sometimes but seems like most of these ideas, simple as most are, are still too much for the severely debilitated. I can’t imagine the shock to my system of splashing cold water on my face—much less stepping g into a whole body cold showe4, I haven’t been able to stand in a shower for ten years—or letting yet another person come into my space for massage (I already struggle with scheduling hydration IVs, occasional family, someone to cut my toenails). There have been many long periods in this illness when breath work is too strenuous, even simple deep breaths or counting out longer exhales than inhales. And the HR pacing—lol! Getting up to pee spikes me well over 15bpm above my resting rate!
These are all great ideas, many of them I’ve tried or strongly considered multiple times over the years, but I think they are beyond many of us. Sadly.
Yes, seems mostly based on what less severe could do. I also have employed several of these techniques over 30 years when less severe, but since deterioration post jab, even diaphragm slow breathing can be overexertion if I do it as much as when less severe. Am not as severe as you, can do cold water face ,but attempting full immersion years ago brought on hypothermia symptoms and bad subsequent prolonged PEM. This doesn’t seem to recognise the extremely poor thermoregulation in ME. I was doing yoga and tai chi before ME and had trained in dance so when more moderate used core stability exercises learned before. But nothing stopped me having severe ongoing deterioration from jab. I haven’t tried compression clothing, that could be possible for severe but many would need help taking on and off , and may cause overheating? I yoyo from cold to blazing sweats all the time, the idea being trapped in tight tights ! tried one device but reacted strongly with delayed PEM after using less than a minute, on two separate trials, it’s so experimental for severe ME and everyone reacts differently, I felt not safe to keep experimenting. I do bit manual vagus techniques when able. Perrin definitely helped many years ago, but plateaued and now moved, . Good practitioners who would home visit rare. Overall though good to read things some can do that should help.
Thank you ..I totally agree.
Yes, agree. My first thought was maybe they could sort these out by severity level, but I guess there’s lots of sub-variation in limitations and abilities of individuals. Hope some of these help someone, but mostly beyond my capabilities, sigh.
Cort, thanks for this. Do you happen to know of the researchers ruled out looking at pharmaceuticals from the get go? And if they did, why?
Sarah
Good question. I don’t know why they ruled them out or supplements. I was surprised they didn’t mention blood volume enhancers which are pretty noncontroversial and easy to get which should help with blood flows.
Perhaps the science required to test supplements and/or drugs was way too laborious. Probably would have taken a decade or so to come out with definitive results. Still, 🤞🤞
Too many cooks in too many different kitchens. I’ll just watch Klimas videos and now you won’t post my other comments because I may have said them before. No wonder I want to jump off of a bridge.
I promise your comments will go through Shea. In a way I fully agree with your statement about too many cooks. ME/CFS is a mess – a very rich mess full of all sorts of findings and hypotheses. In a way that’s good – but what we really want of course is clarity – and we certainly don’t have that yet.
Dear Cort,
I think you’re mischaracterizing the results of the Keller paper. The peak oxygen uptake and anaerobic threshold were reduced by 6% and 6.7%, respectively, on the second CPET day. This is hardly “a sudden collapse in energy production”. It contrasts with the common report of profound fatigue and inability to participate in activities of daily living on the day following substantial exertion…the “crash” that ME/CFS folks commonly report. I think the Keller paper studied mainly mild ME/CFS…and missed the chance to see the true magnitude of the physiologic derangements.
I don’t know who was in the studies but Staci Stevens and Workwell commonly do either the two-day or one-day exercise tests for people who are quite ill and seeking disability and often find that they are unable to safely participate in activities of daily living – that’s why they do the disability testing and why they win them.
Some of the people in the Nath exercise study were profoundly ill as well. Given ME/CFS patients’ motivation to move the science forward I wonder who was in the study.
Maybe “sudden collapse” was too much, though 🙂
Richard,
I participated in the study and was quite severely ill then, but just about well enough to drive to the venue. I think anyone more ill than I was would have had a lot of trouble participating. Your point about the small change in VO2 max is well taken. During the 2nd day CPET I was NOT in a state of PEM induced by the first day. My legs felt slightly more achy, but it was subtle. There seems to be the assumption that a 15 min CPET test will push one into PEM, but my experience (including other single-day CPET tests) was that it didn’t. Having said that, the day AFTER the second CPET (when no tests were performed) put me into the worst crash I have ever experienced, crippling me for years. So IMHO the double CPET tests do not necessarily produce data from PWME with and without PEM.
