


Geoff’s Narration
The GIST

Wirth and company have built on their original hypothesis paper with a string of follow-up papers. (Klaus Wirth at the 2025 Charite Conference)
Klaus J. Wirth is a kind of phenomenon. A German pulmonologist who spent most of his career working in the pharmacological field, Wirth has grabbed onto the ME/CFS field with both hands.
Prior to 2021, Wirth published papers on things like the alpha-2 adrenergic receptor drugs, drugs to treat sleep apnea, antiarrhythmic drugs, channel blockers, and class lc drugs. Nothing in his past suggested he would take on ME/CFS, but in 2021, something changed and working with Carmen Scheibenbogen and Matthias Lohn, Wirth began pouring out the greatest stream of hypothesis papers this disease has ever seen.
 Health Rising’s Quickie Summer Donation Drive is On!
Health Rising’s Quickie Summer Donation Drive is On!Since 2021, Wirth and colleagues have produced 8 hypothesis papers covering the skeletal muscles, neurological symptoms, the blood vessels, the microcirculation, etc., and recently an update on “Key Pathophysiological Role of Skeletal Muscle Disturbance in Post COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS): Accumulated Evidence“.
Plus, Wirth, a longtime pharmacological researcher, has found a drug (Mitodicure) he believes may be able to get at core problems in ME/CFS.
In 2025, Wirth presented his hypothesis at the Charite International ME/CFS conference.
Obvious Muscle Involvement
“Calcium overload and the consecutive impaired energy metabolism can well explain the exercise intolerance and PEM in ME/CFS.” The authors
Wirth and company went straight to the skeletal muscles to explain ME/CFS. Citing clinical findings, exercise testing, force assessments, handgrip strength tests, muscle biopsies, and imaging studies, Wirth and Scheibenbogen stated that “skeletal muscle involvement in long COVID and ME/CFS is obvious”.
The Gist
-

Wirth believes he has found a drug that could help. A blog on that is coming up.
Klaus J. Wirth is kind of a phenomenon. A German pulmonologist who spent most of his career working in the pharmacological field, Wirth has grabbed onto the ME/CFS field with both hands.
- In 2021, working with Carmen Scheibenbogen and Matthias Lohn, Wirth began pouring out the greatest stream of hypothesis papers this disease has ever seen. In 2025, Wirth presented his hypothesis at the Charite International ME/CFS conference (see presentation in the blog).
- Wirth and company believe that reduced blood flows start the process off, and studies suggest that blood flows to the muscles in this disease are imperiled in just about every way possible.
- The muscles respond to the low blood flows by relying on the ancient (and inefficient) process of anaerobic metabolism to produce energy. Anaerobic energy production (or glycolysis), however, produces lots of protons (H+) that acidify the muscles and need to be washed out.
- Something called the NHE1 (Na⁺/H⁺ ) exchanger gets rid of the hydrogen but leaves behind sodium ions. Because high intracellular sodium levels are detrimental in quite few ways, the cell brings in the Na+/K+-ATPase pump. Note the ATPase part, though. The pump requires a lot of energy to function, which ME/CFS cells may not have.
- If the pump gets too overloaded, it actually flips; i.e., instead of removing sodium, it begins importing calcium (Ca+2) into the cell and that’s when the trouble really starts. High calcium levels in the cell are like kryptonite to the mitochondria. ATP production takes a hit, the cells swell, and mitochondrial fragmentation, and even cell death can occur.
- As the mitochondria struggle for survival, they even begin consuming ATP instead of producing it. As damage to the Na+/K+-ATPase pump proceeds in the very severely ill, the muscles struggle to produce any force at all and the patient is left bedridden.
- With the mitochondria producing massive amounts of oxidative stress, what started as a virally induced blood flow problem is now a mitochondrial problem that is shutting down blood flows.
- The authors believe all the different types of ME/CFS probably converge on the same central problem: poor blood flows which trigger mitochondrial damage in the muscles in particular.
- They believe ME/CFS is an acquired (not inherited) ischemic (low oxygen environment) mitochondrial myopathy (mitochondrial damage) that they’re calling AIMM.
- In this scenario, where the disease is being driven by mitochondrial dysfunction, the original trigger hardly matters. What’s really needed is a way to get the blood flowing again, drop the intracellular sodium and ultimately the calcium levels in the muscle cells, and repair the mitochondria.
- Calling ME/CFS an enigma no longer, they believe “there is a good chance of novel highly efficacious drugs and even healing” can take place.
- Several studies could validate their hypothesis but maybe the conclusive way to do that would be to trial a treatment that increases blood flows, normalizes muscle pH, reduces muscle sodium and calcium levels (using muscle biopsies), reduces mitochondrial stress, improves exercise tolerance, and reduces PEM.
- Mestinon, which is under study now, may be able to do that in some people. Vericiguat is another drug that may be able to help as well.
- Klaus Wirth and Mitodicure has found a drug that may be able to help the sodium-potassium pump to produce ATP, reduce sodium levels, and prevent the calcium overload seen, thus allowing the mitochondria to regenerate.
- A talk with him on that drug is coming up.

Donation Drive Update – Last Week of the Drive

In the last week of our drive, we’re getting close.
Thanks to everyone who has contributed. In the last week of our drive, Health Rising is very near our goal. 🙂
Klaus Wirth, PhD is no stranger to Health Rising. Since 2021, Health Rising has produced no less than seven blogs on Wirth’s hypotheses (and another is soon to follow). Why? Because Wirth, Scheibenbogen, and Lohn have brought new and exciting perspectives to ME/CFS – and that’s something we don’t want to miss. If being up on the latest ideas regarding ME/CFS, fibromyalgia and/or long COVID appeals to you, please support us in the last week of our drive.
HEALTH RISING IS NOT A 501 (c) 3 NON-PROFIT
That’s a pretty obvious conclusion for anyone with these diseases, and, indeed, the reduced exercise production, rapid exhaustion, early entry into anaerobic energy production, and post-exertional malaise have made it clear that the muscles MUST be involved.
Poor blood flows start off the process.
Not so obvious, though, has been the cause, or pathomechanism, that’s been bollixing up the muscles, and here’s where Wirth et al., have dug deep, indeed.
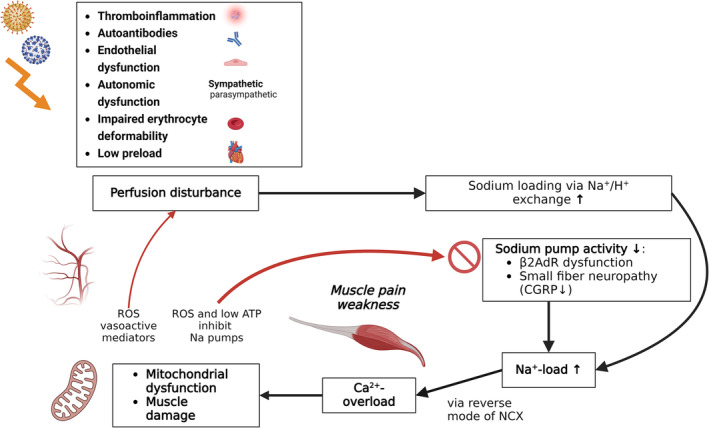
Key to their hypothesis is another factor high on the list of many researchers – reduced blood flows. Indeed, the list of possible blood flow problems in these diseases is staggering and includes inflammation, endothelial cell dysfunction, reduced perfusion into the microvascular blood vessels (small blood vessels), impaired red blood cell deformability, microclots, reduced preload, thickened basement membranes (unpublished), hemoglobin issues (unpublished) and reduced stroke volume.
