


Geoff’s Narrations
The Blog
The GIST
Canada can use some good news right now, and at least on the medical front, it got some with the fascinating “The gut microbiota promotes pain in fibromyalgia” study. The 40+ researcher study hailing from McGill and other Universities in Canada and one in Israel captured new ground.
 Health Rising’s Quickie Summer Donation Drive is On!
Health Rising’s Quickie Summer Donation Drive is On!Multiple studies suggest that something in the blood is causing or contributing to chronic fatigue syndrome (ME/CFS) and/or long COVID, but this is the first study to suggest that something lurking in the guts of fibromyalgia (FM) patients might have just as fundamental an impact.
Something in the guts of FM patients made mice look like they had FM.
Let’s not necessarily limit this finding to FM patients, though. This study was all about “nociplastic” pain – the kind of pain that also produces cognitive, sleep, sensory, and other problems, which means it may apply to other nociplastic pain diseases including ME/CFS, long COVID, irritable bowel syndrome, endometriosis, some subsets of rheumatoid arthritis, etc.
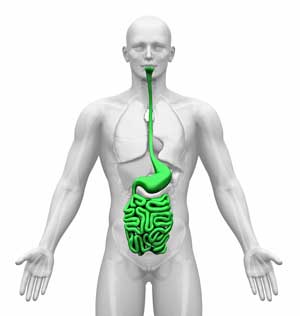
The gut, though, has always seemed kind of like a side issue. The authors, after all, started their explanation of FM with the central nervous system findings (altered neurotransmitter levels, neuroinflammation, dysregulated pain pathways) the condition is so well known for. The authors reminded us that the “gut-brain axis” affects the gut, immune system, and brain. The effects of gut flora on metabolites and metabolism and the high degree of nerve activity found in the gut indicate that the gut is a remarkably significant organ.
The gut is sometimes called “the second brain” because the “enteric nervous system” contained in it contains over 100 million nerve cells that operate independently of the brain. The gut makes its own serotonin and uses many of the neurotransmitters found in the brain to run itself. It’s in constant contact (and vice versa) with the brain via the vagus nerve.
The Study
Instead of transplanting serum, plasma, or antibodies from ME/CFS, fibromyalgia, or long-term COVID patients into mice or lab cultures, these researchers planted gut flora derived from fecal material donated by FM or healthy women into germ-free (bacteria-free) mice.
By the end of four weeks, the mice receiving the gut flora from healthy women were fine, but the mice whose guts were populated with FM flora displayed increased sensitivity to touch, heat, and cold. No signs of cognitive issues or muscle weakness were found. Surprisingly, the FM gut flora worked without producing any signs of leaky gut or inflammation. (Apparently, you don’t need to structurally damage the gut to cause these symptoms (at least in mice).)
Immune changes were reminiscent of what we’ve seen at times in ME/CFS and long COVID (increased classical monocytes, increased inflammation, decreased memory B-cells, and others.
Turning to metabolomics, increased spinal cord glutamine and brain glutamate levels suggested the FM patients’ gut flora had altered some fundamental nervous system metabolites. Decreased plasma medium—and long-chain fatty acids, branched-chain fatty acids, and dicarboxylate fatty acids fit perfectly with the fatty acid problems similar studies have found in ME/CFS.
The GIST
- Multiple studies suggest that something in the blood is causing or contributing to fibromyalgia, chronic fatigue syndrome (ME/CFS), and/or long COVID, and now, thanks to a Canadian study, it appears that something in the gut may be able to produce it as well.
- The gut is an incredibly significant organ, with its well-developed and separate (enteric) nervous system, its effect on the immune system, and its metabolism.
- When researchers transplanted gut flora from FM patients into mice, the mice looked like they had FM. Further testing revealed immune and metabolic changes (fatty acid issues) similar to those in ME/CFS and long COVID had occurred.
- The reduced bile acid levels were particularly interesting given recent similar findings in ME/CFS and long COVID. Bile acids are synthesized in the liver from cholesterol and then are modified by gut bacteria. Numerous potential connections between bile, ME/CFS, FM, and long COVID exist.
- Problems with bile production could contribute to things like neuroinflammation, inflammation in the gut, detoxification, problems with nervous system signaling (pain), and metabolic problems. In the end, bile issues could reflect liver problems—a possible emerging issue in these diseases.
- When ursodiol—an FDA-approved formulation of the bile acid ursodeoxycholic acid—was given to mice, it partially eliminated their pain sensitivity. Supplements such as TUDCA, ox bile or bile salts, taurine, choline, milk thistle, artichoke extract, dandelion root, and betaine (trimethylglycine) might also help with bile production. Efthymios started with 250 mg and gradually increased the dose to 750 mg to support his liver and ameliorate endoplasmic reticulum stress to recover from ME/CFS. (See his recovery story in the blog).
