


Geoff’s Narration
The GIST
It has a kind of futuristic aura about it. Clip a little device to your ear for 30 minutes or so a day and get better! It sounds too good to be true, but non-invasive vagus nerve stimulators are affecting the largest nerve in the body, which just happens to be the conduit for most of the immune signals entering the brain.
We tend to get locked into our own disorders, but the vagus nerve stimulation field far transcends ME/CFS, fibromyalgia, POTS, or long COVID. While invasive vagus nerve stimulation has been FDA-approved for epilepsy, migraine, and stroke, non-invasive vagus nerve stimulation is being investigated in many disorders, including Parkinson’s, Alzheimer’s, RA, metabolic (diabetes), and cardiovascular (various heart issues) disorders, as well as FM, ME/CFS, POTS, and IBS.
This wide breadth is not a surprise. Low heart rate variability – an indication of the sympathetic nervous system dominance which VNS attempts to tamp down – is found in an astounding number of diseases (including heart disease, metabolic disorders, neurological diseases, inflammatory and autoimmune diseases, sleep disorders, as well as ME/CFS, FM, and long COVID).

Low HRV levels are found across many diseases. It’s been called a “hub marker of network dysfunction”.
Hub Marker – The fact that low HRV is so common in ill health suggests autonomic nervous system dysfunctions may underlie many diseases. In diseases like heart failure, diabetes, and stroke, low HRV is associated with increased risk of death. Low HRV also tracks with increased inflammation, autonomic nervous system dysfunction, increased pain, and post-exertional malaise in many diseases. It’s no wonder that low HRV has been called a “hub marker of network dysfunction”.
Low HRV may affect so many diseases, in part, because of the stress that constant sympathetic drive puts on so many systems, including the heart, blood vessels, metabolism (insulin sensitivity), and immune system (inflammation).
Brain Connection – That’s not all, though. Note that low HRV also reflects an inability of the prefrontal cortex to control the highly reactive limbic system (insula, ACC, amygdala) which, in turn, regulates the autonomic nervous system. The result – increased levels of stress, emotional lability, difficulty focusing, etc.
Not surprisingly, most of the research in the brain has focused on psychiatric disorders, chronic pain and fatigue syndromes, substance abuse, and some neurological diseases (Parkinson’s, Alzheimer’s).
Recent research, though, indicates the same HRV-brain connection is occurring in autoimmune and inflammatory disorders. In rheumatoid arthritis (RA), lower HRV is linked with altered insula and anterior cingulate activity. (VNS has been able to normalize cytokine levels and restore the ability of the prefrontal cortex to reign in the insula in RA.) Note that these brain regions have been implicated many times in ME/CFS and FM.
Low HRV has been associated with similar brain regions in multiple sclerosis, systemic lupus erythematosus (SLE), Crohn’s Disease, and ulcerative colitis. Low HRV (i.e. vagus nerve insufficiency), then, is associated with the activation of parts of the brain that produce pain, stress, and impact mood.
Energy Production – One more possible impact of low HRV needs mentioning – energy production. Low HRV has been associated with reduced energy production, and increased declines in HRV after exertion in ME/CFS, reduced mitochondrial enzyme production in FM, and mitochondrial issues in multiple sclerosis, heart failure, Parkinson’s disease, etc.
Why might this be happening? Chronic sympathetic nervous system activation takes a lot of energy, plus mitochondrial diseases tend to show both low HRV and mitochondrial dysfunction; i.e. the two may run together. People lucky enough to improve from brain retraining problems my owe their success to tamping down the chronic sympathetic nervous system activation present.
The Gist
-

The Parasym device Dr. Natelson is using in his long-COVID study clips to the ear.
It has a kind of futuristic aura about it. Clip a little device to your ear for 30 minutes or so a day and get better! It sounds too good to be true, but non-invasive vagus nerve stimulators are affecting the largest nerve in the body, which just happens to be the conduit for most of the immune signals entering the brain.
- We tend to get locked into our own disorders, but vagus nerve stimulation is being investigated in many disorders, including Parkinson’s, Alzheimer’s, RA, metabolic (diabetes), and cardiovascular disorders (various heart issues), as well as FM, ME/CFS, POTS, and IBS.
- This not a surprise. Low heart rate variability – an indication of the sympathetic nervous system dominance which VNS attempts to tamp down – is found in an astounding number of diseases (including heart disease, metabolic disorders, neurological diseases, inflammatory and autoimmune diseases, sleep disorders, as well as ME/CFS, FM, and long COVID).
- Low HRV has been associated with increased inflammation, autonomic nervous system dysfunction, increased pain, stress (increased limbic system activity), and post-exertional malaise in many diseases. It has been called a “hub marker of network dysfunction”.
- Non-invasive vagus nerve stimulation (tVNS) devices work by delivering gentle electrical pulses to parts of the ear, which stimulate the parasympathetic nervous or “rest and digest” system, thus potentially reducing pain, improving mood and sleep, and decreasing stress and inflammation via activation of the cholinergic anti-inflammatory pathway.
- No one right now is presenting non-invasive VNS as “the answer” to these diseases. It may be able, however, to improve functioning and quality of life. Vagus nerve stimulation studies in fibromyalgia, POTS, and long COVID have, with some ups and downs, delivered good results.
- Dr. Natelson’s group at the Pain and Fatigue Center at Mt. Sinai is in the middle of a VNS long-COVID study and they are recruiting patients. Being in this study is easy. No need to see a doctor, check in at an office, undergo any painful procedures, or worry about significant side effects.
