


Geoff’s Narration
The GIST
The cones are off, the surgeries are healed, and Anni and Cielo are fine 🙂
Update – Once again, life has interfered, putting the blogs on a bit of a hiatus. (That really bugs me!) In fact, life has been interfering in all sorts of odd ways over the past year. There was a 6-week trailer breakdown, a 2-month van engine seizure, several flights from forest fires, a dog that got lost/a dog that got hit by a car/two dogs that underwent 3 surgeries, and another trailer breakdown, etc. Most recently, both solar batteries died, two fridges went on the fritz, and a couple of days ago 3 computers (3 computers! (I am not easy on them (lol) )were broken down (so much for having 2 backups), causing me to break camp and drive 6 hours to pick up a new computer two days ago. Yesterday, a rodent died in the van’s ventilation system (occupational hazard- camping). I have never had anything close to a year like this. The good news is that Anni and Cielo are completely recovered, and my health has remained stable (!) :). Here’s to a more peaceful (and productive) next year or so…

The good news is that the small ME/CFS research field is looking everywhere it can. The bad news (for me) is that in a multisystemic disease that leaves a lot of ground to cover.
The Blog
Recent publications indicated just how broad the ME/CFS research field is. They covered extracellular vesicles, cerebrospinal fluid proteomics, a diffusion-based brain scan, a broad-scale single-cell immune analysis, the circulating proteome, a deep dive into complement, a 7 Tesla fMRI brain study, a lipids analysis, a multi-omics study, and a plasma proteome study.
Every study deserves a blog, but it’s way too much for a layman with ME/CFS to try to do justice to. So I took a different tack. Instead of covering each paper, I threw them all together

 My goal was to see whether, despite the different types of tests, body parts examined, and the different aims of the research groups, any convergences or similar themes emerged. Could a similar story be being told across this very diverse bunch of studies?
My goal was to see whether, despite the different types of tests, body parts examined, and the different aims of the research groups, any convergences or similar themes emerged. Could a similar story be being told across this very diverse bunch of studies?
That would be a nice sign. If we want anything in this disease, we want findings that make sense with other findings. What we don’t want are a bunch of findings that are at odds with each other. Research findings, no matter where they come from, are pointing in specific directions.
Findings in one part of the body, or from one type of analysis, that align with findings in another part of the body or a different kind of analysis, provide a particular kind of robustness.
There were a couple of studies I didn’t include (a mitochondrial study, the recent Prusty study, the Worthey whole genome study, and a gut flora study) in part because the list was already long, I’d already covered some of these studies, and I had to stop somewhere. Otherwise, these are simply the pathophysiological studies published over the past 3 or 4 months.
So again, the question was whether this grab bag set of studies – all done by different research groups with differing aims and focused on different parts of the body – would converge in their results.
I did this by feeding the abstracts from 11 studies into ChatGPT Pro and asking where the studies converged and where they did not. (If you don’t like AI, just pass this blog by.) For me, this kind of thought experiment is a good way to use AI. Treatment suggestions that involve strong drugs are another ball game. Once I had ChatGPT’s answer, I dug into the individual studies.
THE GIST
-