If these findings are accurate, it would appear that blood flows to the muscles are imperiled in just about every way possible. That alone would be enough to severely disturb muscle functioning, but Wirth and Scheibenbogen add in further inhibiting factors: inflammation or viral infection in the skeletal muscles, and/or damage to mitochondria. Indeed, muscle biopsy studies have found evidence of muscle fiber death, immune cell infiltration, capillary loss, and basement membrane changes.
While the fly in the ointment in this field is always small study sizes, Wirth and Scheibenbogen were able to point to no less than 11 ME/CFS / long-COVID muscle biopsy studies that have found significant abnormalities (Table 2).
Wirth and Scheibenbogen presented several possible causes for the muscle problems found: inflammation in the muscles (remember immune cell infiltration), viral infection (not high on the list), autoantibodies (variable evidence), and damage by calcium overload (ka ching?) could all do it.
Interestingly, it all starts with low blood flows to the muscles (hypoperfusion). The muscles respond by relying on a backup system – the ancient (and inefficient) process of anaerobic metabolism to produce energy. Anaerobic energy production (or glycolysis), however, produces lots of protons (H+) which acidify the muscles and need to be washed out. (Lactate increases and needs to be washed out as well, but for a different reason).
Notice how many actions need to be taken to remedy that situation.
The Exchanger – First, an exchanger called NHE1 (Na⁺/H⁺ exchanger) exchanges one hydrogen atom (H+) out in return for allowing one sodium ion in. That takes care of the hydrogen problem, but now high intracellular sodium levels (Na+) can result. These sodium levels can leave muscle cells less resilient and able to produce force. Plus, because many of the transporters that bring vital nutrients (glucose, amino acids, phosphate) into the cell rely on the appropriate Na+ levels, high Na+ levels can inhibit nutrient flows into the cell. The cells can also begin bulging – which disrupts the receptors on the surface of the cell – inhibiting it from communicating with the outside world. The cell appears to become moribund; looking perhaps like a cell locked in a cell danger-like response.
The Na+/K+-ATPase Pump – The body, of course, is prepared for high intracellular Na+ levels, and it’s created the Na⁺/K⁺-ATPase pump to do just that. Wirth and Scheibenbogen, though, believe that people with ME/CFS are almost uniquely positioned for this pump to fail. First note that the Na+/K+-ATPase enzyme requires something ME/CFS and long-COVID cells presumably don’t have – energy, and lots of it – to function.
The Na+K+ATPase pump goes down.
Plus, high levels of oxidative stress, dysfunctional B2 adrenergic autoantibodies, and calcitonin‐gene–related peptide (CGRP) shortages caused by small fibre neuropathy could also be interfering with the pump. If things get really bad, the pump actually flips; i.e., instead of removing sodium, it begins importing calcium (Ca+2).
The mitochondrial calcium exchanger – Yet one more failsafe mechanism exists. The mitochondrial calcium exchanger should start pumping calcium out of the cells, but Wirth and Scheibenbogen believe that dysfunctional B2 adrenergic receptors and low CGRP levels knock it out in ME/CFS.
So does the mitochondrial calcium exchanger. (Wirth Charite 2025)
High intracellular Ca+2 levels are essentially the kiss of death for the mitochondria. By opening something called the mitochondrial permeability transition pore (mPTP), ATP production takes a hit, the cells swell, and can even rupture the outer mitochondrial membrane, trigger mitochondrial fragmentation, and even cell death.
Instead of producing ATP, the mitochondria begin consuming it.
If things get really bad, as the mitochondria struggle for survival, they begin consuming ATP instead of producing it. In this state, even small stresses can make the situation worse, and severe exercise intolerance is present.
And so it is a vicious circle. Low blood flows were already impairing mitochondrial production. Now, high intracellular calcium levels are impairing it even more – causing more reliance on anaerobic energy production, which produces more acid buildup, higher sodium levels, more impaired Na+/K+-ATPase activity, more calcium buildup, etc.
Over time, the damage accumulates as the pool of healthy mitochondria shrinks. The clearest evidence of mitochondrial damage comes from muscles which contain the highest loads of mitochondria in the body.
*Please note that intracellular sodium and calcium levels have nothing to do with your diet. From the paper “As calcium in the muscle cell is about 104 times lower than the ionic calcium concentration outside the cell membrane, cellular calcium overload does not result in changes in plasma calcium.”
Explaining the Really Severely Ill Patient
Wirth believes the most extreme endpoint of this process is a total loss of muscle force. He and Scheibenbogen may be the first to theoretically explain why some people are so impaired.
Nobody to this point has been able to explain why some people with ME/CFS or long COVID become so functionally impaired. Wirth believes he can.
Enter the sodium pump (Na+K+ATPase). Studies have shown that damage to the sodium pump can lead to depolarization (Wirth called it a “depolarization trap”) and a total loss of muscle force. Wirth believes depolarization occurs intermittently in the moderately ill, and is present all the time in the more severely ill patient.
At this point, the NCX is constantly importing calcium into the cell, leaving severely ill ME/CFS/long-COVID patients well and truly stuck. In this state, Wirth believes that even minor mental stressors can cause muscle symptoms.
While the poor blood vessel flows initially produced by the infection can be healed, the situation in the typical ME/CFS patient has become more difficult. Now the mitochondria are the main issue. Mitochondria always produce lots of oxidative stress, but damaged mitochondria produce even more – damaging the NA+K+ATPase pump and the blood vessels further. Now, in order to heal the blood flows, the broken mitochondria must be healed. The authors say it best:
“A probably initially predominant capillary‐microvascular disturbance is shifted into a mitochondrial‐vascular disturbance and explains why the disease cannot heal or even aggravates due to this self‐perpetuating mechanism as outlined below.”
And:
” a self‐reproducing mitochondrial dysfunction most likely constitutes the final and common disturbance of ME/CFS, which locks the patients in a vicious circle from which they can hardly escape.”
“AIMMING” at ME/CFS
Wirth and Scheibenbogen are confident that they’re on the right track. They believe that calcium overload triggered by high intracellular sodium levels “is the only explanation for tissue necroses and particularly mitochondrial damage in ME/CFS.” (Wirth believes that high muscle calcium levels are preventing muscle atrophy from occurring. Ron Davis has been surprised not to see more muscle atrophy in Whitney Dafoe).
The authors believe all the different types of ME/CFS probably converge on the same central problem: poor blood flows that trigger mitochondrial damage in the muscles in particular. They believe ME/CFS is an acquired (not inherited) ischemic (low oxygen environment) mitochondrial myopathy (mitochondrial damage) that they call AIMM.
There’s much to like about this hypothesis. It integrates the many potential blood vessel problems found (reduced preload, red blood cell deformability, endothelial damage, microclots) with mitochondrial damage and problems producing energy, and it explains how, via the vicious circle, people with ME/CFS/long COVID get stuck in a chronic illness state.
In the end, the mitochondria become the main drivers of ME/CFS.
This is because the authors believe a shift occurs over time. While the initial blood flow problems are likely caused by a viral-induced inflammation which usually resolves, other factors present in post-infectious illnesses prevent the healing from occurring. They include things like autoantibodies, hypermobility, dysfunctional genes regulating mitochondrial, vascular dysfunction, mast cell hyperactivity, and TRPM3 ion channel dysfunction.
In this scenario, where the disease is being driven by mitochondrial dysfunction, the original trigger hardly matters. What’s really needed is a way to get the blood flowing again, drop the intracellular sodium and ultimately the calcium levels in the muscle cells, and repair the mitochondria.
In the end, the authors believe a promising future for ME/CFS awaits. They believe the disease is now biologically explicable and treatment options are present.