Pem can be instant or delayed, of course it would have crippled you, sorry you had to do that.
Sounds very much like:
You were normal.
Something happened.
Now ALL these parts of you suddenly don’t work.
BUT
If you spend ALL your time journaling and going to PT
You can get a little bit better.
But don’t expect to get well.
Why am I not encouraged?
I already spend ALL my time ‘monitoring my condition’ and trying to get a few clear hours daily without brain fog to write.
Not the answer I’m looking for.
I already use: Meditation. ldn. Vagal nerve stimulation. A very low-carb diet. B1. B12. Rest. Pacing. Avoiding PEM. Pain meds. Stretching. Because if I don’t, I don’t even get that little bit of functional time.
None of this is enough to get even remotely close to well.
No Nobel prize for you.
Just because you already know something doesn’t take away from the fact that people new to the disease don’t know about these ideas. You didn’t know about them until the first time you read about them either.
So the new ME/CFS and Long Covid sufferers will appreciate it because they’ve probably read about all sorts of treatments in which many don’t help.
So to hear researchers recommend these therapies means patients now know they aren’t wasting their time on these ones.
Yes we know they aren’t game changers. But a small improvement is better than none.
I’m grateful the researchers are at least making sure the ideas in the article help us
Yes!! Alicia gets it!!!!
I am NOT grateful – I’ve been sick almost 35 years, and would never get anything done with all these mini-expensive-interventions.
Alicia is right!! Thank you!
I agree with Alicia, especially for mentioning TIME. Usually people talk about doing this or that to secure what is essentially a very transient and modest gain that will just allow you to do another session but nothing more.
Essentially you become obsessed with “the programme” because you know that if you deviate by a micro detail, you’ll relapse, and if you skip the whole thing, well… you’ll be told “you really don’t want to get better, do you?”
Landmark? No. It’s the same rebranded recipe ME/CFS patients have been served for decades…
Bringing newbies up to date should be standard treatment for GPs. It is not.
But the only thing that will REALLY help is finding cause, treatment, and CURE, not bringing the distraught newbies up to minimum standards because their OWN doctors are not doing it.
We need a CONCLUSIVE cure/treatment – to benefit the newbies AND the rest of us who have been battling – for newbies and for ourselves – for decades.
Anything less is a waste of very precious effort, time, and money.
WE know the full story – so WE have to keep NOT accepting this kind of mealy-mouthed results and ‘help.’
This is all so confusing. I can’t diagnose changes. These lists are so long and the things to do are endless. As I age, I get worse. I had a good ME doctor who retired. Now I’m alone to figure it out. I can’t. Ron Davis ( whom I respect) can’t figure it out. How am I supposed to figure out what to do. I’m just going to be another blue rose. I can’t afford food. This is just too hard. I can’t do charts and cross reference this and that. I take LDN and I try but this illness has stolen everything from me after 35 years. I’m not being negative, just ready to give up. I can’t even read all of this. My anaerobic threshold is 102 and that is proven to be a limit. I stretch, meditate, fall, can’t clean or fix meals. Why isn’t there a social services aspect to this. I can’t afford the meds I’m supposed to take. How about a good pain med instead of a drawer full that don’t work.
I agree, Stephanie. This stuff isn’t ready for patients, and certainly not for our non-ME/CFS doctors.
As for what to do, there have to be some social services in your county, and Medicaid, and I don’t know how to tell you to navigate any of it. I’m so sorry. Your local hospital might have a person you could talk to, or your local government.
At least you HAD an ME doctor at one point.
Since we have the same length of illness, I’ll mention I got sick in Anaheim the week of Nov. 5, 1989, at a physics meeting – and the only extra thing I remember from then was that they were spraying for the medfly.
Having lived with CFIDS/ME for over 30 years, I would say to not do anything that you can’t afford; or that immediately seems over your capacity; or that involves convincing some kind of therapist (PT, OT, etc) that you can only do 5 minutes then must lie down. I’d say to you: when you wake up, evaluate what you have, do a bit of what you must do, rest, do a bit of what you wish to do if possible, and don’t waste energy or money on anything that sounds over your limits. If you evaluate on an ongoing basis, that’s much better than buying products or lessons. And learn which people around you are supportive in healthy ways and who is toxic.
Good Advice, thirtyyearsplus.