- An 8-week open-label fecal transplant trial in FM patients, which first used an antibiotic to clear the gut, found that new bacterial flora had taken hold, bile acid levels improved, and amino acids showed substantial changes. Pain intensity was reduced and anxiety, depression, sleep quality, and physical quality of life scores improved. A larger, placebo-controlled study is underway.
- The million-dollar question is where it all starts – the gut or the rest of the body. An AI engine (AI Perplexity) suggested that diseases like FM, ME/CFS, and long COVID could start in either place.
- It’s really something! Studies have found that something in the blood and now the gut can reproduce the symptoms seen in FM, ME/CFS, and long COVID in laboratory animals and in the lab! It was heartening to see how the immune and metabolic changes in the mice (B-cells, monocytes, inflammation, fatty acids, lipid dysregulation) mirrored so much of what we know about these diseases.
A Bilious Problem?
- A brownish-greenish-yellow substance produced by the liver and discharged into the duodenum where it helps with digestion; also an important detoxifications and signaling agent.
- An excess of bile was believed in the Middle Ages to result in irascibility and ill humour.
- In Hindu medicine, a “bilious temperament” is associated with increased irritability, a susceptibility to sweets, and rapid alcohol intoxication. (It is, however, caused by increased bile production.)

Bile problems could affect many systems. The liver, showing the various bile ducts. (Image by T Sheasby CC; Wikimedia Commons).
It was the reduced bile acid levels (reduced plasma ursocholate, increased fecal lithocholic acid sulphate), though, that really sparked things.
Bile is a fascinating new entrant into the ME/CFS, fibromyalgia, and long-COVID fields. Bile acids are synthesized in the liver from cholesterol and then are modified by gut bacteria. Numerous potential connections between bile, ME/CFS, FM, and long COVID exist.
Because bile binds to receptors across the body, including in the brain, immune cells, and metabolic tissues, problems with bile production could contribute to things like neuroinflammation and inflammation in the gut. Bile acids can activate sensory neurons, causing pain, or downregulate pain-producing pathways by stimulating opioid activity. Reduced bile levels can impair detoxification, resulting in fatigue, pain, etc.
Bile acid production problems appear associated with reducing butyrate-producing bacteria, intestinal inflammation, and fatty acid metabolism problems in ME/CFS. Reduced bile production has been speculated to impair tryptophan metabolism in these diseases, resulting in increased levels of neurotoxic metabolites (quinolinic acid), which produce fatigue and cognitive problems as well as serotonin synthesis (mood). In Germain’s study, the pathway with the highest “impact factor” was taurine, part of the primary bile acid biosynthesis pathway.
In the end, bile issues could reflect liver problems—a possible emerging issue in these diseases. Interestingly, mitochondrial issues that negatively impact the liver may also be implicated (more on that later).
Possible bile acid problems first showed up in a 2023 paper, “Altered serum bile acid profile in fibromyalgia is associated with specific gut microbiome changes and symptom severity“. The study found substantial bile acid changes in both bile-metabolizing gut bacteria and serum bile levels.
Alterations in one bile acid, α-muricholic acid, whose levels were highly correlated with pain and fatigue, appeared particularly significant. These detailed analyses, which uncover specific molecular entities that may have thrown major systems off, could lead to targeted treatments.
Fibromyalgia isn’t alone in its possible bile acid problems. Germain’s 2017 metabolomic study highlighted bile reductions in ME/CFS and signs of liver problems. After Xiong’s 2023 microbiome study found a reduction in bile acids, his 2025 BioMapAI study highlighted bile acids (among other factors). Turning to long COVID, both metabolomic and lipidomic analyses have found dysregulated bile acids.
Treatment Possibilities
With their own and the 2023 bile findings in hand, the Canadian researchers suggested that ursodiol—an FDA-approved formulation of the bile acid ursodeoxycholic acid—might help. When they gave it to the mice, it partially eliminated their pain sensitivity.
Interestingly, primary biliary cholangitis (formerly cirrhosis) (PBC) is one of the most fatiguing diseases known. In fact, Julia Newton, a UK ME/CFS researcher, came to ME/CFS via primary biliary cholangitis. The bile problems in PBC—where bile and toxin buildup cause scarring of the liver (fibrosis) and destruction of the bile ducts—far exceed those found in fibromyalgia, ME/CFS, and long COVID-19.