“ME/CFS is no more an enigmatic disease for which therapeutic concepts are missing. Since the assumed disturbances are functional in nature and are treatable by appropriate agents, there is a good chance of novel highly efficacious drugs and even healing for this frequent and most debilitating disease. We appeal to politicians, pharmaceutical companies and stakeholders to support the rapid development of such promising new drugs.”
Validating the Hypothesis
We’ve seen that a number of results support this hypothesis, but as always with ME/CFS, the studies are usually small, and the question exists how to fully validate it.
Some ideas (ChatGPT supported)
- A large-scale exertion test that shows reduced perfusion/oxygenation, pH, increased intracellular Na+, reduced mitochondrial functioning, reduced strength (handgrip strength), and increased symptoms would be very helpful. This study could use ^31P-MRS to assess alterations in muscle mitochondrial functioning and muscle health. One study did find mitochondrial problems, but the study was small and reductions in mitochondrial functioning did not correlate with fatigue scores.
- Do in vitro or ex vivo studies of ME/CFS muscle fibers using fluorescent ion indicators (like Fura-2 for calcium or SBFI for sodium) to observe if calcium levels spike abnormally during and after an exercise challenge.
- Show that mitochondrial functioning and markers of injury (swelling, membrane potentials) are associated with high calcium loads. Because the TRPM3 ion channels regulate calcium handling, duplicating that finding in muscle cells would be helpful.
- Larger electron microscopy studies to confirm that the mitochondria found nearest where calcium enters the cells are the most affected.
- Assays of Na+/K+-ATPase activity in muscle biopsies from ME/CFS patients to determine if the pump is indeed failing. (With several muscle biopsy studies underway, this may already be being done?)
Best Shot – Clinical Trials
The most compelling evidence, however, would be an intervention that increases blood flows, normalizes muscle pH, reduces muscle sodium and calcium levels (using muscle biopsies), reduces mitochondrial stress, improves exercise tolerance, and reduces PEM.

Wirth believes he has found a drug that could help. A blog on that is coming up.
Clinical trials or animal models using NCX inhibitors (like KB-R7943) or agents that improve microcirculation (like Mestinon or Vericiguat), symptoms and mitochondrial output might be helpful. Mestinon has already been shown to quickly increase energy production, and the Open Medicine Foundation is conducting a large Mestinon clinical trial.
Vericiguat is currently being trialed in a nice, large (n=104) long COVID trial in Germany
Even more helpful would be trialing the Mitodocure drug that Wirth and company believe will be able to fix/ameliorate the exertion issues in ME/CFS. This drug would stimulate the sodium-potassium pump to produce ATP, reduce sodium levels, and prevent the calcium overload seen, thus allowing the mitochondria to regenerate.
That drug will be the subject of an upcoming talk with Klaus Wirth.
The Book
 Not many hypotheses inspire a book, but Wirth and company’s hypotheses have. Patrick Ussher’s book “U
Not many hypotheses inspire a book, but Wirth and company’s hypotheses have. Patrick Ussher’s book “U
‘I have been strongly impressed by the high scientific level of Patrick’s writings on ME/CFS, particularly considering his non-medical background and the short time that he could have worked on this area. I welcome the publication of his book which seeks particularly to explain the research by myself and Prof. Scheibenbogen in an accessible way for a patient audience, as well as talking about other facets of the illness and ways to improve quality of life.’ Klaus Wirth
Dr. Eleanor Stein is a big fan as well.
In this book, Patrick shares these transformative experiences alongside key insights into the ME/CFS research. His perspective offers invaluable guidance, providing both clarity and practical approaches that, in my opinion, have the potential to significantly improve the lives of others.
I wholeheartedly recommend this book to anyone seeking to enhance their quality of life or to better understand possible pathways to improvement for conditions like ME/CFS, Long COVID, or other post-acute infection syndromes. Patrick Ussher’s work is a beacon of hope, offering both scientific understanding and tangible solutions for those in need.”
Donation Drive Update – Last Week of the Drive
In the last week of our drive, we’re getting close.
Thanks to everyone who has contributed. In the last week of our drive, Health Rising is very near our goal. 🙂
Klaus Wirth, PhD is no stranger to Health Rising. Since 2021, Health Rising has produced no less than seven blogs on Wirth’s hypotheses (and another is soon to follow). Why? Because Wirth, Scheibenbogen, and Lohn have brought new and exciting perspectives to ME/CFS – and that’s something we don’t want to miss. If being up on the latest ideas regarding ME/CFS, fibromyalgia and/or long COVID appeals to you, please support us in the last week of our drive.
HEALTH RISING IS NOT A 501 (c) 3 NON-PROFIT


This is really exciting. Thanks for the hope!
Thank again, Cort! I appreciate all your information. It gives me hope for all of us. Happy to again this year be able to contribute to your great work in a small way.
Thanks so much Georgie 🙂
ME/CFS is widely known to be a descriptive collection of symptoms known as a “syndrome”, driven by multiple underlying dysfunctional biological and psychiatric systems.
Anybody claiming a single causal path and then, a breakthrough treatment, is peddling simplistic and unscientific false hope.
DecodeME showed there’s a biological signature associated with this syndrome though.
What do you mean “widely known?” You’ve apparently been out of the loop on this disease for the past decade or so. Here is the NIH description of ME/CFS: “Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), is a serious, chronic, complex, and systemic disease associated with neurological, immunological, autonomic, and energy metabolism dysfunction (Institute of Medicine, 2015).” The medical community has long since abandoned the misconception that there is a psychiatric component of this extremely debilitating disease.
“Neurological”.
That would that involve the brain? And the mind?
Psychological dysfunction is part of the picture. There is no need to get defensive; it’s not about blame.
“Neurological”
Yes. Systems in the brain are clearly involved.
Thus the mind and psychological dysfunction is involved — likely more secondarily (reactively) than primarily.
In either case there is no blame, so no need to get defensive.
Are you aware that the brain is not the same as the mind? The brain controls our muscles, breathing, heart rate, hormones…most of our bodily systems. Other neurological diseases include ALS, Parkinson’s, and MS. None of these are “driven by psychiatric systems,” though of course, like all serious illnesses, including ME/CFS, they affect our mind and mood. You must be aware that ME/CFS has been wrongly “psychologized” by the medical establishment for decades, and that this has done horrific harm to the entire patient population and to our hopes for effective treatment.
Thank you! Clear, direct and helpful answer. No one should have to go around the repeating loop of a psychiatric cause or significant involvement which has sidelined the scientific, biological research and treatment we need!
Did you even read the blog? Or did you just read the heading? When I read the heading I did think “Here we go again”, but reading the blog changed my mind.
Brian Keith: My understanding of their hypothesis is that they think there are many causal factors involved in creating the energy crisis in the muscle tissues in the first place. Different factors for different individuals. But that there are some very specific mechanisms that create a specific metabolic trap that, together with other individual factors, makes the energy crisis self-perpetuating. I would be very surprised if they think that 100 % of all diagnosed with ME/CFS is suffering from this, since the it’s only a syndrome diagnosis like you say. But they think it’s a central mechanism in making the disease chronic for a large part of the ME/CFS population.
I think it is ‘widely known’ that psychiatry is famous for simplistic solutions and peddling false hope . I can only presume that you are part of the discredited GET brigade.
I agree with you, Brian. I share your cynicism about these promised cures. . But it would be nice if we are pleasantly surprised.
Okay, but I am not “cynical”; just skeptical, based on past experience and the human tendency ( of patients who are suffering) to seek hope.
Hope is a good thing, but makes patients vulnerable to many highly questionable claims peddled by so many in the “alternative health care” industry. Bought a vagus nerve stimulator yet?