- Participants can live anywhere in the continental U.S., the study requires a phone/Zoom interview, and a documented COVID infection is required. You cannot have been hospitalized for long COVID, you must fulfill the 2015 case criteria for ME/CFS, and you cannot have a BMI over 30 or be pregnant.
- Once you qualify, the device is sent to you. Each person wears the device for 35 minutes/day in the morning for 12 weeks.
- With the NIH’s HEAL and SPARC projects doing deep, deep dives into the vagus nerve and actively looking for better VNS devices, the future of vagus nerve stimulation is bright. While the correct parameters (duration, frequency, pulse width, etc.) are still being developed, numerous devices can already be found in the US. (See blog.)
- On the subject of breathing, Dr. Natelson reported that an ME/CFS exercise study will be published showing that about 25% of people with ME/CFS are hyperventilating and another 25% have a breathing pattern likely to result in fatigue.
- He recommends an affordable CO2 device – the capnograph by Contec – to his patients to determine if they are overbreathing and emitting too much CO2.
- In conclusion, the field of vagus nerve stimulation has a lot going for it, and we should expect substantial advances to show up in the future.

Other Factors
While the vagus nerve is the primary controller of high frequency HRV (the frequency that seems to be primarily missing in ME/CFS/FM and long COVID, other factors (breathing patterns (slow and deep is better), increased sympathetic activity, baroreflexes, hormones, inflammation, aging, and brain regulation (prefrontal cortex, insula, amygdala) all affect HRV.
Note that problems with virtually all of these (breathing patterns (hyperventilation – another one), sympathetic nervous system activity, baroreflexes, inflammation, and those parts of the brain) have been found in these diseases.
How Non-invasive Nerve Stimulators Work

The Parasym device Dr. Natelson is using in his long-COVID study clips to the ear.
Auricular vagus nerve stimulation (tVNS) devices work by delivering gentle electrical pulses to parts of the ear, where the branches of the vagus nerve are accessible through the skin. The stimulation activates the parasympathetic nervous, or “rest and digest” system, thus potentially reducing pain, improving mood and sleep, and decreasing stress and inflammation via activation of the cholinergic anti-inflammatory pathway.
It does this by stimulating vagal nerve fibers that signal to the brainstem, and which then link to several parts of the central nervous system (locus coeruleus, hypothalamus, amygdala, hippocampus) that have been implicated in ME/CFS and FM. Several of these areas are involved in processing pain, fatigue, and autonomic nervous system regulation. Note that several of them fall in the limbic system, which appears to be poorly regulated in ME/CFS and FM.
PENFS – A similar approach called “auricular percutaneous electric nerve field stimulation” (PENFS) uses subdermal needles to target a “field of nerves” in the ear that impact pain, stress, and autonomic circuits. PENFS, interestingly, is FDA-cleared to treat disorders of the gut-brain interaction – which a recent study just implicated in ME/CFS. VNS, on the other hand, specifically targets the vagus nerve.
Vagus Nerve Stimulation (VNS) in Fibromyalgia, ME/CFS and Long COVID
The first VNS FM trial took place back in 2011 in FM. The results of the small trial, which involved implanting a device in the neck, were hopeful, with 5/13 patients no longer meeting the criteria for FM, and many were able to get off their opioid drugs. That seemed like pretty robust evidence that VNS could dramatically help at least a subset of FM patients, but the NIH was not willing to fund another trial, and with that, the invasive VNS trials in these diseases were over. (Dr. Natelson reported that a reviewer said, “If you can’t tell us how VNS works, even if it works like a charm, we’re not going to fund it.”)
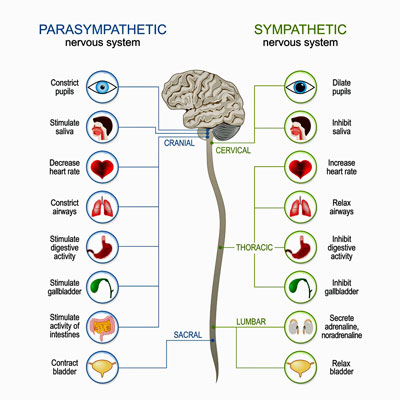
The goal is to rebalance the sympathetic and parasympathetic nervous systems.
Nine years later, the next FM trial comparing home-based exercise and home-based exercise plus non-invasive VNS did not find that VNS added much. A 2021 review of VNS musculoskeletal studies, though, found that small non-invasive VNS pilot studies decreased rheumatoid arthritis activity, fatigue in Sjogren’s Syndrome, and pain in FM. It also acknowledged that much doubt persisted about the best settings to use.
Next, a short 116-person 2-week Norwegian FM study did not find increased HRV or reductions in overall FM severity and current pain intensity. A 2025 25-person Italian study, though, found that twice-daily 30-minute tVNS sessions using the Nurosym™ device for 28 consecutive days resulted in significant improvements in autonomic scores (COMPASS-31), fibromyalgia impact scores (moderate reduction), and improvements in neuropathic-like symptoms and central sensitization.
Next, a 10-day (30-minute sessions, twice a day) 2024 trial of 24 female long-COVID patients also found significant improvements in cognition, anxiety, depression, and sleep, which remained or improved at the 1-month follow-up. Improvements in fatigue took longer but reached statistical significance one month after the trial had ended.