Still, the bile and liver problems that may be emerging in these diseases and the enormous fatigue in PBC suggest it’s worth a look. Like ME/CFS, addressing the fatigue in PBC has been difficult, but a recent drug called Iqirvo has recently helped both with fatigue and sleep. Iqirvo’s ability to reduce bile production may not fit in FM, ME/CFS, and long COVID, but with its ability to increase peroxisome activation via peroxisome receptors and enhance lipid metabolism – both of which have been implicated in ME/CFS – one wonders if there’s a fit somewhere.
Supplements such as TUDCA, ox Bile or bile Salts, taurine, choline, milk thistle, artichoke extract, dandelion root, and betaine (trimethylglycine) might also help with bile production. Bile acids are metabolized in the gut to ursodiol. During his recovery, Efthymios started with 250 mg and gradually increased the dose to 750 mg to support his liver and ameliorate endoplasmic reticulum stress.
Open Label Fecal Transplant Study Provides Some Benefits
Whether or not to first use antibiotics to clear the gut microflora prior to recolonizing the gut has been controversial. In this study, the FM-like mice given antibiotics first did much better than the mice simply given new flora. For example, the attempt at flora recolonization stuck and their pain sensitivity improved. FM-like mice given new flora alone did not show reductions in pain sensitivity.
Recolonizing the gut with healthier bacteria helped. Bigger studies are needed, and one is on its way.
The next step was obvious – give fecal bacteria from healthy women to women, each of whom had “severe, refractory,” (i.e., treatment-resistant) FM characterized by high levels of pain and fatigue. After being given oral antibiotics for 3 days (vancomycin 500 mg (Mylan, France) q6h and neomycin 1000 mg (Ma’ayan Haim, Israel); 24h clear liquid diet and bowel irrigation using polyethylene glycol 255 g (PEG, Taro, Israel), each participant received 30 healthy donor FMT capsules, the equivalent of 15 g. This was followed by four maintenance doses of 15 capsules each, taken 2 weeks apart, for a total duration of 8 weeks.
Stool samples indicated that the new bacterial flora had taken hold. Importantly, even nine weeks later, each participant’s gut flora still closely resembled their donor’s gut flora. Bile acids improved, and amino acids showed substantial changes.
Symptomatically, recolonizing their gut flora with healthier flora wasn’t a magical cure, but it did help. Pain intensity reduced by about 20%, and anxiety, depression, sleep quality, and physical quality of life scores improved. There was a trend towards improved hypersensitivity to heat. A larger, placebo-controlled study is underway.
Overall, fecal transplants are just beginning to be assessed in FM. A 6-month open label trial resulted in significantly improved symptom scores (widespread pain Index, symptom severity, hospital anxiety and depression scale, and Pittsburgh Sleep Quality) score as well as significant increases in serotonin (5-hydroxytryptamine) and gamma-aminobutyric acid levels (P < .001), and decreased levels of the neurotoxic neurotransmitter glutamate.
Small FMT trials in ME/CFS and long COVID have had mixed results, and key factors such as how many treatments are optimal are far from clear.
Fecal transplants appear to use a similar “flood the system” approach as IVIG, i.e., inserting lots of healthy bacteria or antibodies in an attempt to reset the system. Perhaps it would be far better to identify the specific bacterial and/or metabolic imbalances that need to be repaired and focus on those, and efforts to do that are underway.
In the end, personalized treatment may be the ticket. Ken Lassesen – a mathematician, software engineer, and citizen scientist with an MS in Operations Research and Statistics argues that the “One treatment treats them all” is the stuff of fantasy writers. After looking at dozens of microbiomes from ME/CFS and Long COVID, he’s found that each one is different and that gut changes over time must be addressed. (Studies suggest consistently broad alterations, such as butyrate depletion, exist.) Lassesen, who is not a doctor, created MicrobiomePrescription.com to provide more detailed treatment options.
The Starting Place…
Perplexity AI suggested that problems in the gut or elsewhere could explain the “something in the blood or gut” findings.
Perplexity AI suggested that problems in the gut or outside of the gut could start the process.
The million-dollar question is where it all starts – the gut or the rest of the body. Just for the heck of it, I asked Perplexity AI, “What is the likely source of a disease that can be transmitted to laboratory animals through blood, serum, or gut transplants?” Its suggestion—various viruses—didn’t seem particularly helpful.
Next, I asked, “How could gut microbiome alterations affect the blood so as to produce disease when the blood or serum is transplanted into laboratory animals?”, and got a more helpful response. Perplexity AI proposed that toxic metabolites, inflammatory factors, and autoantibodies that are produced in the gut could find their way into the blood or serum and produce disease when transplanted into laboratory animals.