What Health Rising does is mostly stick to reputable science; not matter how slow and frustrating that can sometimes be.
I was using cynical in the same way that you are using the term skeptical,
Sorry to not be more precise. But I was trying to support your point of view.🤷♀️
Yes, thanks. I just wanted to be clear — I was not being critical of your comment.
I think scorning on vagus nerve stimulators, one of the few reasonable avenues available to pwME with little biomedical research and few clinical trials, when anecdotal reports abound, shows you are far removed from the patient community. I am assuming you are not a patient, or if you are, you’re unlikely to be one driven by intolerable suffering and need for relief to try things.
That’s the thing though, Mitodicure (while having not been tested on humans yet) IS based on reputable science. Any other “promised cure” hasn’t had a real comprehensive scientific rationale behind it. But the work behind Mitodicure makes a scary amount of sense.
So while it is still yet to be proven, it’s one of the best chances we have for an across the board disease modifying therapy for ME/CFS
I think you mean neurological not psychological!!!
Both, neurological and psychological.
Science (and philosophy) moved beyond mind-body dualism decades ago. For example, see Descartes’ Error (1994, A. Damasio).
To be clear, that does NOT mean one’s symptoms are “all in your head”. It does mean that in such a complex syndrome as ME/CFS, there is an element of interaction: psychological systems play a part — likely secondarily — and not just reactive to one’s experience of suffering.
This does not imply blame or shame, any more than one should shame a person who is experiencing symptoms of bipolar disorder or post-partum depression (to name two mental health disorders with a large known biological component).
May I ask if you’d already be familiar with current clinical diagnostic criteria for ME/CFS (CCC , ICC) and the key role of PEM (postexertional malaise) in defining the disease?
I disagree, I think there has to be a common mechanism to explain the common, distinctive and disease-defining symptom of post-exertional malaise (PEM) and exertion-related permanent deterioration over time (i.e. the more ME/CFS crashes happen, the tighter exertion limits get over time), but possibly different perpetuating factors of the disease in different people. All known different initial triggers also have in common that they are also immune events. So in my opinion, ME/CFS is probably a disease with a pathomechanism that has more than one tier, explaining why different patients respond to different treatments, but are all united by the distinct mechanism of PEM.
People who are new to this field often perceive the broad range of research as disparate; however following research for a few years I personally believe ME/CFS is likely a cascade regulation failure in the body. I.e., research has so far uncovered many areas of dysregulation in many parts of the ME/CFS multisystem disorde, but has so-to-say not yet found the very first domino to fall and cause a multisystem dysregulation failure.
By now, the first unifying theories emerge that link together the various research findings.
My personal current best guess hypothesis is for ME/CFS being a disease with a very strong epigenetic component, both in the initial trigger mechanism, and in push-crash-cycles. My guess is that a trigger event of systemic (immune) stress so-to-say flips an epigenetic switch to trigger ME/CFS, and possibly what flips that initial switch could be viruses that get reactivated by the initial immune stress event and – without necessarily replicating themselves – influence cell metabolism epigenetically at cell level (that’s something viruses do, as far as I know).
May I ask, are you the same Brian who commented below on psychology? In that case, I can add as someone who really likes psychology that from my own lived experience, psychological issues function in an entirely opposite manner from ME/CFS in daily life and are not causative of ME/CFS.
However, stress is both a known initial (co-)trigger for some ME/CFS patients (fitting in with the epigenetic hypothesis and with the commonality of immune triggers because of the connection between stress and immune systems), and also an important factor in illness management (Pacing).
However, to me the distinction is important that this different from classic psychosomatics assumptions of e.g. psychological beliefs or repressed feelings leading to symptoms (stress often gets vaguely subsumed under psychosomatics, leading to an in my opinion unfortunate commingling with the original meaning of psychosomatics) – I rather look at it from a viewpoint of stress medicine (i.e. the impacts of stress on the body system).
Of course an ME/CFS patient will feel a bit better if they manage stress in their lives or have a talk with a mental helpline to process/relieve emotions, simply their overall energy load on the system will be reduced, and also because many patients like me get strongly stress intolerant/adrenaline intolerant over time. I do not think any ME/CFS patient would dispute the role of stress management in disease management. But psychology as curative or part of the causative patchomechanism? Clearly no.
So if we’re talking psychology in this discussion, I feel that the best thing to avoid misunderstandings would be to specify as concretely as possible with examples how exactly we see psychology interact with ME/CFS.
Brian
I’m afraid that is a totally illogical statement
M.E. is NOT cfs.
cfs does not Scientifically EXIST.!
It’ S like a Doctor telling a Patient he has Chs → Chronic Heachache Syndrome
e,g Which could be caused by a hangover,, flu..indigestion,, heart problems,,, or even worse a Brain Tumour. or even psychological prob lems !
True M.E ,,, according to experienced researchers is nearly always triggered by a virus, and starts Very suddenly.
Fatigue ” syndromes ” can appear much more gradually.
Long Co vid proves this.
Hey Richard, JR here. ME/CFS can also start gradually, as in my case. However, key symptom for ME/CFS is PEM, and for a full ME/CFS diagnosis, fulfilling current clinical set of criteria including PEM, like CCC, ICC, IOM. I think the distinction to other fatigue syndromes is PEM, not gradual onset. The distinction is important to me, as I am one such case :-).
I did not initially fulfill full ME/CFS critera, but through repeated overexertion did progress into full ME/CFS over time (now severe ME/CFS). Articles by German ME/CFS researcher Scheibenbogen usually mentioned that both sudden and gradual onset exist for ME/CFS, and other initial triggers besides viral infection exist, and I’ve also heard from German patient organisations that other ME/CFS cases such as mine are known to them. Yesterday I learned that there is as of 2026 ICD an R-code for fatigue syndrome with PEM, but not (yet) fulfilling full ME/CFS.
Adding to what Richard wrote: I agree that ME/CFS is not equal to chronic fatigue as happens with other diseases, but the distinction from other chronic fatigue is made by existence of PEM (plus full set of ME/CFS clinical criteria including PEM), not by gradual onset. Though ME/CFS is very often sudden postviral onset, gradual onset does not exclude ME/CFS. See my rqeply to Richard also on new 2026 ICD R code for fatigue syndrom with PEM (but not yet full ME/CFS), which may progress into full ME/CFS.
Did you actually read and understand what was said the initial symptoms are or the initial root is mitochondrial dysfunction your body’s going to rack with many symptoms there’s not many pathways there’s only two things that cell does energy creation and exhaustion of the toxin or the reactive oxygen species read the article again nobody is peddling anything
You might be right. But its also simplistic to think your not wrong. Perhaps different subsets of patients, but the majority, are post viral. And without sounding rude, i couldnt care less about someone who says “i have Cfs, and its from trauma”. Ofcourse they likely have something else and a different cure path…. This is why many say “True ME”. Because so many join the “cfs” path because their GPs doagnose them with the syndrome. Without even knowing what ME is.
Hi.
I was about to make a donation via PayPal, until I noticed a $9 fee that’s not explained. It’s not a PayPal thing. Who gets that money?
Thanks for trying! There should not be ANY fee. (There is a small processing fee but it should not show up). Can you send what you saw to cortrising@gmail.com?
Cort, I’m confused – is there, or is there not, damage to muscles in ME/CFS?
Ref: https://www.healthrising.org/blog/2025/12/21/muscle-damage-me-cfs-muscle-repair/
Exactly my thought too. Am a bit confused. And I do have a problem to fit all the hypothesises together. Or apart 😉 .
Though I haven’t read this blog post all the way through so far.