In a 2024 postural orthostatic tachycardia syndrome (POTS) study, one hour of VNS daily over a 2-month period resulted in increased HRV, reduced levels of adrenergic autoantibodies and inflammatory cytokines, and reduced heart rate levels. A review noted that while many questions remained (correct stimulation site, frequency, pulse width, intensity and duration) the study, nevertheless, brought “electrifying hope” to the POTS field. Another review agreed that while tVNS may be able to “enhance individualized care for POTS”, more “rigorous, high-quality research is needed to establish its long-term efficacy and safety”.
Clearly, we are just at the beginning of understanding what tVNS can and can’t do in these diseases. As we learn more about how to use these devices, and as improved devices appear, they should get more effective.
It should be noted that no one right now is presenting non-invasive VNS as “the answer” to these diseases. It may be able, however, to improve functioning and quality of life.
Long-COVID VNS Stimulation Study Underway
I talked with Dr. Ben Natelson about his long COVD tVNS study underway. He’s using the Parasym device made in the UK that clips to the ear. In an earlier pilot study, Dr. Natelson was surprised to see that a “bunch of them” got better. (It did not appear to help the more severely ill patients.)
Thus far, Natelson’s group at the Pain and Fatigue Center at Mt. Sinai has enrolled about 30 patients in the study, and they need 80-90. The great thing about the study is that it’s so easy. You can live anywhere in the continental U.S. It requires a phone/Zoom interview, and the device is sent to you.
You need to have a documented COVID infection, cannot have been hospitalized for long COVID, must fulfill the 2015 case criteria for ME/CFS, cannot have had ME/CFS prior to long COVID, cannot have a BMI over 30, be pregnant, be a cancer survivor, have had any type of neck surgery, or have an autoimmune disease.
The study lasts for 12 weeks. Each person wears the device for 35 minutes/day in the morning. During the first 6 weeks, each person will receive one of two settings. (Natelson is using the settings that worked in an atrial fibrillation study.)
During the second 6-week period, the device will use the most effective setting found in the first 6-week period. (Natelson believes that, ultimately, AI will be able to determine the best settings for each person.) Each person will also be asked to raise the current until it becomes uncomfortable and then back off. Everyone, then, will likely have slightly different currents.
Each person will also be trained in paced breathing, and the effects of the device on heart rate variability will be assessed. (Paced breathing stimulates the parasympathetic nervous system, aka the vagus nerve.)
“Can’t Lose” Study
I see this is a kind of a “can’t lose” study. You don’t have to see a doctor, check in at an office, undergo any painful procedures, do any work (other than wearing it for half an hour a day, and side effects, if any, are minimal. Past study results are generally good as well. tVNS won’t cure your long COVID, but it might give you more energy, help you sleep better, etc.
If you want to be in the study, contact:
- Name: Anna Norweg, PhD
- Phone Number: 212-844-6665
- Email: anna.norweg@mssm.edu
or
- Name: Patrick Quan
- Phone Number: 212-844-6665
- Email: Patrick.quan@mssm.edu
Breathing

Dr. Natelson’s latest study found that about a 1/4 of ME/CFS patients were “overbreathing” during exercise – causing their CO2 levels to drop.
On the subject of breathing, Dr. Natelson reported that an ME/CFS exercise study will be published showing that about 25% of people with ME/CFS are hyperventilating and another 25% have a breathing pattern likely to result in fatigue. He said he was surprised to find so much abnormality.
He noted that he asks new patients if they sigh or yawn a lot – a sign of overbreathing. The only way to know, though, is to hook them up to a CO2 monitor. It can tell them if they’re expelling too much CO2. (He recommends an affordable option – the capnograph by Contec. (The website says it’s for veterinary use, but the same model is marketed to hospitals.)
He uses a four-part breathing technique for people who are “moving too much air”. The breathing should be diaphragmatic – from the abdomen – not from the chest. This breathing technique, which is often practiced for 1-5 minutes, also stimulates the vagus nerve and is used by everyone from yoga instructors to Navy Seals.
- Inhale — slow, deep breath in (e.g., for 4 counts).
- Hold — gently hold the breath in (e.g., for 4 counts).
- Exhale — slow, controlled breath out (e.g., for 4 counts).
- Hold — pause at the bottom of the breath (lungs empty) (e.g., for 4 counts).
(Practitioners are increasingly recommending a 4-6 or 4-7-8 approach (in for four, out for six; in for four, hold for seven, out for eight) which emphasizes breathing out for longer than you breathe in).
More on Breathing and HRV
Check out how Hannah used heart rate variability to get better
The Future
We’re going to learn a lot more about how the vagus nerve functions and hopefully, vagus nerve stimulation, over the next couple of years.
Deep, Deep Dive Underway
The NIH’s HEAL Project, in collaboration with the NIH’s SPARC (Stimulating Peripheral Activity to Relieve Conditions) project, is doing a deep dive on the vagus nerve and how to manipulate it to reduce inflammation, pain, and other symptoms. The goal is to develop clarity on the mechanisms behind VNS and to identify biomarkers/endpoints that can effectively track its effects.
Among others, this includes an extensive mapping program to identify the specific nerve fibers the VNS is affecting, how to stimulate them effectively (duration, frequency, strength), and next-gen electrodes (e.g., injectable/soft interfaces) to provide more precise neuromodulation.
The $21 million Reveal study, for instance, is assessing how the autonomic, cardiovascular, metabolic, immune, and gastrointestinal systems respond to a broad range of VNS parameters. The SPARC program is now entirely focused on the vagus nerve and helping to develop better devices. The SPARC Neuromod Prize is a $10 million competition to develop more effective neuromodulatory devices. If this all works out, we should have VNS devices that are specifically tuned to target specific diseases/conditions.