On that note, Jason and Katz’s prospective study following college students who came down with infectious mononucleosis strongly implicated the gut. College students who experienced severe gut symptoms (pain, bloating, irritable bowel) at the time of their illness and low levels of IL-13 and IL-5 had nearly an 80% chance of coming down with ME/CFS 6 months later (!).
Lastly, I asked Perplexity AI: “How could factors not produced by the gut but are found in the serum or blood replicate disease by transferring the gut microbiome to laboratory animals?“. It stated that inflammatory factors, altered bile acids, autoantibodies, uremic toxins, and cortisol could all influence the gut flora in such a way as to cause it to produce disease when transplanted.
The gist is that Perplexity AI believes the process could start from either direction – the blood or the gut.
Conclusion
It’s really something! Studies have found that something in the blood and now the gut can reproduce the symptoms seen in FM, ME/CFS, and long COVID in laboratory animals and in the lab! Perhaps this is not surprising, given how intense and debilitating these diseases can be, but still… (What’s next—spinal fluid transplants?).
It was heartening to see how the immune and metabolic changes in the mice (B-cells, monocytes, inflammation, fatty acids, lipid dysregulation) mirrored so much of what we know about these diseases. While these diseases are very complex, and there are no easy answers, many of these studies—whether in FM, ME/CFS, or long COVID—seem to end up in familiar places—hovering around a simuilar suite of dysregulations, and that’s good to see as well.
Please Support Health Rising and Keep the Information Flowing


Wow Cort you’ve done it again, given me more ‘actionable intelligence’ with which to improve my condition re ME/FM than my family Dr, or even my supposed ME-specialist, apparently can.
After reading Efthymios’s recovery story earlier this year I became interested in the liver-ME overlap discussed there and asked my family Dr about TUDCA. He said he didn’t know about it but would ‘read up on it’. Although I keep asking if he’s read up on it at the start of each appointment, several appointments later it’s been pretty clear he’s not going to bother.
I started a small twice daily dose (50mg) of TUDCA recently, along with other supplement and herbal treatments such as dandelion and milk thistle seed, and now having revisited and expanded these issues in this article I plan to gradually increase to 250mg TUDCA. I have mysteriously elevated liver enzymes and am hoping to get them down as I know for sure they are implicated in my ME even though my Drs say they are completely seperate issues.
At the same time, your previous articles about viral reactivation fit very well with my own experience, such as Canadian blood services rejecting my blood donation based on findings of a viral presence that the local publicly funded labs can’t seem to pick up. Also I’ve had several classic symptoms of viral reactivation during PEM. And finally I experienced a temporary remission from my ME/FM after taking Paxlovid.
However my ME specialist from UBC says there is no evidence for the viral theory of ME and refuses to prescribe antivirals. This leaves me to experiment with herbs such as Cistus incanus in an attempt to tamp down viral activity. It’s a healthy polyphenol-rich daily tea in any case and now I’m growing it in the garden as a beautiful ornamental. But it probably wouldn’t be there without Health Rising.
In both cases the information in this blog has allowed me to move forward on my own, despite medical neglect, making informed cautious choices to explore various treatment options. It seems all Drs are good for is prescribing drugs to help with symptoms once the problem has been ignored and allowed to progress.
Your specialist is correct! There isn’t any convincing evidence on viral factors. It has been studied for more than 30 years, and nothing really convincing to show for all the research.
I am skeptical but not totally closed to the theory of viral perpetuating of the illness. Let’s see if Polybio’s trials of antivirals help. I doubt it, but we will see and I hope they do and I am proven wrong!
This has me wondering if the temporary remission from decades of ME/CFS I had after Covid, was from the Paxlovid and not the immune system resetting as I have been presuming. I soon deteriorated below baseline within a couple weeks anyway.
I wonder if Paxlovid targets more than just SARS-CoV-2, maybe it takes out other viruses hiding in reservoirs throughout the body. I’m aware the 2 week Paxlovid study was a failure in Long Covid. Yet some other studies have shown some patients have improved on extended Paxlovid treatment.
So I might try a longer month long course of Paxlovid to see what happens.
As I’m not on other medications, it’s actually very safe tolerable drug. As when toxicity testing was done
(normally 50% of the lab animals are killed via overdose to establish toxicity level. Called the LD50 test, Which is one of the most evil science tests done on innocent animals because it’s poisoning them to death over several days with no sedation).
However, when it came to Paxlovid toxicity testing in monkeys, they couldn’t overdose the animals. The dose was many times higher than the standard dose, yet the animals showed no adverse reactions. Meaning it’s quite a safe drug.
The only problem though is one of the two drug compounds in Paxlovid keeps other drugs in the system longer, it’s there so the anti-viral stays in the system longer . So there could be a dangerous buildup of a current medication if people are considering taking a long-term course of Paxlovid while they are on other medications.