I think myopathy in Wirth’s hypothesis refers to malfunctioning of the muscle tissue. It’s not a structural problem as far as I understand, and he thinks it’s reversible if some blockages in specific mechanisms could be resolved. The cells will then be able to clear the overload of sodium and calcium and revert back to normal functioning.
So it’s not muscle damage – in the same sense that is referred to in the header for the article about Hanson et al’s study. In that article they also talk about mitochondrial stress of the same kind that Wirth is referring to.
This article did mention that this process can cause cell damage (in the muscles, from my understanding). It just maybe reversible. I don’t have the bandwidth to re-read the otehr article, though I do remember some of it. And, basically, if I’m remembering right, it said that muscle damage that naturally occurs after exercise is not repairing itself in ME, whereas in healthy people that damage repair is what strengthens the muscle. But in ME, it causes deterioration. That would not be inconsistent with this article. (That said, I could also be remembering a different article. I read a lot & like I said, am really operating on low battery mode atm…actually just woke up & am having a particularly bad day.) So, ignore me if I’m getting it wrong.)
My understanding is that if blood flows can be restored and sodium removed the mitochondria should regenerate. They are continuously being removed and regenerated. They believe that the mitochondrial problems in ME/CFS are “acquired” – not genetically determined; hence they can be “de-acquired” :).
I think they’re saying that the impairments in ME/CFS prevent repair of muscles.
My limited understanding is that any sort of physical activity causes muscle damage, which then becomes the job of the immune system to repair. This is just the day-to-day way our muscles work.
The issues with blood flow in ME/CFS then prevent this repair from taking place. This lack of repair then leads to the high levels of physical dysfunction.
So it’s not that ME/CFS causes muscle damage, but that it’s renders the body unable to repair the muscle damage that results from physical activity.
Interesting, Cort. May they be right. Thanks for taking the time and making the effort to make sure we all know the developments.
IF they’re right, it will be proven. If not, well, we’re used to that.
I always have high calcium levels – so much so that they screened me for a type of cancer that can cause that (but the oncologist had my physician do another test before seeing me, and that was enough to disqualify the cancer hypothesis, so I never saw the oncologist).
I can’t take regular vitamin pills – they have calcium in them; I eat a lot of cheese, and have always thought that was the reason.
Who knows? Until the trials are performed, we won’t.
And then we’ll have to find out whether long-term damage can be reversed, or if all the useful stuff only applies for the new folk (and maybe the long covid folk); still desirable, but discouraging for the many of us who have been sick for decades.
Maybe 2026 will be the year.
Hyperparathyroidism?
I don’t think it has anything to do with your blood calcium levels. If I understand correctly, it’s the ion calcium channels that move calcium in and out of your cells.
Yes,ive read several times that changing your diet has nothing to do with this upset calcium curcuit
Makes sense – one wonders if they are connected in any way, though.
I was wondering about both the calcium & the sodium, because I normally have plenty of calcium, though my intake is abysmally low. And, I also normally have too low sodium, even though I try to take in extra. However, I know that I don’t fully understand the ion channel thing either.
That said, this is very interesting, & from what I can tell makes a lot of sense, other than that.
I should have put this in the blog and I just did. Intracellular sodium and calcium levels don’t have anything to do with your diet – which is why Klaus is not recommending any dietary changes to fix this problem.
Good to know
The trouble with this hypothesis is that healthy muscles exposed to the blood of cfs patients acts in the very same way.
There is no problem with our muscles; they’re likely just protecting themselves from poor perfusion.
It’d be interesting to see if the new drug helped in the model they made in this other recent article
https://www.healthrising.org/blog/2025/12/27/something-blood-me-cfs-long-covid-serum-muscles/
Dr Michelle James at Stanford has reported PET scans that show inflammation isolated in proximal muscles in MECFS patients. It would make sense that stressed mitochondria are the common denominator. PGC-1a (The peroxisome proliferator – activated receptor co-activator) is the master regulator for mitochondria. NF-kB,TNFa, and IL4 known to downregulate PGC-1a. The question is what is perpetuating this inflammatory cycle? Is it damaged endothelium/inadequate blood flow? Viral hit and run? Something in the blood? Smooth muscle of blood vessels dysfunctional?
Happy New Year Cort and to all readers.
So, it is Adenosine and K+, Na+, Cl− Imbalances after all.
Back in 2024 I wrote:
Introduction to Adenosine and Tachycardia https://swaresearch.blogspot.com/2024/04/introduction-to-adenosine.html
The Diagnostic and Clinical Relevance of Adenosine Testing https://swaresearch.blogspot.com/2024/06/the-diagnostic-and-clinical-relevance.html
It is also known that Adenosine deficiency can lead to severe combined immunodeficiency (SCID).
Diagnostic Tests for Muscle Fatigue: Uncovering K+, Na+, Cl− Imbalances and Na+-K+ Pump Dysfunction https://swaresearch.blogspot.com/2024/10/diagnostic-tests-for-muscle-fatigue.html
December 28, 2025,
Muscle Weakness: Causes, Viral Links, and the Physiology Behind Muscle Function
https://swaresearch.blogspot.com/2025/12/muscle-weakness-causes-viral-links-and.html
Thank you for listing those links again!
Can Wirth’s hypothesis explain brain fog?
Thanks for asking that. And sleep disturbance? And problems with speech?And Mast cell issues? And all the co-morbidities listed in the Bateman Horne clinician booklet?
Maybe it does but I wish someone would explain it to me- I’m pretty severe and can’t think through these things myself anymore…
I think their thinking is something like this: Everything starts with an energy crisis in the muscle cells caused by different factors. A lot of preexisting medical problems can contribute to that energy crisis, and also contribute to making it chronic. Their proposed mechanism is something that makes the muscle cells getting stuck in the energy crisis, not being able to gather enough energy to get back to normal functioning again.
As a consequence of the low energy stat the muscle cells don’t contribute to the whole body metabolism like they normally do (resting muscle cells normally play an important role in that). I suppose other organs also may get stuck in a low energy state. Anyway a lot of bodily functions get affected – both by other co-morbidities, and by the lack of available energy. Their hypothesis is that the chronic energy crisis in the muscle cells is what’s making it impossible for the body as a whole to heal.
Also, I think small-fiber neuropathy plays a part here, in connection to low blood flow. If I understand it correctly, if the nerves are not provided enough oxygen and nutrients, they can be damaged/die.
Small fiber neuropathy is connected to the autonomic nervous system, and can produce a whole host of symptoms in the automatic processes in the body – temperature, heartbeat, pain etc.
Small fiber neuropathy had been found in different studies in about 1/3 of ME/CFS-patients, about 1/2 in POTS-patients, and in around 40-50% of fibromyalgia-patients. A study found 60% occurrence in Long Covid. Whatever the exact numbers, quite high for all these illnesses.
There’s so many factors going on, but it seems convincing these findings might be a big part of the whole picture.
Combine that with Visser et als findings of low blood flow to the head, not enough blood gives too little oxygen and nutrients for vital systems in the brain.
Heightened oxidative and cellular stress also provides more toxin build-up, giving it’s own host of symptoms.
Yes, maybe Wirth et al are right that the impaired energy metabolism in the muscle cells is very much a core problem (at least for a large subset of ME/CFS) – fuelling an array of other problems like SFN, permeable barriers in the body, autonomic dysregulation and so on. Or maybe it’s just one of several negative loops that together keeps the whole system stuck in a dysfunctional state.
Yes, you make very good points.
I read a very interesting article by Komaroff in Cell. It outlined how many different dysfunctions all could become self-perpetuating circles by their own, and also fuel other self-perpetuating dysfunctions. It was eye-opening.