This is the kind of basic research that the NIH does well, and it was no surprise that it was a congressional appropriation of $500 million that got the project going. It received over $600 million in the past year.
The big question is how well the ME/CFS, FM, and long-COVID fields will be able to piggyback on the results.
Many Trials Underway
A bevy of tVNS trials underway should give us more information on how effective these devices are.
- Long COVID – Long COVID tVNS trials are underway in Brazil, Turkey, Germany, France, and the New York one featured in this blog.
- Fibromyalgia – Fibromyalgia tVNS trials are underway in Georgia, Georgia (veterans), Charleston, Massachusetts; Boston, Massachusetts; Greece, and Egypt.
- POTS – A post-COVID tachycardia syndrome (COVID-induced POTS) is underway at Vanderbilt, a hypermobile EDS trial is underway in Wisconsin, and POTS trials are underway at the University of Calgary, Vienna, and Greece.
- ME/CFS – no ME/CFS trials (except for Natelson’s long COVID ME/CFS trials are underway).
Vagus Nerve Stimulation Breakthrough
The FDA, by the way, just approved the first implantable vagus nerve stimulation device for an immune disease – rheumatoid arthritis. Kevin Tracey’s Setpoint device can tamp down the inflammation in RA without the side effects associated with powerful immune drugs. Trials for multiple sclerosis and Crohn’s disease are planned.
Tracey talked about the “bioelectronics revolution” at the 2021 Dysautonomia Conference. He also recently published “
Non-Invasive Vagus Nerve Stimulation Devices Available in the US
In just a few years, the number of tVNS devices available in the US has shot up. This is what a recent search found:
-
-
- Parasym Nuropod model (seeking medical approval) — is now available in the US. Parasym is engaged in long COVID, POTS, and heart failure trials.
- GammaCore (medical approval) – FDA-cleared and commercially available in the United States, prescribed for several neurological indications related to headache and migraine.
- Nurosym (seeking medical approval) – A CE-marked and FDA NSR-designated transcutaneous auricular VNS (taVNS) device, clipped to the ear’s tragus, with medical approval in international markets and US sales in progress.
- Pulsetto (wellness device) – A non-invasive, wearable transcutaneous VNS (tVNS) device, applied to the neck and sold directly to consumers, is FCC-certified and available for use in wellness contexts such as stress reduction, sleep, and mood.
- Hoolest VeRelief (wellness device) – A compact, handheld tVNS device targeting the neck, marketed for acute stress relief and wellness but without full FDA approval as a medical treatment device.
- Apollo Neuro (wellness device) – A wrist-worn wearable using vibratory stimulation, marketed as vagus nerve stimulation for wellness, but not classified as a medical device in the US.
- Vagustim (wellness devices) – Consumer-targeted, non-invasive devices generally for relaxation and claimed wellness benefits.
-
Devices Pending or in Clinical Trials
-
- The Tivic Health Non-Invasive Cervical VNS Device (seeking medical approval) – is currently patent-pending and undergoing clinical studies in the US. Early data show measurable autonomic effects. Tivic aims for FDA approval upon completion of ongoing trials, with broad clinical indications anticipated.
-
- Check out Dr. Courtney Craig’s appraisal of the Neurostym model.
Conclusion

With much basic research underway, vagus nerve stimulation looks to be a growth field.
The non-invasive field of vagus nerve stimulation has a lot going for it. We know that invasive vagus nerve stimulation can work really well in some very difficult disorders, that non-invasive VNS is being widely studied, that both are getting institutional support via the HEAL and SPARC projects, and that past study results in these diseases have, with some ups and downs, generally been good, and that many studies are underway.
All in all, while there are still quite a few variables (pulse width, frequency, duration, etc.) that need to be worked out, and bigger studies are particularly needed in the ME/CFS, FM, and long-COVID fields, the tVNS future looks bright.
Support Health Rising – Keep the Information Flowing
Health Rising is not a 501 (c3) non-profit



There’s a British study as well.
I tried this for 4-5 weeks. No benefits as far as I could tell.
But that’s a sample size of one!
If I recall correctly that recently published patient reported treatment study didn’t show much benefit in this.
I tried the Nurosym device for 70 days and didn’t help me. I used it for 30-60 minutes a day. Maybe I should try again…
Thanks for this blog. I’ve been wondering for a while whether to try one of these devices, and which one to buy. As they are expensive and I react badly to everything I was hesitant about getting one. It’s obvious they help some people so may give it a go. I suspect it’s back to sub groups within ME as to who benefits from them.
I definitely over breathe. I can feel it. I do yoga breathing exercises and feel nice and relaxed, but it goes back out of balance when I do activity – mental or physical.
The patient community I’ve found most helpful is the “AVA A Vagus Adventure” group on FB. I was able to find a TENS device second-hand, along with a standard double ear clip I got online, to start TVNS therapy. They don’t really tell you how to titrate up other than to go slow to avoid PEM, but there’s a good research paper out there on which settings have been used in clinical trials. For instance, it’s different for every individual, but there are branches of the nerve that don’t get activated until you get to a certain threshold of mA intensity.
I use it every night and find it very helpful, if nothing else than for sleep quality. In my experience is absolutely best when combined with supportive strategies — like a weighted eye mask and doing breathing exercises while stimulating. Also, I’ve found that pre- and probiotics and NADH have been very complementary therapies to TVNS. It’s all been helping me a lot.