Great advice thirtyyears plus and also Karen below! I am also 30 year plus with this illness. The techniques listed in the article are mostly familiar to me, and I have found them to be supportive without reversing the course of the illness. However….
Two years ago, I found a practice that has seemed to turn the tide….. scientifically based breathwork. I have been a meditator for almost as long as a CFS sufferer and this particular approach to breathwork has led to a greater capacity to work with the chronic pain and fatigue and allow for greater involvement in the world around me – less brain fog. After I began incorporating this style of breathwork, I felt more able to access other supportive methodologies.
Here is a link to an explanatory video of the breathwork:
https://bytcourses.thinkific.com/courses/your-breath-your-truth
As one of the other commenters below mentioned, I do feel like I have to be incredibly disciplined in its implementation – “an Olympic athlete” of breathwork. It is not a silver bullet. With that said, I was able recently to take an enjoyable vacation that seemed wholly out of the realm of possibility 2.5 years ago.
One other element that has seemed to promote recovery is a very healing self compassion meditation by Tara Brach. At just 11 minutes long, it reminds me (in the face of overwhelming negative self talk) that this illness isn’t my fault and that no matter how much I am able to “Do” in the world, I still belong.
https://www.youtube.com/watch?v=wm1t5FyK5Ek
Many thank to all the commenters and also to you Cort for your dedication to this blog. I know that reading this material, though sometimes difficult, has inspired me to keep going.
Thankyou for sharing these links ❤️
I’m 26yrs in, and this is my strategy exactly.
Also, corsets are amazing for me, when I need to go out and about. Compression, support, and posture aid all in one. Plus: it’s nice to feel pretty.
💯! Thank you! I couldn’t agree more
Cort, Yes, yes, yes, thank you so much for writing about these non-pharmacological approaches! For so long I have wished all this information was available in one spot so others might benefit. No, unfortunately, they won’t cure us, but they can still improve quality of life for many. As a former occupational therapist and rehab director with additional training in myofascial release (MFR), craniosacral therapy (CST), red light and low level laser therapy, and who now is disabled due to ME/CFS, Sjogren’s, Lyme disease, dysautonomia and other conditions, I have personally experienced the beneficial effects of many of these suggestions (and have witnessed in many of my prior patients).
Fascia is such an important topic that is not discussed enough! It runs throughout our entire body down to the cellular level (and into our brains!) and has so many important functions. However, we often develop restrictions that interfere with these functions and those can be caused by disease, inflammation, dehydration, scarring, toxins, and physical and emotional trauma. These restrictions can interfere with blood and lymph flow, joint and muscle movement, organ function, cognition, breathing, etc. The above treatments can be helpful with these problems and I use many of them myself on a daily basis. Without them or the supplements I take, I would be mostly bed bound. In fact, I think someday we will find a lot more answers from studying fascia
For those who are bedbound or very limited in activity (check with your doctor first though!) – some alternatives methods or tips that have been helpful to me include the following –
Cold therapy – Even putting a soft icepack on the back of my head and neck or lower spine has a beneficial effect (I realize that ice sounds uncomfortable, especially when you are in pain, but after a moment or two, it actually starts to feel good!)
Compression – I’ve found abdominal compression to be the most effective (even wearing shapewear tank tops and, for some reason, they do not make me feel hotter!).
Hydration – Fascia gets more restricted and “sticky” the more dehydrated you are. While many people drink water, I find the electrolyte drinks and mixes are much more helpful in maintaining hydration
Vagus Nerve Stim – There are many you-tube videos on simple exercises and releases you can do even lying in bed with your eyes closed. A very popular series and some of my favorites are by Sukie Baxter who has very short and simple tips. One theory is that disease or trauma keeps our vagus nerve in a freeze or collapse response and these exercises help break up that pattern.
Myofascial Release – I even do this when resting in bed to any tight areas since the pressure is so minimal and gentle (less than the weight of a nickel!) and focuses on horizontally and gently stretching just the skin and holding until you feel small releases in your body. Craniosacral therapy is even more effective but requires someone who is professionally trained.
Spinal alignment – When unable to go to a chiropractor, I try to use a lumber support cushion or even a cervical pillow to help maintain alignment when sitting.
Breathing – I’ve found focusing initially on exhaling as much as possible allows a more natural and deep inhalation to occur with less effort and to be more relaxing.