I do believe we are getting closer each day to finding things that work (even if it has to be many different things working at once), we’ve got to keep looking forward and try to fit the pieces together.
Here’s the article: “Causes of symptoms and symptom persistence in long COVID and myalgic encephalomyelitis/chronic fatigue syndrome”, Komaroff & Danzer, 2025.
https://www.cell.com/cell-reports-medicine/fulltext/S2666-3791(25)00332-5
Thank you, Tuva, for the link, very interesting article. They kind of try to map how all the different dysfunctions fit together in a system. Wirth’s mechanism easily could get incorporated into that system.
The article gives quite marginal space to deficits in cellular energy production – and mainly describes that as a direct effect from neural sickness responses. From my own experiences and some other persons I’ve followed there seem to be some chronic malfunction in cellular energy production that is relatively stable and doesn’t really follow systemic inflammation and sickness responses. Wirth’s mechanism fits perfectly in the system to complement regarding that.
I’m inclined to believe that Komaroff and Dantzer focus a bit too much on ”top-down” aspects of the system in their perspective. Maybe the activated neural sickness circuits are more of an effect of the chronic energy crisis in the cells than the cause. Maybe the brain stem is very correctly signaling this deep cellular energy crisis to the body – but the cells are unable to get out of the crisis. (Writh’s mechanism, cell danger response, etcetera.)
Thank you Michael.
Very helpful to me : )
Cort, the mention of ion channels reminded me of the research from Griffith University (Queensland, Australia).
Great question. And mental fatigue? It would be great if Cort could ask.
I like their hypothesis. But I wonder if a better one is the impact of brain inflammation and cytokines such as interleukin-6 signalling the muscles.
This also explains brain fog, mental fatigue etc.
My post was directed as a response to Kevin’s.
Yes, I want to know about brain fog, light sensitivity, etc too.
Thanks for raising this.
Taking this in slowly and don’t pretend to understand it all, but question as to how people think this intersects with POTs if yiu have that version of MECFS. We’re advised to take ALOT of slow sodium – could that be making things worse??? And I remember Ivabridine can affect Pitasdium levels, so Coukd Ivab also be making things worse in an underlying way?? Thoughts very welcome!
I will add this to the blog. These intracellular sodium and calcium problems have nothing to do with diet…which is why Klaus does not recommend dietary changes.
This sounds great its so good to hear of all the research going on and in the right places in the body. Thanks Cort for all your hard work in bringing it to us.
It is interesting to me that calcium came up, my three children are long term severe sufferers of ME. Though spending most of the last 30 odd years in bed they do not have any muscle wasting. What they do have is osteoperosis and of the severe and moderate suferers we know a lot of them have oesteoporosis too it seems to be common in ME people. I would be very interested to know if this fits in with the calcium theory
Duizelingwekkende informatie stapelt zich op, maar waar o waar blijven de biomarkers?!
Is lack of blood flow the reason a hot bath brings relief? I suffered a NAAION attack a few years ago for no apparent reason, lack of blood flow?? I do believe there is an element of stress involved, whether physical or mental. Thank you to all who continue this important quest
Reading all of this brings me two simple conclusions. I have been diagnosed with ME/CFS. One of the greatest helps to reduce muscle pain and give me more energy is a good medical massage. I believe it stimulates what my muscles should be involved with physiologically. It reduces stress. I live under very high stress from an alcoholic husband 89 years old. I’m unable to do any therapy to regain muscle strength as I have I’m unable to do any therapy to regain muscle strength as I have myofascial pain. Long story short when you have been married almost 50 years under these conditions which got worse with time and raised 4 boys. With no options for divorce, you live a long life of physical and stressful existence!
Glad to hear that massage is helping and sorry to hear about your living situation!
Now imagine: if poor blood flow can produce this profound a disaster in the muscle – how much greater must the impact of poor blood flow be in the brain? What i want to say with this: the focus of this hypothesis is perhaps a little too “muscle-centric” 😉
It’s interesting to compare and contrast your new research with the lates research on P.O.T.S.
Researchers at Virginia Commonwealth University and Columbia University may have discovered that benzodiazepines (I know, not directly pertinent to the above blog, but I’ll tie it in below) make people chronically ill by binding to the human mitochondrial tryptophan-rich sensory proteins (HsTSPO1), which is located on the outer mitochondrial membrane.
https://news.vcu.edu/article/2025/04/researchers-may-have-solved-decades-old-mystery-behind-benzodiazepine-side-effects
Advocate organizations, like the Benzodiazepine Information Coalition, have raised awareness concerning the potential for harm from chronic administration of benzodiazepines. These organizations have noted patients becoming ill with POTS, chronic pain, chronic fatigue, with some becoming house bound or even bed bound.
In light of the new research, these illnesses might, in part, be due to the drugs binding to HsTSPO1 (in addition to their binding on GABA receptors).
Google’s Gemini provided the following about how HsTSPO1 ties in with Wirth/Scheibenbogen’s hypothesis:
In the context of the Wirth/Scheibenbogen hypothesis (the AIMM model), the Translocator Protein (TSPO) is not just a potential issue—it may be a critical “regulator” that determines whether a cell survives the ionic stress or succumbs to the mitochondrial destruction they describe.While Wirth and Scheibenbogen’s primary focus has been on the sodium (1$Na^{+}$) and calcium (2$Ca^{2+}$) pumps, TSPO sits exactly where the most significant damage occurs: the outer mitochondrial membrane.3Here is how TSPO likely fits into the “Vicious Circle” of ME/CFS:1. The Calcium “Gatekeeper”The Wirth/Scheibenbogen hypothesis hinges on calcium overload inside the mitochondria. Research (notably a 2024–2025 focus) has shown that TSPO directly regulates mitochondrial $Ca^{2+}$ signaling.The Issue: When TSPO is overexpressed or dysfunctional, it can “prime” the mitochondria to be more sensitive to calcium.The Connection: In the AIMM model, when the $Na^{+}/K^{+}$ pumps fail and calcium floods the cell, TSPO may facilitate the “opening of the gates” that allow that calcium to enter and poison the mitochondria.2. The Link Between Neuroinflammation and Muscle FatigueTSPO is most famous in ME/CFS research as a biomarker for neuroinflammation.4 PET scans using TSPO-binding radioligands have consistently shown that ME/CFS patients have “activated” microglia (the brain’s immune cells).5Cross-Talk: TSPO is found in both the brain and the skeletal muscles. If TSPO is upregulated systemically due to chronic inflammation (the “trigger” Wirth mentions), it creates a state where the mitochondria in the muscles are less resilient to the ischemia (low oxygen) caused by exertion.3. Oxidative Stress and the “Permeability Pore”Wirth et al. describe mitochondria that eventually swell and fragment. This is the result of the Mitochondrial Permeability Transition Pore (mPTP) opening.TSPO’s Role: TSPO interacts with other proteins (like VDAC and ANT) to form the complex that regulates this pore. If TSPO is “stuck” in a high-stress state, it makes the pore more likely to pop open during exercise. Once it opens, the mitochondria lose their electrical potential, ATP production stops entirely, and the “crash” (PEM) becomes physical reality.4. Why this matters for TreatmentIf TSPO is a core part of the problem, it explains why traditional “mitochondrial cocktails” (like just taking CoQ10) often aren’t enough for ME/CFS patients.The Strategy: You don’t just need more “fuel” (ATP); you need to stabilize the membrane where TSPO lives.TSPO Modulators: There is emerging interest in TSPO ligands—drugs that bind to this protein to “calm it down.”6 Interestingly, some medications used off-label for ME/CFS may indirectly influence these mitochondrial membrane proteins.Summary of the TSPO ConnectionStep in Wirth HypothesisRole of TSPOResultIschemia (Low Oxygen)Senses cellular stressTriggers TSPO upregulationCalcium OverloadRegulates $Ca^{2+}$ entryAccelerates mitochondrial poisoningMitochondrial DamageControls the mPTP “Pore”Leads to mitochondrial swelling/deathSystemic PEMActs as an inflammatory markerLinks muscle failure to brain fogThe Bottom LineWhile Wirth and Scheibenbogen point to the sodium-potassium pump as the “engine” that fails, the Translocator Protein (TSPO) is likely the “structural support” that collapses under the strain. It is the bridge between the inflammatory state (seen on brain PET scans) and the mechanical failure (seen in muscle biopsies).
omy stephen,
ive been on clonazapam for years and i am very sick with m.e. do you know if i taper off it will my mitochondria recover from the effects? im exhausted and cant do much research. thank you for this post.