Yes, Vagus is the way, the thing with it is its a regular practice, all day ,everyday, exactly why monks om for long periods, I find regular short bursts the best, ear pulling, breathing techniques,yoga, humming and, special sounds Primal Trust teach you that work so well! All sorts of Somatic and brain retraining combined, Pattern interrupt, letting go, laughter yoga, full body stress relief and toning, the Vagus nerve is everything, when its shut down, you are are in dorsal vagal, cant do stuff etc, frozen when overactivated in parasympathetic, too much unchecked energy, goal is ventral vagal, calm, cool, collected, healthy, happy high vibe. Detachment, self awareness.
A very simple effective vagus exercise when stuck in dorsal vagal, is with both eyes look all the way the the left for up to 45 seconds, work yr way up over time, and then back to center ,then all the way to the right.
To add to the list, Cort, Alpha-stim
https://alpha-stim.com/product-category/alpha-stim-m/
Another, which I have, is the ZenoWell Luna. No prescription needed, easy to use.
Vagus nerve regulation techniques have helped me achieve a great deal of recovery from chronic pain and fatigue that was reached debilitating levels in June 2019 and cascaded downward until about 2.5 years ago. I found the work of David Deppeler at Breathe your truth. He hooked me to a capno trainer device helped me understand how much overbreathing I was doing. Over the last 2.5 years, I have learned to re-regulate the breath by reducing the hyperventilation, and it has been a game changer. If there was a non-invasive device that could help with this, that would be so much easier than the process I have gone through. I have had to relearn how to breath.
It hasn’t been easy but by the results have been noticeable over time and supplemented with other vagus nerve reset exercises including Alexander Technique, Acupuncture, postural work with a Chiropractor and also standard therapy to be able to keep spirits up to continue the slow and steady work of recovery.
Good luck to all those on this journey. Keep going.
I wonder what’s the cause for overbreathing in the first place?
My best guess is that it is a protective mechanism.
First there is the amount of oxygen provided to the cells / mitochondria. If it is too few then you’ll make fewer ATP but some more ROS (reactive oxygen species). If it is too much then you can make a lot of ATP but ROS production will rise quickly. In between is the optimal point with minimal ROS production. Since we already seem to have trouble with oxidative stress, minimizing it might be rather important and even more so when we crash.
The thing is, too much or too few or just enough is a relative thing. We are said to have poorer function of our mitochondria and when we crash it gets a lot worse. Itaconate is one of multiple ways to reduce the (speed of the) Krebbs cycle. The Krebbs cycle isn’t the part that makes ATP. That is (mainly) the ETC (electron transport chain). The Krebbs cycle mainly produces “high energy intermediates” like NADH and FADH2 and H+. The energy those carrier molecules hold needs to be converted into ATP. That requires a precise balance between “energy carrier molecules”, amount of molecules participating in the ETC and oxygen supply. Get that wrong, and ROS production ramps up a lot.
With us, it seems reasonable to think our “mitochondrial capacity” is already reduced at rest and takes a deep dive when crashing. Our number of cells is roughly the same as in healthy individuals. With normal oxygen release from the RBC (red blood cells), our mitochondria / ETC would likely already see a relative oversupply of oxygen (per mitochondrion and per ETC molecule), risking to already be outside of the optimal zone for minimizing mitochondrial ROS production. When crashing, the Krebbs cycle is IMO more likely to be quickly downregulated then the ETC (because that seems easier for our bodies to do quickly). Keep the amount of oxygen supply constant and the balance of “energy carrier molecules” versus oxygen likely is skewed rather far to plenty of oxygen per carrier. Classic view says that is going to produce copious amounts of ROS.
Now overbreathing does one thing well: reduce CO2 in the blood. And, according to the Bhor effect, that reduces oxygen release from the RBC. Overbreathing hence reduces oxygen seen per mitochondrion / ETC molecule. At rest, it probably reduces it to lower levels then in healthy people given we have poor functioning mitochondria. So at rest we hyperventilate some. When crashing, the functioning of the Krebbs cycle seems to crash and a quick drop in oxygen supply per mitochondrion / ETC molecule is needed to not go into self destruction mode (excessive ROS production). Hence why IMO plenty of us overbreathe massively during crashes or wake up at night breathing like a horse.
Second, RBC barely releasing their oxygen has some advantages: they always seem to have plenty of oxygen aboard. That way, a drop in breathing (for example due to sleep apnea) won’t affect oxygen supply so much (compared to when not rationing). It’s like rationing food during war time. By giving each person no more then the strict minimum of food, fewer people starve to death since the stocks aren’t depleted as soon as any food comes in.
And third, (mildly) low oxygen triggers a number of (wound) healing genetic programs.
There are obvious downsides to poor oxygen release too, such as poor average and maximum capacity to produce ATP. Yet, excessive chronic (or truly excessive during crashing) ROS production might be rather destructive to our bodies. And if we are good at one thing, it is being very ill with very few clear tissue damage to show for.
Good question!
As far as I can tell, stress. Here is my theory: the overbreathing pattern was likely set by sustained fight or flight response in childhood. Family dynamics created some extreme stressors. Neural pathways for breathing were set early on and a pattern of feeling familiar with fight or flight response allowed me to continue to make life choices where fight or flight was a way of life. Eventually, I hit the wall about 6 years ago and my muscles were so fatigued and there was a huge oxygen deficit in my muscles and brain that my breathing pattern could not restore. I basically could not function and had excessive brain fog and chronic pain.