Lymph flow – If you can’t get a professional lymph massage, you can learn gentle techniques online to do in bed, elevate legs above heart while resting, use breathing techniques, pump feet from time to time, etc. Our lymph system has no pump of it’s own, so using muscles, massage, compression, gravity and drinking plenty of fluids assists in ridding body of toxins
Oxygen – I had no idea of how restricted my air flow was from allergies until I started using a daily allergy nasal spray. It made such a difference! Also, make sure your iron levels are adequate since that may also help with oxygenation.
Mindfulness – Gently focussing on tight or painful areas can often help those areas to release on their own.
Heart and brain coherence – The Heart Math Institute website has free information on this technique. It sounds a little strange, but is backed by research and I’ve found it to be actually very helpful in getting my body and brain into a relaxed and healing state.
I hope these simple tips will help some of those who are unable to take advantage of all the great suggestions mentioned in the article above.
These are some great suggestions, thank you for sharing your experience!
As always, thanks for the blog, Cort, and all you do to keep us informed.
I have, from my first bout of serious illness (that turned out to be neuro-Lyme, after treatment I recovered), and old biofeedback/HRV machine from “Heart Math”. Like another commenter, I deteriorated after jab #4, booster #2… probable C didn’t help and I’m attwo years and counting…again.
So agree with the posters that want a cause and cure, but often wonder if they may be different from pt to pt. Good, old-fashioned antibiotics were my cure way back when, but I do want to mention an “intervention” that made a significant, if temporary, difference in the way that I felt and that was Cranio-Sacral work with two competent practitioners (I used two others that I saw no improvement). So..some of these strategies, while not cures, may help some of us to make it through challenging days.
An important thing to point out when doing short amounts of cold therapy, is that researchers found the benefit in healthy people still worked at higher temperatures than the insane ice filled tubs people get in.
The water temperature at a warmer 15°C still triggered the response. So no ice water baths needed.
This is good news for ME/CFS patients because less energy is lost trying to warm back up.
The key is in tricking the body it’s in a situation that it needs to respond to the cold.
I also found a less stressful way to get down to the 15° was gently reducing the dial on the shower in gradual stages. The body still shivers (but not violently) and you still get the benefits of kick starting the adrenals.
I noticed the days I’m incredibly weak, that reducing my shower to cold enough to induce gentle shivering, Are the days I can sometimes boost my energy enough to be able to do a few paced out chores.
Note: The length of time shivering is something you need to be very cautious with as shivering is a big user of energy. So be careful not to trigger PEM. Maybe best start at 20 or 30 seconds, or less for severe patients. If ok after your normal PEM delay, then you know can increase the time and try again.
I agree with gradually turning down the temperature. After a while, you’ll be surprised that you don’t even shiver like you once did. I focus the water on my head and brain stem and I notice a marked difference in my energy after I end my showers with a minute of colder water. Does not have to be frigid, as you’ve said. Everyone can do this one – at the end of your shower, try 10-15 seconds of merely cool water. Gradually turn down the temperature and increase the time with every shower. A big help.
Underwhelmed. A bunch of non drug treatment therapies we’re all familiar with that help NORMAL HEALTHY people? Wow. Nope. Sorry. Studies and articles like this giving them attention are NOT helpful to our cause, parts of which are UNTRUE for MECFS.
Not trying to be negative but this is something I would expect to read maybe 20 years ago. This is still the best we have? Again, publishing things like this causes more damage than help.
I love and respect your work and all you do. Nothing against you or the blog.
Felt compelled to comment because it’s time for new advancements.
This is just sad.
Shea, I think you misunderstood. These are therapies that have helped people with ME/CFS, not just healthy people. That said, not every therapy helps everyone and you may have to do efor several weeks or months before you get an effect. I do vagus nerve stimulation and exercises, red and NIR light, neurosomatic exercises, meditation, etc along with LDN, propranolol, gabapentin and other meds. If each one helps me get 5% better, then it really adds up to a significant improvement
Landmark: an event, discovery, or change marking an important stage or turning point in something.
Is this really the word being used in the title of this study?
Do you believe this marks a turning point in MECFS?
Apparently the authors do.
I sure don’t.
Yes I do – because this study once and for all validates the 2-day exercise studies which show that exercise one day inhibits the ability to produce energy the next day. So far ME/CFS is the only disease to show that.
It would be really good if researchers tried a 3 day CPET, or a day between 2 CPETS. As someone else pointed out, the biggest crash comes after the second test. My PEM has always been worse two or more days after overexerting. I don’t think these 2 day CPETs are nearly capturing the full PEM in many cases. Why isn’t anyone testing more than 2 days as it’s known the delay can be longer. So frustrating, money could be better spent and results could be much more revealing and helpful.