But they can check the list of medications (which is extensive) to make sure they aren’t on a drug that will accumulate in the system while on Paxlovid. like heart medications for example do. With some drugs, patients can actually take a lower dose to balance it, and still get the same effect while on Paxlovid, but one would need to know the research on that to be sure.
So anyone thinking of taking an extended Paxlovid course, first talk to your doctor about the other medications you are on. Or look up that list yourself.
How to get hold of extra Paxlovid, tell your pharmacist or doctor wherever you get your medication from, that your whole family is sick with Covid. Sometimes they give you extra boxes for family members. Unfortunately, that all depends on what country you live in.
When I mentioned this new blog to my husband, he said “I told you so”. When I first got sick in 1984, I had horrible, horrible headaches which could be partially relieved by drinking a cold, slushy drink like an Italian icy. (A shot of heparin would knock out the headache also.) The effect of cold on the stomach suggests inflammation. My husband always said that my problems were focused in my stomach. The stomach-brain axis is well-known and the stomach has a big part of the immune system.
“The gut’s immune system, or gut-associated lymphoid tissue (GALT), is a crucial part of the body’s defense, housing a significant portion of the immune cells and interacting with the gut’s bacteria to maintain health and prevent infection. It protects against pathogens while also tolerating beneficial gut microbes and dietary antigens.”
Geoff, if ME/CFS is not viral, why would they prohibit blood donations from people who have it?
My contention has always been that ME/CFS is caused by HHV-6 A, which they claim not to have a universal test for. Balderdash! I am positive for it as is my daughter, but our tests were done through research labs.
Please don’t confuse HHV-6 A with HHV-6 B. Dr. Cheney thought that HHV-6 A was an entirely different virus and not a subset of HHV-6 B.
To further support my argument, metformin is being used in ME/CFS patients for its ability to suppress HHV-6 A.
“Metformin, a commonly used antidiabetic medication, has shown promise as a broad-spectrum antiviral agent, including against HHV-6A. Studies indicate that metformin inhibits HHV-6A replication in T cells by activating AMPK (AMP-activated protein kinase) and decreasing glycolysis, a process crucial for viral replication. HHV-6A infection actually reduces AMPK activity, which then leads to increased glycolysis and viral replication.”
Why would this be of interest if HHV-6A was not an important factor in ME/CFS?
I agree that hidden viruses may be underlying ME/CFS. Re: HHV6/AMPK are you familiar with this? I take or have taken about everything on the list. https://selfhacked.com/blog/natural-ampk-activators/ . If my Total IgG/HHV6 IgG #’s come back high again I think I’ll test for HHV-6A. Have you tested for ciHHV6?
I left an in-depth comment about my experience with TUDCA but when I submitted it said ‘duplicate comment – looks like you’ve already said that’ and erased it 🙁
Short version: TUDCA may also help ME directly due to immunomodulatory and mitochondrial effects…
Yup already started tudca and taurine with good results aprox.3 months ago.my stools are now brown in color as opposed to every color but brown prior to starting tudca.Sorry for the gross out lol.i also take milk thistle in powder form.
I also have been making my own l.reuteri yogurt as per dr.william Davis on youtube…and..make my own keifer.i buy the powder starter packs on Amazon. The l.reuteri starter is a bit tougher to find.
Dr.william Davis explains the l.reuteri will eventually push out the bad bacteria in the small intestine (Sibo).
He recommends making a couple other strains as well.its all on his youtube Chanel.Very jolly down to earth genuine human trying to do good in the world unlike the 35 yr.struggle I’ve endured with those other quacks…in it for the gain $$$
I have other chosen words but I’ll try holding myself back
Apart from stool colour – haha – in what way is Tudca helping?
My stools were not formed, lots of bouts of diaharea…now gone.
I do still have leaky gut…I know this because I have reactive arthritis but like the eff. Guy I stray from my strict diet just to see what happens.
My issue is different from some where I took 1.5 yrs of tetracycline for acne when I was 15 yrs of age but also I’ve been in three car accidents.pretty sure my microbiome is altered…had furry white tongue yrs ago…its gone now.
Now that I have my liver somewhat pumping out better bile I started a heavy metal detox as the specialist in Calgary advised. I’ve worked in a lot of jobs with chemicals,mercury…oil well fracking,steel foundry,taxidermist but I also believe mercury from dental amalgams plays a big role.its one of the most toxic elements known to man and its in our mouths
As per Ron Davis findings, I do have high levels of uranium….I live in saskatchewan, 🇨🇦 where one in 3 homes has radon gas.