I had done breathwork/meditation for many years (prior to hitting the wall) as a way to calm or soothe the stress. However, until I established the overbreathing pattern, the breathwork, humming, chanting did not help. Perhaps, it might have made things worse. Now that I understand the overbreathing pattern, my the skill with breathwork has made recovery possible. I am able to establish new patterns and recover function, slowly.
I should note that I was a highly accomplished swimmer in my teen years as a way to manage the family stress. And, I enjoyed, for a number of years, extreme physical activity as a way to manage stress. Exercise as a management tool dissipated almost 20 years ago with ever deteriorating abilities until the new, effective breathwork pattern was established. I still cannot exercise as I would like. However, I remain hopeful that my function will continue to increase with the supports.
I’ve been using an Intensity twin stim for years – a couple of times a day for 2ma for 4 min. Don’t tolerate more (my ear starts to hurt). Not a big change, but it makes me feel I’m doing SOMETHING which might help.
Along with ldn and liquid B12 as things which seem to help a bit, and don’t make me sicker.
It will be interesting to see what might be improved, if it really works. Some people swear by these things. Me, not so sure, and not a huge effect.
Warning for Severe ME
Big caution for anyone with severe ME/CFS! Please be aware that any type of “normal” tVNS settings can crash you really fast and really hard!
I am so glad I found the AVA (A Vagus Adventure) Facebook group for people with ME/CFS and LC who are at all severe. There is so much excellent documentation and support there!
So please be super careful to start low and slow as recommended at that group for those wanting to try out this adventure.
And by all means, do not turn up the device until it’s uncomfortable and then turn it down a bit. Big risk doing that.
I second Titania’s recommendation. I personally have not benefited from tVNS, but the thorough and even-keeled info in this group is outstanding.
I told like electrical stimulation. I like to do manual massage around and in my ears, on my neck, head and face and it is helpful.
I did VNS by ear a couple years ago . It did not work for me . The only thing it did was make me feel very nauseous for hours after using it. Nausea is not even one of my chronic illnnss symptoms .
I must have tried it 10 years ago. I had no idea how to use it and got nothing from it. Since you experienced nausea – which is often caused by the autonomic nervous system – I wonder if you had it on too high?
I don’t remember the exact setting but I do remember starting low and slow and could never work my way up because of the nausea .
I had an interesting experience with my vagus nerve recently. I was hospitalised with a severe infection and sepsis after giving birth to a baby, which fortunately was treated quickly. Four days after the infection I experienced what doctors tell me was a strong vagal nerve response to the infection – my heart rate dropped into the 40s and my HRV went up to 115. It normalised within a week after that, but my resting heart rate stayed lower than normal for a month and overall I felt really good in the following weeks- interesting to know if I essentially had a very strong vagal nerve therapy in an odd way??!
Has anyone tried pulsed electromagnetic field therapy (PEMF)?
Yes, I have. It is helpful. But not all PEMF mats are the same. I wasted money buying the Higher Dose mat for at home, which really is a glorified heating pad. Sadly the mat that helps the best costs $8,000 and my doctor is an hour and half drive away, so I can only do it once a month. I have a miHealth device which helps at home. He suggested another device for home use that works with nervous system, $2-3,000. I have the Apollo Neuro also which is like using nothing.
Thank you for the information.
Hi, I am exploring which device to get. Can you please share what your doctor recommended? And also which miHealth device do you have? Thank you:)
The PEMF mat is Sedona Pro Plus mat. The miHealth device is through NES/Energy4life. My doctor is a Energy4life practitioner, Juneva Health in Antioch, California. He has been very helpful. The main theme of all my scans over the past 2 years has been nervous system as the core issue.
What is considered low HRV?
I bought a TENS device called iStim, which can set the pulse width, pulse rate, and frequency, and an ear clip specifically designed for tVNS. Both cost about $100. I’ve been using it for 30 to 60 minutes daily for several years and have noticed the benefits. I feel like my body is being forced to relax. Sometimes I fall asleep. What’s interesting is that the effect varies greatly depending on the electrode placement, rather than the intensity or stimulation pattern. I didn’t notice any results when I placed electrodes on my earlobes, but I can definitely feel the effects on my conch. Of the various treatments I’ve tried, tVNS is one of my favorites as a home therapy. Although I’m nearly bedridden, I use it in combination with biofeedback using heart rate variability and fingertip temperature and so on. Home therapies that have been effective in improving my energy levels include microcurrent electrical neuromascular stimulation, scalp electroacupuncture, hydrogen gas inhalation (with a certain level of emissions), near-infrared light, and HBOT. I haven’t tried any of the more expensive options, but I feel that my quality of life has improved significantly. Skipping these treatments would cause my condition to deteriorate two or three levels. I hope you find the treatment that’s right for you. *
I would really like to do hyperbaric sessions, but a prescription is required and it is difficult to find a doctor in France who will provide one. I know that I lack oxygen. My nose is permanently blocked. I have tried natural products, antihistamines, and cortisone. Nothing has brought relief.
I also tried the Remedee connected bracelet (https://fibrorem.remedee.com/), but I couldn’t tolerate it. I felt even more tired when using it. However, apparently, there are good results for fibromyalgia.
Thank you for interesting information. I had never heard of this device.
And it’s a shame that you can access a treatment that is probably effective.