Kimberly, I don’t think everyone is affected the same by benzos, even with respect to the recent research revealing this class of drugs’ potential harmful effect on mitochondria. Some patients are seriously affected while others do not appear adversely effected. The decision to taper off a benzo is a very personal one to make in collaboration with your physician.
Generally speaking, the therapeutic effects of the benzos wane over the course of time, even for those who can discontinue without much trouble. If a patient chooses to discontinue, the Benzodiazepine Information Coalition and other advocacy organizations strongly recommend for individuals who are sensitive to reductions in the drug’s dose to discontinue via a micro-taper method. This might involve your doctor prescribing a compounded liquid prep of the drug in an oil based solution allowing for very small drops in dose over the course of several months. Otherwise, the lowest prescribed dose is 0.125 mg for clonazepam, which might be too large a drop in dose (especially at or near the end of a taper), than some people can tolerate. This website provides helpful information:
https://www.benzoinfo.com/tapering-help/
thank you for that stephen. great to hear it doesnt affect everyone’s mitochondria. ive been on and off for years now. i was currently taking .5 a few days a week but increased to .5 every day and took 1mg a few times this past week. my thinking was if emotional exertion triggers m.e. pem then maybe i should take my prescribed dose of 1.0 a day to stay calm hoping to avoid the emotional exertion link. but when i bumped up to 1mg for 2 days i started feeling sicker? so im thinking it may be making me worse. ive never correlated the two bc i was in a very difficult situation which kept me triggered therefore constant PEM. in the past i managed to wean myself of klonipon okay so i see how i do this time. a friend of mine is suggesting rhodiola rosea but i believe that cant be taken for an extended period of time. thank you for the link. i will check it out.
Interesting research. I have tried Mestinon and did not notice any improvement. If anything, it gave me headaches. I have small fiber neuropathy. The only intervention which seems to help is meditation and deep breathing. That leads me to believe my problems are more CNS related. Although I guess the small fiber neuropathy could be impacting my CNS. Either way, adjusting my blood flow via Mestinon didn’t work – for me.
!
Have Ana MIchalcea’s remarkable photos of the insides of our bodies, including blood vessels, with her fantastic microscope, contributed to our understanding of what is happening in our blood vessels? The pictures are so clear that she must have an interpretation she could offer us.
I don’t know but maybe she should be asked for her views.
Very cool stuff, thanks for bringing it to us Cort.
I never really understand the fixation on the muscles in this disease though. It’s a disease of exertion, but not strictly physical. How does this hypothesis explain PEM from cognitive, emotional, sensory exertion, etc?
what is the name of the mitodicure med wirth is saying may get to the core of m.e. problems? thank you for any help!
I don’t know much about the drug. I do know that it is not available. I believe its a novel compound. I’ll learn more on our talk.
cort,
can you get me in touch with researcher wirth? in your upcoming interview with him i want to know how i can become a participate in the phase 1 research trials for the mitodicure MDC002 drug.
thank you for all of your help
I’ll see how/if the trial is going and if it is I’ll provide the contact info on the blog 🙂
hello cort,
when you do your interview with dr. wirth, will you ask him how long does he thinks it is going to take to get his mitodicure med through phase 1 fda trials? i am a member of a support group with about 6,000 members so i might can help with getting pwM.E. to do the study if the registry doesnt already have enough people. thank you for all that you are doing to help us with one of the most complex and disabling disease that exists. 😇
How exactly can a viral trigger cause low blood flow and how is it maintained?
What about people who get MECFS from vaccines or physical trauma?
Hi
Hi Angel, sometimes you have to look around at other research to get answers.
For instance, HIV can cause low blood flow by damaging blood vessels, leading to issues like endothelial dysfunction (impaired vessel widening) and increased plaque buildup (atherosclerosis), which restricts blood flow, increasing risk for heart attack, stroke, and peripheral artery disease (PAD). Chronic inflammation from HIV is a key driver of this damage, affecting vessel flexibility and increasing clotting risk, even with well-controlled viral loads.
Then Covid: Patients with unhealthy endothelial cells — cells that line the inside of the heart and blood vessels — have a higher risk of heart failure, hospitalization, bypass surgery and death. The study, published online in JACC: Cardiovascular Imaging in August, is the first to link reduced blood flow and COVID-19.
And finally. ME/CFS…significant evidence shows endothelial dysfunction (damage/impairment to the inner lining of blood vessels) is a key feature in ME/CFS, impacting blood flow, oxygen delivery, and potentially causing symptoms like fatigue and brain fog, with research linking it to inflammation and post-viral issues, similar to Long COVID. Studies using metrics like flow-mediated dilation (FMD) show reduced vessel flexibility and impaired microvascular regulation in ME/CFS patients, suggesting vascular issues contribute to the disease’s complex puzzle.
Re. this blog, I am always troubled by researchers seeking to develop a medicine that their lab will profit from. That said, it will take years and years for clinical 2 and 3 studies if they can raise the funds.
Hello, thanks for your answer.
I understand, but why does the poor blood flow remains? I see could it happen as result from an accute immune response but why is it not repaired after it? In my case all my problems started after a vaccine so no chronic infection in my case.
Regarding the monetary incentive of researchers, all drugs are made with monetary intentions, we won’t have any otherwise.
Seeing the word “calcium” pop up again in this blog makes me think of your other blog on memantine showing up as a promising treatment. Thoughts?
How would things like mcas and heds fit into this though?
Wirth and Scheibenbogen believe that MCAS and hypermobility and other factors kind of lock ME/CFS in. There’s the initial process which occurs in everyone who has an infection and then there are extra factors like MCAS, hypermobility that cause people with ME/CFS to get stuck.
If my understanding is correct, skeletal muscle is build from fusing many smaller precursor cells into longer fibers.
See https://en.wikipedia.org/wiki/Myogenesis.
“Myogenesis is the formation of skeletal muscular tissue, particularly during embryonic development. Muscle fibers generally form through the fusion of precursor myoblasts into multinucleated fibers called myotubes.”
Now if I understand (difficult) recent muscle and ME/CFS research correctly, muscle exertion / training does create parts (sections) of these long fibers to go into necrosis or at least become very poor quality. Shortly after this exercising, in healthy people this activates a sizeable response from the immune system likely helping to clean these faulty segments out. Recent research hints to this not really happening in ME/CFS. Then follows a phase of repair. In healthy people that means ‘cut-out’ sections of dysfunctional muscle are replaced by new segments of better quality. Compare it to cutting out a bad link in an iron chain and replacing it with a new one.
A good but difficult paper on muscle repair is https://pmc.ncbi.nlm.nih.gov/articles/PMC7290814/
Now if I make the leap to hypermobility, that hints to people having too long connective tissue (like tendons) and maybe a bit too long muscles too. In my imagination, this sort of fits the above (in patients dysfunctional) renewal process of muscles too. Old sections in long fibers don’t get removed often enough and when new tissue is added it has chances to elong it rather then only filling the (few in ME/CFS?) gaps to largely retain the old structure.