All of these treatment/management strategies are also being used for fibromyalgia, particularly myofascial release therapy, breathing, and mindfulness to calm the ANS. So once again, I argue that fibromyalgia should be grouped with ME/CFS and long COVID, at least in this context.
Hej Curt
thank you for this so relevant and exiting subject. I have long time used breathwork in relation to pain, it dosent cure but help me so much. Its so relevant with the autonomic nervesystem regulation for ME, and also ways it can influence on imunune system
Thank you very much, Cort, for the article. It confirms for me the powerful effects of cold exposure, that I have discovered. (I have had mild to moderate CFS/ME since 2018.)
Last winter, I was fortunate enough to go to Switzerland with my family. I would take mini walks in the snow, a few minutes at a time, and stay close to the holiday home. I can always sense when I’m approaching my limit. Normally, I have to rest after just a few minutes of walking or cycling.
But this time, that limit never came. Within half a week, I was able to walk for about two to three hours without experiencing PEM! My hypersensitivity to mental stimuli and noise also decreased. Unfortunately, the effect didn’t last after the holidays.
The same phenomenon happens when it freezes in our own country. I can build up to skating for a few hours a day within half a week. However, the effect quickly fades when the temperatures rise.
This positive effect of cold exposure, in my opinion, has several causes: reduction of low-grade inflammation, improvement of blood circulation, and activation of the parasympathetic nervous system. These may not be new perspectives, but it does suggest that PEM is, to some extent, dependent on these three elements!
Interesting. Thanks for sharing that!
I experience the same, especially if its my head thats really cold. I can do so much more activity and actually feel invigorated when its cold and snowy out (most of the time but not always, sometimes my system is just toooo out of whack for even the cold to help, then it can actually be really painful).
If Im moving around a bit i can even be in a tshirt in freezing temps and feel great. The warmer it gets out, the less I am able to do/ more symptomatic i am; much over 70 degrees and I can barely step outside. Sometimes it feels like the cold temporarily ‘resets’ me, but i do crash from it sometimes too – its too easy to overdo it when i actually feel so good for a brief bit!
The company Cort talks about in the article may be Remedée labs. I know she wants to establish herself in the US. This French company markets a connected watch for pain in fibromyalgia by stimulating endorphins.
They did a study which included 170 fibro patients. 53% of patients went from severe to moderate within 3 months of treatment.
https://remedeelabs.com/en/fibromyalgia/
I tested the Remedée watch for my fatigue (I don’t really have any pain), but I quickly gave up because I felt worse.
It is not a connected watch, but a connected bracelet. Sorry.
Before anyone launches into massage with the aim of improving circulation, I suggest reading the excellent Pain Science website.
https://www.painscience.com/articles/massage-and-circulation.php
Thanks for this, Cort. Having mast cell disorder, I find most medications are not available to me for POTS, EDS & ME. I wonder if something like this was in the minds of the researchers in deciding to examine non-drug treatments?
Apart from BFR I have experienced everything on the list and felt some benefit. Unfortunately you need a level of fitness and support to engage with most of them. Perrin Technique helped me back to nearly normal during the 1st 10 years and I feel shifted some symptoms that never returned over the next 20 years.
The relapses as a result of infections (Lyme & co., typhoid) and unhelpful medical treatments have been devastating and show how precarious any ‘improvements’ are. The underlying disorder is still present and ready to pull apart the painstaking improvements almost overnight.
These treatments are tweaking round the edges and act as slow, tough, incremental recovery if you can manage to do them. I think most chronic illnesses would benefit in a similar manner. I always felt I had to have the focus and commitment of an Olympic athlete to make any progress with them. I suppose it is helpful that research is catching up with what we have all been practicing for years. I have been glad to have them but I wish after all these years the researchers were able to move further on than this to uncover something specific and fundamental about our disorders.
Thanks so much for this blog, Cort! Been looking forward to it with baited breath! 🙂
Finally got done!
For fascias, I use kinesiotaping bands. It’s very effective in reducing pain and tension. But it’s not always easy to find a trained professional.
I learnt the technique from professional and consumer books.
If you’re talking kt tape, I do that too to support my hypermobile joints, and find it very helpful. I found easy enough to learn to do it myself from YouTube videos.
Yes.
I use the German brand Pinotape, which offers a reference for sensitive skin.