I have one lung they found some damage. But since getting bad covid19 I had hundreds of lymph nodes the size of quarters inside my lungs…almost all gone now. I have this issue that when I pick up a bug etc ,my immune system goes nuts and right away I have a reaction in the form always of my lymph system producing large lumps in the weirdest places
I’ve had FM for 35 yrs. I had covid in September ’21 and again a month ago. Both times I had an improvement in FM. I didn’t take Paxlovid. My FM started after a minor car accident. Don’t understand the improvement in symptoms after Covid.
May I suggest you research Chlorine Dioxide. You have to go over to Rumble to find out about it because the powers that be have demonized it so badly. They use Chlorine Dioxide to purify water and blood for transfusions and transplants and it’s used in toothpaste and mouthwash. NASA called Chlorine Dioxide “The Universal Antidote”. It’s cheap and you can get it on Amazon . It comes in a two part kit. If you research on Rumble you will find out all about it and how to use it and peoples experiences with it.
I also use Monolaurin because it’s supposed to kills viruses and bacteria and mold and fungus.
I will also add that at my worst in 93′ there wasn’t one bit of eaten food that came out the other end digested.same with a vitamin…it came out exactly as it went in…whole.
Like whitney dafoe I stopped eating which in hindsight was not the thing to do but honestly to this day I never ever have my brain tell me my body needs food.its like I fell off the wheel of life and can’t get back on
Hi Cort. Amazing info! I’m too zonked today to take it all in. But what I was wondering is how you are doing lately. Are you still in bad shape or have you gone back to your usual baseline?
Thanks for asking. Ativan and Klonopin worked for a while, but at least for now, that has mostly stopped. A bunch has happened though which lead to some really strenuous days. Hopefully they will kick in again!
That’s too bad Cort. Sleep is so important. I take progesterone at night as well as Clonazepam but I doubt that would be the best thing for a man.
I just checked online and apparently Progesterone is used in men to improve sleep. It might be worth a try.
Thanks! Interesting idea 🙂
How much Taurine do you take? My bottle says 1000mg per day.
That’s what I take, 1/4tsp NOW powder.
I’ve been experimenting with something for the gut which seems to be helping my digestion. I read (or heard?) something years ago (can’t find it now) that said if you have lactose intolerance (I do, per genetic report), and you eat a little bit of dairy, your gut will produce bifidobacteria. After years of IBS-C and -D, years of avoiding dairy, years of non-stop crippling gut pain, especially after eating high-histamine foods or being exposed to mold, years of low to no bifidobacteria on stool tests, I have had textbook normal experiences in the bathroom for about three weeks. I don’t know if it will last and it hasn’t helped my fibromyalgia, but it’s amazing to me. I eat 2 T. of Bellwether Farms Plain Sheep’s Milk Yogurt (naturally A2) daily. When I first started, I had some pain (not crippling) which went away after a couple of days. If I eat more than 2 T., it hurts at first, but then the pain goes away again. Not sure it would work for everybody. Maybe I can find the original information on the lactose intolerance/bifido connection.
AI knows about the lactose intolerance/bifido connection, so I guess this is not new news. Here’s the AI link:
https://www.google.com/search?q=lactose+intolerance+and+eating+diary+helpfs+create+bifidobacteria&rlz=1C1VDKB_enUS1062US1062&oq=lactose+intolerance+and+eating+diary+helpfs+create+bifidobacteria&gs_lcrp=EgZjaHJvbWUyBggAEEUYOdIBCTE4MjA1ajBqNKgCALACAQ&sourceid=chrome&ie=UTF-8
You didn’t mention if you were casein intolerant. I’m assuming you know about it since you chose an A2 product for your experiment. I can eat 2T of goat cheese (A2) without issues as long as I take the DAO enzyme for histamine intolerance, I’m not lactose intolerant but A1 protein issues. My bifido levels are good as well. Glad this is helping!
I haven’t been tested for casein, but I thought A2 would be the wisest way to go. The only dairy product I’ve ever eaten that I have had no reaction to (and the tastiest) was raw goat cheese feta sold in small batches by a feed store in Houston. They stopped selling because of state laws, I believe, but those were good days. I may have to start taking DAO–I forgot that yogurt is fermented! If I go past 2 T., I have some histamine reactions.
Oh, I didn’t notice the yogurt either. Oops. Naturdao on Amazon is the cheapest and most potent. You can cut it into quarters or smaller. I take big or little “quarters” depending on the meal. The 10,000HDU “Hista….” versions are more expensive and never worked for me but might for you. They are more for people who aren’t histamine sensitive but want to drink too much and not be hung over the next day. 😉 Hope it works for you!