Both (many, not all sub-) types of muscle and connective tissue have high renewal rates. So normally there is plenty of cutting out old parts and fixing new parts in the gaps. Testosteron helps at least muscle renewal rates, likely making men less prone to this.
Utterly fascinating!
Cort, do you think Klaus has anything to do with why Germany government has recently dedicated 500million euro to Long Covid, ME/CFS research?
I don’t know but I would think it can only have helped. The really fascinating thing, for me, about Wirth and Scheibenbogen’s hypotheses is that they keep building. First there was the original one – and then they kept finding things to tack onto it – hence 7 hypothesis papers so far. Not bad!
Pretty cool to see a new hypothesis that ties together man things I’ve learned from previous HR blogs over the years.
I wonder what sort of influence this hypothesis has on the work of OMF in selecting medications to use for their treatment trials in ME/CFS disease models in various lab animals. I’d like to think they’d be able to coordinate in some way, to enhance each other’s research.
Always like your interesting articles about various topics, but your title here definitely is misleading and polemic.
Wirth and Scheibenbogen do not propose that ME/CFS is primary a disease of muscle myopathy, but that the mitochondria are the main drivers of the disease and there are different, often immunological, reasons why the mitochondria can’t be repared.
I mean, the name of Wirths company which tries to find a treatment for ME/CFS is called MITOdicure for a reason.
Wirth is trying to develop a drug that will address the mitochondrial dysfunction. According to AI, MDC002, Mitodicure, is a novel oral drug in development by Mitodicure GmbH, targeting the underlying mitochondrial dysfunction, calcium overload, and sodium pump issues in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and related conditions like Long COVID.
cort, im hopeful in wirth’s hypothesis bc it seems to explains the list of findings other researchers have discovered in m.e. however, wirth does not mention the contributing role WASF3 has on mitocholdrial malfuntioning?
Another.
Sydney – Researchers at Australia’s Macquarie University have gained new insights into the physical changes in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).
Mapping the complexity of ME/CFS: Evidence for abnormal energy metabolism, altered immune profile, and vascular dysfunction
https://www.sciencedirect.com/science/article/pii/S2666379125005877?via%3Dihub
Fascinating study! Just produced a blog on it. 🙂
Cort, am I correct to assume Wirth’s hypothesis would also explain the “nanoneedle” findings? If so, this is a reason in support of the hypothesis.
Since you’ve reported on the replication of nanoneedle findings in the UK involving the University of Surrey https://www.healthrising.org/blog/2024/02/11/nanoneedle-chronic-fatigue-me-cfs/, a thesis has come out of Surrey on the topic: https://openresearch.surrey.ac.uk/esploro/outputs/doctoral/99893266002346: It states that “The dielectric and ζ-potential response of PBMCs to 1.5-hour hyperosmotic challenge differentiated ME/CFS donors from healthy controls with 81.80% sensitivity and 85.70% specificity. ”
Do you know if the UK research has resulted in more “nanoneedle” related publications since then?
Well, the state as described by Wirth is definitely how fee, (tight muscular exertion limits and muscular acidity).
With regards to the cellular sodium/calcium ion channel disruption: I have had great success using tissue salts as recommended by my ND (https://martinandpleasance.ca/products/comb-12) which are designed to correct cellular imbalances. Since starting on the salts just over 3 months ago, I’ve had the following improvements in my ME symptoms (which I’ve had for 30 years):
-almost complete recovery from orthostatic intolerance/electrolyte imbalance issues
– 60% reduction in requirements for HPA axis meds/supplements
-50% reduction in requirements for mitochondrial support supplements
-Improvement in gut symptoms
-Improvement in brain fog
They are inexpensive, and easily available, however, due to their significant effects, I would recommend working with an ND to monitor progress and dosage. I started out taking the maximum dosage and now take only 1 tablet per day.
Thank you for making this article! The work of Wirth and Schiebenbogen is by far the research that I’m most hopeful for in the ME/CFS world – both due to its mechanistic comprehensiveness, and how well it explains my own illness development and progression.
I got POTS after my COVID infection, and it took several months for ME/CFS to develop. In the first few months, I had a heightened Sedimentation rate in my body, implying that inflammation played a role initially before fading. It lines up scarily well with their inferences on how the disease develops.
I really hope for all of our sakes that Mitodicure works as intended for as many people as possible, and it comes to market as soon as possible.
THanks! An interview with Klaus on Mitodicure is coming up 🙂
One of the most effective drugs for me has been ranolazine. Two of its effects are to reduce intracellular sodium and calcium in cardiac muscle. Wonder what it does for skeletal muscles in this respect? It also may reduce brain inflammation be reducing inflammatory microglia activity. It seems to improves microcirculatory function in cardiac muscle and is used to treat angina.
Thank you for reporting 🙂 May I ask what specific improvements you had from this medication?
Energy, brain fog, mood as well as altitude intolerance.
This is plausible but not even mentioning SFN is weird because that’s what’s likely driving blood flow imbalance in us, driven by autoantibodies
Acquired epilepsy, also thought to be a case of adverse intra cellular conditions damaging mitochondria in a progressing “trap” scenario, comes to mind
Can be triggered by a collection of seemingly unrelated pathologies and brain injuries
Mechanism is still not actually understood
Hopefully doing this work of investigation and intervention for muscle, rather than brain, will be easier in some ways?
Perhaps also relevant, my own condition is able to mimic ME without perhaps actually being ME, and is partially treatable with anti seizure drugs (my migraines had a good, response to valproate although the therapeutic effect failed over time)
But my migraines turn out to be secondary to POTS
And my migraines took a long time to be established to a highly impairing severity. During which time I was unaware of the fact I had POTS which I assumed to just be problems with breathing and fatigue (and doctors assured was anxiety)
Muscles themselves are not such a notable feature of my disease. Although.the lactate is noticeable. Whatever it is about poor POTS perfusion that causes mitochondria to fail in muscles, appears to have broken in my brain/pain/gut/neurology before it broke my muscles’ mitochondria.
Now that I try to treat POTS and not push through it I hope I won’t get to full blown ME “touch wood”
I recall that Sarah Boothby is quite focused on the mitochondria as the cause of the gastrointestinal failure in ME
Whether or not that’s through neurology or more locally I am not sure
My gut only properly ceases to function as a result of worsening near continuous migraine states
Not pushing through POTS feels like the key for me personally
Although I wish it was easy to resolve the hemodynamic and perfusion issues (as this article seems to imply at a couple of points throughout) to prevent further damage
Thank you for the excellent article, Cort. ME/CFS patients are fortunate to have you breaking down studies and making them easier to understand.
This is just a tangent to a very small part of the article, but if you have an opinion, I would appreciate hearing it. I am interested in hydrogen rich water, but it looks like it may be counterproductive.
From the article: ” First, an exchanger called NHE1 (Na⁺/H⁺ exchanger) exchanges one hydrogen atom (H+) out in return for allowing one sodium ion in. That takes care of the hydrogen problem, but now high intracellular sodium levels (Na+) can result.”
Also, hydrogen rich water is supposed to be alkaline, but now I am reading that water with extra hydrogen electrons is acidic. I realize this question may fit in better in the article about Friedberg’s study, but that’s such an old thread that it seems as if there is no interest in it anymore.
Are calcium channel blockers used for HTN, dangerous for ME patients calcium issues? Also, how many PTH levels are done to look for hyperparathroidism, as contributing to the calcium transport issues.