In Japan, HBOT devices up to 1.9 atmospheres pressure are available without a doctor’s prescription, and due to demand from athletes and amateur runners, they are available massage and acupuncture salon all across Japan.
A new 1.3 atmosphere pressure folding HBOT device can be purchased for $2,000〜.
I bought used one for a cheaper price.
I also suffer from oxygen deficiency, and my peripheral and microcirculatory systems fluctuate greatly depending on my physical condition, resulting in severe extremity chills and visible vascular constriction.
After HBOT session, I feel my body light and flexibleand like olld days.
However, the effects don’t last long, so I try not to push myself too hard.
I hope this information is useful to you and everyone reading this.
I’m going to be in Shinjuku, Ginza and Kyoto soon. Can you recommend places to get the hyperbaric oxygen? What do I look for to be at a reputable place for this in Japan?
Thank you for your question.
First, I’ll discuss three points to consider when choosing a salon.
First, higher air pressures tend to be more effective.
I feel difference depending on how high air pressure is, ranging from 1.3~1.9 atmosphere pressure.
But even 1.3 atmospheres is enough to notice a change.
Second, equalizing your ears is crucial.
This is similar to what you do when diving, but if you’re not used to it, your ears may hurt, and this can become more pronounced with higher air pressures.
If you’ve never tried HBOT before, starting with a lower air pressure might be a good choice.
Third, I recommend choosing a box-type or hard-chamber device.
This is easy to see in the photo on a salon’s website.
These types of devices tend to be more spacious and allow for comfortable use of air conditioning.
Finally, I recommend O₂Care or シエスタ酸素 in Shinjuku, みらい姿勢堂in Ginza, and 酸素カプセルCozy in Osaka, based on the air pressure of the machines. (Using with 1.9 air pressure is available)
The prices are also within the market range.
I hope this was helpful.
Thank you
I do soft chamber hyperbaric oxygen. I’m in the US and a prescription is needed for the hard chamber and it is not covered by my health insurance. So I do the soft chamber through a wellness spa, self pay. It’s worth it and I’m looking into getting one for my home.
I think it’s a great choice. The more frequently I use it, the more helpful it becomes in my life. However, after purchasing it , I realized that I had a cat. I’m worried that one day he might break the chamber.
Bonjour,
Ma belle-fille, diagnostiquée Covid Long en 2922, a retrouvé une vie normale (disparition de la fatigue extrême) après 12 séances de cryothérapie. Hélas, fin 2924, le symptôme de fatigue écrasante est réapparu. Mais elle a profité d’un répit de 2,5 années sans problème. Actuellement, elle recommence des séances de cryothérapie et constate la même amélioration de santé qu’en 2922.
Ma fille, diagnostiquée Encéphalomyélite Myalgique et Covid Long, a tenté cette expérience, mais s’est arrêtée en raison de troubles cardiaques (arythmie).
Que pensez-vous des soins par cryothérapie ?
Cordialement,
Christian Auloy
Google Translate:
Hello,My stepdaughter, diagnosed with Long Covid in 2922, has regained a normal life (disappearance of extreme fatigue) after 12 sessions of cryotherapy. Unfortunately, at the end of 2924, the overwhelming fatigue symptom reappeared. But she enjoyed a break of 2.5 years without problems. Currently, she is starting cryotherapy sessions again and is noticing the same health improvement as in 2922. My daughter, diagnosed with Myalgic Encephalomyelitis and Long Covid, tried this experience but stopped due to heart problems (arrhythmia). What do you think about cryotherapy treatments? Best regards,
Congratulations!
We actually did a blog on that – a rather controversial blog, actually! Glad it worked for one of your daughters. 🙂
https://www.healthrising.org/blog/2024/11/26/cold-exposure-chronic-fatigue-syndrome-fibromyalgia-long-covid/
Merci beaucoup, Cort !
Just to say that I’ve found that simply swallowing raises HRV via Vagus Nerve stimulation.
Cort, would you write about ways to stimulate ANS and recovery (using apps like EliteHRV and polar H10 to mesure and see how change)
Yo uso el tens Med fit 3 desde hace año y medio, 30′ con una frecuencia y otros 30′ con otra, por recomendación de mi fisio, que está muy puesto en esto del nervio vago, pero no sabría deciros si me ha ido bien o si no me hace nada. Hay tantas variantes que nos afectan y que no podemos controlar… no sé cómo estaría si no lo usara a diario… yo me lo pongo con mucha fé… él ya me dijo que era algo a largo plazo… no sé si os sirve para algo mi comentario. El aparato es barato y sencillo de usar. En mi caso me lo prestó mi fisio. Ánimo a todos!
If you’re going to try breathing, try 4:6 (in for four, out for six) or 4:7:8 (in for four, hold for seven, out for eight). Basically, breathing out for longer than you breathe in is more helpful than the “box” breathing 4:4:4:4 for people with CFS.
I totally agree with this recommendation. I did 4:7:8 breathing for a long time and it did not help. I also tried humming and it didn’t help. I have had the most success with 4:6. Basically, if I can just exhale a little longer than I inhale my muscles get more oxygen and I have better oxygen delivery to my muscles. I did start feeling better almost immediately when I did this approach. However, it has taken me 2.5 years with a lot of other vagus nerve reset approaches to get to a functioning level that works for me and my family.
That seems to be more the recommendation now. Thanks!
Hi.
Brain retraing works for me very well. I am a Dutch ME/CFS patiënt, sick for 50 years and really improving since I started in April. I do not use any device or practitioner but I understand the vagal paradox very well now, mainly from the books of Deb Dana. I make my own program.