Also interestingly, if one goes to the DAMS (dental amalgam website)they write about detoxing mercury and how important supporting the liver while detoxing mercury.
Shortly after having my third molar removal us when my issues seemed to have started.
The dental surgeon didn’t bother to stitch the hole up and ive wondered ever since if that hole where the tooth came out may have infected and the infection migrated into the rest of my entire body,including my head. Dry socket?
It was one hellova a ride I went on years later in 1993
I’ve had FM for 40+ years. When it first started pain and sleep were the most pressing issues. I am much older now, and my gut and sleep are the main issues. I been taking Tudca with taurine and butyrate to help with my gut which is slowly improving. When my gut is improving, my sleep also seems to be improving as well. When I have a flare, both are terrible. I also notice increased neuro-inflammation at night. I get a stuffy nose and a terrible headache. When this happens, I take a B 6, which seems to help to reduce pain and inflammation. I also take probiotics and some digestive enzymes before meals. I mostly follow a somewhat modified FODMAP diet, which also seems to help as well. I tried HCL, but stomach didn’t tolerate it well.
This is really interesting for me. My central sensitory illnesses began in 1999 after my liver almost ruptured as a result of HELLP syndrome in my first pregnancy. The internalist said my liver would heal in 6 months, but in that time I developed IBS and have had less energy since (finally diagnosed with CFS/ME and POTS in 2020). I’ve been declining more quickly over the last 2 years, so am reading a lot more research. I’ll talk with Dr Arseneau about these medications and supplements.
I’ve often wondered whether to make my organs available if something happens to me. These studies make me lean towards NOT doing so- as I wouldn’t want to give anyone me/cfs!
Yeah, I took myself off the transplant list a few years ago for this 🙁 I keep meaning to see if I can find a way to donate the whole body to ME/CFS autopsy efforts once I’m done with it.
Interesting Kira, please keep us posted re what you find out 🙂
there’s this, but it’s only for Americans
https://www.meaction.net/2017/03/24/donate-your-brain-to-find-a-cure-for-mecfs/
Thanks!
I too came to the conclusion that my fibromyalgia symptoms were gut and liver related. I took a supplement that caused a mild liver injury three years ago. I developed fibro and sibo symptoms 9 months later. After much experimentation and research that lead me to high does Vit. B1, my fibro symptoms – pain, fatigue, light sensitivity, got much better. My gut problems however got worse and worse until I finally had my gall bladder removed 6 months ago. Many symptoms improved, but 3 months after surgery, sibo symptoms returned. After much additional research, I came to the conclusion that bile flow problems were likely all part of what was happening my fibro, sibo, and gall bladder. I started on TUDCA, milk thistle, and digestive enzymes, three weeks ago. The sibo symptoms are gone. Fingers crossed that this is the final piece of a long and challenging illness!
…and, just to add more info on liver health…consuming beat leaves is known to thin bile.
Only other way is to take a product called beet flow.
Apparently bile sludge or thickening of bile is pretty common
Hi Cort, This is just for you, not to be posted. I don’t want to be petty and I sure appreciate your work. I wanted to call out the photo at the top of the article of the woman in her underwear. I think it’s unnecessary. I’m not asking you to remove it. But would you post a frontal photo of a guy in his briefs pointing towards his stomach? I don’t mean to be a burden to your amazing effort, but I’m just asking you to think about posting such images in the future. In my opinion, they subtly perpetuate the objectification of the woman’s body.
Seconding this. The photo is really bothering me too. Could it be changed for something else, please?
Done!
Thank you!
Thanks, Barbara. The comment automatically got posted but it rang true with T and I imagine with others – and the photo has been replaced 🙂
You’re the best! Thanks for your kind response.
Can people who have had success with TUDCA please share their source and dose amounts?
Sure Birdie…ive only ever bought allmax brand 250 MG. Lately I’ve bumped up to taking 2 caps (500mg).the price is better on Amazon but the last bottle of allmax I bought they price matched at the vitamin store.i actually found 2 stores that said they would price match with Amazon. Here in saskatchewan, Canada I paid 46$ without tax
The taurine i take is now brand 500 MG. I only take one capsule.
Ive stuck with these brands because of the instant change that happened in my stool’s color from a variation of colors and textures, including lots of bouts of diaharea, to only brown and only one texture after supplementation.Thats enough proof to me.
About 20 min or so after taking tudca i get what feels like acid reflux but I believe its bile being released from the duct entering the gut.its very short lived
I have been taking Milk Thistle capsules for years in a bid to protect my liver. It certainly hasn’t helped my ME/CFS.