In France, the technique is little known, and it’s a good thing the videos are accessible, but for non-English speakers it’s not easy to understand everything.
Potential drug free solutions or any real help at all is pretty much a rarity so, thank you! If I took the drugs each specialist recommended I wouldn’t even be able to function by now. There is a problem getting Drs to prescribe treatments for Long Covid symptoms because “there are no treatment protocols.” Without that you can’t get treatment and insurance doesn’t cover.
I’m surprised the (free forever) app, Visible: Pacing For Illness, was not mentioned. It’s an outstanding pacing tool! I’ve used it for well over a year and have seen a significant reduction in crashes.
It gives a stability score as a guide for the day based on Resting HR, HRV, and the previous bedtime symptom symptom tracker. Symptom tracker covers 3 important areas: symptoms, exertion, other factors. Of course, one still has to listen to their body throughout the day because our body’s response can change. (There is also a wearable device subscription that communicates with the app available – for which insurance coverage is a goal.)
Happy I read this. I limit my reads lately because I’m drowning in studies, research, outdated information, opinions, & even some ludicrous solutions.
Thanks
Yes! I may have learned about Visible on this page. It has been very helpful to me. Not only has it taught me how to pace myself better, it also gives me a record so I can see if things are getting worse or better. On a rough day it can feel like, “I always feel this way and I have forever.” With Visible, I can see that this is not the case. Also very interesting when there are streaks of much better or much worse–what preceded those?
The PDF to print is helpful to that end. I find the reminder that Visible is only a guide to set our pace for the day and that we know our bodies best very important. At times, the stability score does not match how I’m feeling. Then know I need to pace differently than the score indicates. This is the best & only tool I’ve found to teach me the value of pacing. The team behind it has the goal of helping others. Many of them are living with the consequences of LC.
I have also found the Visible app with the continuous heart rate monitor to be essential for tracking what is going on with my body. All users are flabbergasted by how much energy it takes to shower❗ I used it to get a diagnosis of POTS. I also use it to determine if I am getting a reactivation of EBV, a slowly increasing, 2-3 weeks, resting heart rate. I wouldn’t have been able to see this otherwise. Then, 2 weeks of additional supplements will tamp it back to latency.
In addition, something I’ve utilized for years to free up fascia is Essentrics (formerly know as Classical Stretch) based on the essentric method is an important gentle stretching & strengthening resource for addressing fascia issues. Routines for every need, including Post Covid. Available via video ( from public library or purchase online) or streaming, also some on uTube.
The only thing that works for me is 7mls of naltrexone every 2 hrs, but yes I do alternate nostril breathing, pacing, mindfulness, massage, grounding, vagus etc, but without the naltrexone I’d be dead. I am Kundalini awakened, and I’ve tried everything.
I would like to clarify that caffiene is also an important part in my naltrexone protocol , Thanks Vanessa
This is very disappointing to me. I’ve had ME/CFS for 30 years and I’ve tried nearly ALL of these treatments on my own up to 30 years ago. Some were relaxing, some had some benefits to life in general (stress relief, body care), but none had any real or noticable impact on my ME/CFS. I still continued to decline for 30 years despite continuing many of these practices for 20+ years. Now I have been too severe to leave my home for 10 years. I even had to stop getting massages at home bc they started giving me PEM for weeks each massage. That is not a positive influence.
I don’t think it takes a team of specialists to come up with a list like this. The fascia work, craniosacrail therapy, mindfullness, breathing techniques, massage, TENs, acupuncture, compression garments, physical therapy, personal trainers, chiropractic care, stretching, nutrition support, yoga, core work, etc etc were all on my generic list of treatments since 1994 when i was 18. But, I haven’t tried the ice bath.
I don’t believe they have had ANY influence on the majority of my ME/CFS symptoms. Maybe 1/20 of them. It would be interesting to see a list of which symptoms they believe are helped or “positively influenced” by these ideas. Maybe this list is designed for mild folks who can still get out of their homes to try these things and do physical therapy & tolerate massage, but I cannot.
I was really hoping for more than one new idea when I saw the article boasting such a long list of non-drug treatment ideas. But these have all been around and tried extensively with little benefit to me for decades.
Hello!
When I tried the modalities suggested here, they actually made me worse! I did not need even more adrenaline from cold water exposure, and physical therapy by an ‘expert’ led to even less ability, until I couldn’t even do the simple movements, and injuries, etc.