So everyone, keep up your spirits!
What does a (re)trained brain ( ME patiënts)look like on an MRI scan compared to an untrained brain (healthy people) before and after the retraining (and for ME patiënts in particular)?
Just a warning to anyone tempted to try tVNS on the ear (tragus). I couldn’t get the clip to stay on, even when lying down and stationary. I tried 2 different clips: the cheap standard 2 sided clip commonly available for use witha tens machine, and a Parasym clip. I’ve not seen this problem mentioned in tVNS studies, so maybe not a common problem. But if you have a small tragus it might be better trying a different stimulation area. The frustration of trying to get the clip to stay on did nothing for my stress levels!
A UK group physiosforme conducted a survey a couple of years ago about tVNS for people with ME. 56% reported some benefit.
https://www.physiosforme.com/tvns-survey
Last year they were recruiting for a study of taVNS in ME.
Thanks for the contacts for the tVNS Long Covid study at Mount Sinai. Thought I would pass along that I contacted them and found out that previous diagnosis of me/cfs makes people ineligible for the LC trial. (Not surprising, but thought I would check.)
Sorry you couldn’t get in! will add that to the profile.
I’ll chime in on this one since I’ve used a Nurosym now for over a year. I use it about every other day and only for 12 minutes. I tried the 35-min protocol used in clinical trials and got WAY worse. Overstimulation is a real concern! It can cause worsening fatigue and digestive upset.
Mine consistently delivers deeper sleep (I dream!) and relieves pain as well. Expensive as can be, but I’m happy to have it as a tool in my toolbox.
I made a video review a while back if anyone is interested: https://youtu.be/TyhaXMGBMvo?si=wnWRgCFzeNkpVoPN
Hi Cort. Thanks for this blog. I did reach out to Dr Natelson’s team to see if I might qualify for the VNS study . They were very responsive and prompt in getting back to me for screening. However there are additional health requirements besides the ones noted in the interview. I have a remote history of breast cancer and also have had a parathyroidectomy.
They told me people who are cancer survivors, have had any type of neck surgery, or have significant autoimmune disease won’t qualify.
Since all of those are pretty common, I just thought I’d mention it in case others were considering trying to join this study. Still I think it’s definitely worth a look.
Thanks! I don’t think that was stated in the clinical trials report. I will add that. Sorry you couldn’t get in the study.
I have ME/CFS and a doctor recommended VNS via accupuncture based on my description of immediate PEM (yes, kind of an oxymoron) from simple streching exercises. I have not yet tried it but wondering if anyone is familiar using accupuncture for VNS and the results.
My husband has Parkinson’s disease, adding PD-5 to his nighttime Parkinson’s meds has completely changed his sleep issues. He slept all day and up all night, we had to hire care nurses. Now using this PD-5 medicine for the last four months and a normal routine he sleeps almost completely through the night and may get up once to use the restroom. It’s improved so much we were able to let go of the night nurses. This medicine also helps a ton with memory. we got the treatment from www. limitlesshealth center . c o m I am absolutely confident that this program offers a viable solution. I hope someone find this helpful, We feel very fortunate to have learned about pd-5.
I have been saying Mis-A since the beginning.
What was the drop out rate for the two 2024 studies? I’m asking because I was invited to join a trial but declined because they required patients to use it for 30 min, 6 days a week. I knew it would be too much and my Long Covid doctor also said the same and not to join because it can lead to a crash. I wish these studies allowed more personalized settings/times.
A few comments on different subjects. One for the Can’t Lose study, you cannot have had ME/CFS before getting Long Covid.
I have this $150 ear clip device that I found to be largely frustrating and ineffectual, so I was hoping to get my hands on this more expensive version in the study. There is another company called Vagally that has their version coming to market for $500. I will do some more research via the referred to FB group in the comments. That will be my next trial or PEMF – discussion below.
Currently I am doing HBOT. There is a clinic in Florida AVIV that does HBOT and and charges between $50-100K for Long Covid treatment. What they do is 5 days a week of 2.0 ATM alternating periods of breathing no O2 air for 40 or more days as well as brain imaging. Supposedly, this contrast in breathing leads to Hypoxia Induce Factor (HIF) and stem cells and brain healing. They have alot of testimonies. Like most of you, I cannot afford that. I have found HBOT helpful with my brain fog issues. Now, that I have learned about HIF, I am trying to do my own version using my local 1.3 ATM chamber. It cost me $100 hour, so I go in for an hour and breathe in the O2 for the first 45 minutes. For the last 15 minutes, I then hold my breath over and over again, leaving time for recovery.
Lastly for PEMF, I found a company called Healthy Wave that has a $1300 mat that seems to have all the bells and whistles one might want. Also, they have a reasonable trial period, so if it does not work for you, you can return it. I have not yet purchased one nor tested their return policy, but they seemed to me to be the best price for value. I have no affiliation with them.
Darn…this as in my email and I feel guilty if Idont comment. CFS since 1968 Hong Cong flu. A few years ago observed diagram of Vegas nerve,function unknown at time. Immediately recognized gut brain connection. Purchased alpha stim ( guy that developed ECG. Upon first use I became wonder women for approx. 4 years until contracted RSV.
My focus now is on microglial and coincidentally my Alma mater,,U of A hospital studying this.
I have seen good results with the Truvaga device (which is the commercial version of the GammaCore mentioned above). Increased energy, increased activity tolerance, improved sleep. It is applied to the neck, not the ear.