However a month ago I started taking Taurine. It hasn’t stopped my “crashes”, but it has cured me of dizziness every time I lie down or get up. I.have had this dizziness for 2 years, following one particularly bad crash / EBV reactivation.
Off topic, but this is a large and I think very important study by Systrom et al on PEM in ME/CFS and long covid.
Keen to see what they think is causing this. Also keen to see Systrom’s drug trial results in the not too distant future
https://www.atsjournals.org/doi/abs/10.1164/ajrccm.2025.211.Abstracts.A7881
I guess its official – however they got to their diseases ME/cFS and long COVID patients look the same during an exercise test. Pretty good!
Thanks Cort for this interesting article. Ever since I took tetracycline for acne more than 40 years ago, and then developed ME/CFS along with major gut issues, I’ve been painfully aware that the gut is central to ME/CFS, at least in my case.
I feel pretty normal until I eat breakfast. Then I crash, regardless of what I’ve eaten. I’ve tried every supplement known to man, as well as FMT, and nothing really moves the needle.
Bob…have you tried berberine?
Thank you for the suggestion. I’ll try it!
Hi Cort, first of all, how are you doing? Is your setback getting any better? It will surely be better again. Yes, the million dollar question… the gut… do you still remember the research of Meirleir? H2S gas in the intestines. This gas would disrupt the nervous system. I genuinely thought he had found the cause back then. Unfortunately, that turned out not to be the case. Nevertheless, the gut plays an important role in our illness. Almost every ME patient I know has often had issues with sensitive intestines before they got sick. I still don’t rule out enteroviruses as a (contributing) cause. Maybe we shouldn’t look at what is in the gut but rather at what is not there…
Something has helped improve my baseline and it was either CBD oil or choline, or both. I can see CBD helps my terrible goosebumpy dry skin a little (which a neurologist said is an indication of neuroinflammation??!) but reading this I think it’s the choline. I have tried TUDCA but haven’t noticed improvement with it. I had my gallbladder removed after I declined to housebound and I suspect taking Taurine completely stopped my attacks for a year. I’m sure this research is getting close to the answer, with some of us at least.
Thanks for this – really interesting. Since taking anti malaria tablets when I was 17, I’ve had pain and discomfort just under the bottom of my right rib – exactly where my gallbladder is. After eating I have a jammed up blocked feeling at that spot – it has a knock on effect on my mood, intestinal muscles and general exhaustion. At the time various tests were done for tropical diseases. Nothing showed up. Liver and gallstone tests were all normal. Even though the doctors wouldn’t believe me I know it was the tablets, as the diarrhoea started at the airport about 5 hours after taking my first tablet. It got progressively worse over the next 9 days until we decided I should stop taking them. Once home doctors told me the pain can’t be that bad get back to school, and it would be gone by Christmas. Of course it wasn’t gone by Christmas, and decades later I still have the same digestive symptoms. At its worst the pain is all over my liver – a violent sore pain, and my intestines are paralysed. Liver tests are always normal.
The digestive problems first started when I was 14 after having a general anaesthetic. At 16 my grandad died of bowel cancer so my mum had us all start eating wholemeal bread and more fruit, veg and legumess. That was back in the 1970s long before doctors realised it was positive to eat a high fibre diet. I remember my new diet feeling more comfortable, but it didn’t stop my symptoms continuing to gradually worsen. I was finally diagnosed with ME at 27. Since then I’ve tried elimination diets. None have helped. Various alternative practitioners insisted on giving me treatment to stimulate my liver – all made me worse.
My digestive symptoms are directly linked to my head – severe sinus problems and migraine type headaches. My body has been extremely sensitive to temperature since my teens – hot and cold.
I had depression for decades after the general anaesthetic – worse after eating. Doctors kept giving me antidepressants. Even tiny doses would make it worse – even suicidal. More recently I worked with an OT specialising in ME. She helped me understand that I needed to slow down my nervous system and brain – and use breathing to control the vegas nerve. Depression gone! Along the way I’ve found paracetamol and aspirin used sparingly also help relieve the paralysis.
I had a happy stress free childhood living in the countryside, so don’t believe stress caused my ME. I have the same tight jammed up pain by my eyes at the top of my nose – at it’s worst my nasal passages become so constricted I can’t breath through my nose. My immune system seems to be over sensitive to things I inhale and ingest. Are they mast cells? The sinus problems started a couple of years before the digestion problems.
Hi there – great article, but I take issue with the ethics of recommending TUDCA specifically as well as ox bile. Have you seen how the bile is harvested? It is disgusting and cruel. Part of my moral duty as a US-based family medicine doctor is to consider the far-reaching impact of the recommendations I make to patients. Food for thought.