All but one: infrared light.
I first tried it with a hand therapist, for the terrible pain at the base of my thumbs and it was surprised thqt it worked.
I then moved on to sunbathing in the very early mornings, as much as my body could take. I would make sure to eat before hand, specially fruits, because otherwise my blood sugars would drop.
Infra/red light (from the sun) together with addressing my nutritional and hormonal deficiencies was how I got out of the deep ME/CFS state.
Sorry to hear. My experience is showing me that these modalities have varying effects for each person and are also very related to where one is in the ME/CFS process.
I started doing ice water dipping when I was first diagnosed but had to give it up, as it was too hard. Now two years later and lots of self-education, I’ve started again, in the ocean with less cold water (~ 16° C) and it’s wonderful.
Cold water exposure causes a stress response – adrenaline kicks in.
It feels great when you are on an adrenaline high.
I think it’s nutty to purposefully activate the stress response, healthy or not.
The sea has many other things going on that can be very good – the salt, the sun, the minerals, the CO2, grounding, etc.
I went to the shore every sunset for a year, and that helped greatly with getting sleepy after sunset (lifelong insomnia), in tandem with the nutritional and hormonal stuff.
One thing that I was not aware of until year 3 of ME/CFS was the tachycardia. I was diagnosed at 47 with ADHD and I take stimulants, so whenever my blood pressure and pulse were taken, the tachycardia was mistakenly attributed to Adderall.
I have heard credible researchers say that we are “potsy” and should explore this with our doctors. I use the Visible app which showed me, in under a week, that I have POTS. Propranolol lowered my heart rate and I immediately went from moderately severe, house and often bed bound, to mild.
Not everyone can take meds to control heart rate, but for anyone who hasn’t looked into it, it might be worth a look. Beta blockers are routinely prescribed for anxiety and high blood pressure, have been around for decades and have minimal side effects. I wish someone had suggested it to me a five years ago.
I had both a low AND a high heart rate, both low AND high blood pressure and my pulse pressire also varied wildy.
One doctor could could have killed me, because he prescribed meds for the highs – which would have made the lows even more dangerously so. I reasoned not to take the medication, and another doctor nearly fell of his chair when he saw what the other doctor did.
My lows disappeared with B vitamins. The highs came down considerably with calcium (milk), and then further with salt. (Prior to the milk, salt would spike everything up). I had been milk intolerant all my life and today I can drink 2 liters, eat cheese, ice-cream, etc. So it is possible to overcome it.
Ultimately thyroid supplementation normalized my heart.
Broda Barnes did the research on heart and thyroid.
Propanol works by lowering adrenaline.
Salt can also lower it.
By restricting salt intake, more damage can be caused.
If salt raises heart rate / blood pressure, it does so in the background of a calcium defficiency. Vitamin D and K participate in the homeostasis of calcium in the body.
The body can compensate for low metabolic / thyroid function with high adrenaline.
This is awesome! Focusing on what is most effective to leverage the body’s own fantastic recovery capabilities is something that our societies need a lot more of, instead of more drugs.
I’ve myself uncovered a number of these and am steadily (albeit slowly) improving. It’s wonderful to see that science is catching on and beginning to uncover what’s actually possible.
Many thanks for sharing this information!
I’ve used Oura ring for past 3 1/2 years and find the data invaluable in helping me stay honest about my condition.
I would (and often do) encourage absolutely anyone but especially anyone with chronic fatigue to try out the Alexander Technique with a reputable teacher. It ties into so much of this – core stability, myofascial release, vagus nerve stimulation, mindfulness… I know for sure that it increased the blood flow to my head and that after I had my breakthrough on it I felt clearer and less tired, all the time, and I have a lot more control over my pain and sensitivities now. It was a miracle for me and reading all of this stuff after having that experience is just validating. It’s a method to access all of the helpful things that your body can do for itself. It’s worth trying out, it gave me my life back and this is a list of things that it helps with, all without mentioning that you can access all of them at once.
A 5-minute cold water bath has been a tremendous help for my PEM.
Thanks for letting us know, Paul! A blog on cryotherapy is coming up 🙂
Since I started taking beet capsules I’ve been feeling better, I assume it’s due to the increased blood flow.
Thanks for this insightful article — the way you’ve pulled together non-drug strategies like breathing techniques, compression garments, and myofascial release for Myalgic encephalomyelitis/chronic fatigue syndrome is especially helpful!
THanks!