We appear to be getting a grasp of the downstream problems, but what started the ball rolling in the first place?
The ME/CFS field is just too productive for a person with ME/CFS facing all sorts of extra challenges right now (see update at the top of the blog) to cover, so I threw the last ten or so ME/CFS studies together and asked ChatGPT to see if general themes popped out. (If you’re not an AI engine fan, just pass this thought experiment by…)
- Because the studies covered everything from large-scale multi-omics analyses to brain imaging, genetics, cerebrospinal fluid, and extracellular vesicles, etc., asking whether the same general themes emerged was quite a lot to ask. In fact, I thought, the answer would be no.
- The answer was yes. In fact, ChatGPT thought that the great majority of the study results were “strongly convergent”.
- Two major themes popped out. Instead of being characterized by inflammation, the main immune problem in ME/CFS was “immune remodeling” or altered immune networking – a more complex issue to resolve.
- The other major theme involved blood and blood vessel issues. Despite the fact that no blood vessel studies were included, virtually every compartment that was assessed, whether it was in the brain, blood, or spinal fluid, showed evidence of blood/blood vessel problems.
- A recent complement study by the CDC provided a possible connection to the immune system and the blood. Complement activation, it turns out, can not only activate mast cells but also damage blood vessels.
- One might have thought that the most isolated organ in the body, the brain, might be different, but no. Recent brain studies that found evidence of widespread neuroinflammation, complement activation, and blood vessel problems suggest that the same process affecting the body may also be affecting the brain.
- Other prominent themes include a failure to respond to stress and dysfunctional networks.
- Note that while it’s good to see common themes emerge, these are all “downstream” effects. What we really want to know is what’s happened in the headwaters to start off all these diseases.
- ChatGPT proposed three possibilities – two of which were quite linked. One involved a self-reinforcing loop in the brainstem that whacked the autonomic nervous system, producing blood vessel and immune irregularities. Another loop began with the immune system and dysregulated the blood vessels across the body. The last one involved a bodywide breakdown of metabolism, inhibiting energy production across all systems.
- How to get to the source of these mysterious diseases? One magnificent, multiple-exertion stressor (exercise, tilt, cognitive stressor) study that employed many assessments to determine which system goes out first – causing other systems to fail. Once that is determined, attempts are made to turn off the system(s) at the source.
Support Health Rising and Keep the Information Flowing!
Health Rising is not a 501 c (3) non-profit
Note that every study has its holes, and that’s a problem. ChatGPT provided cautionary assessments of each study, i.e., identified places where the findings might not hold up, and highlighted what it considered to be “anchor” studies (e.g., Hanson’s). It clearly preferred multi-omic studies to those that examined a single aspect.
For the purposes of this blog, all the study findings were considered real and accurate, but that may not be true.
You can decide for yourself if the findings make sense.
Two Main Clusters
More than Inflammation: Immune Remodeling Writ Large
It wasn’t so much that the immune system had become activated as it was that it had become remodeled.
We talk a lot about inflammation, but the key immune takeaway was that immune “remodeling” has occurred. That is, ME/CFS is associated with an immune system that is not simply activated but, more importantly, behaves abnormally. This makes sense. If ME/CFS had simply been caused by immune activation, we could just use immunosuppressants. Instead, it’s more complicated.
Nor is ME/CFS simply a T-cell or B-cell disease; that would probably be preferred, but instead it’s a disease of broad immune changes. In other words, it’s not HIV-AIDS (primarily affects T-cells), it’s more complex than that.
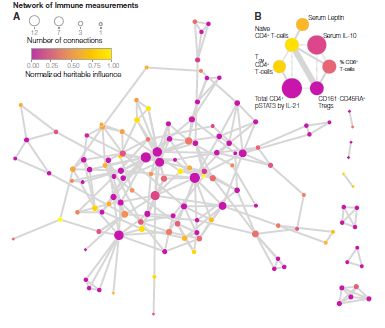
This finding jived nicely with Nancy Klimas’s results using a supercomputer, which revealed altered immune networking in ME/CFS. The immune system is overactivated in some areas and underactivated in others.
One encouraging theme emerged, though. Even in this recent swath of studies, a familiar theme showed up: the innate immune system (neutrophils/monocytes) is accompanied by substantial problems in the adaptive immune system (T and B cells). That scenario gives researchers a nice start.
We saw this best, perhaps, in Ian Lipkin’s big 2025 multi-omics study (not covered in this analysis) titled “Heightened innate immunity may trigger chronic inflammation, fatigue and post-exertional malaise in ME/CFS“. That study highlighted innate immune activation, as well as problems with energy production, fatty acids, lipids, and connective tissue.
Blood and Blood Vessel Problems
Blood vessel problems across the body could, if present, affect just about everything.
Five years ago, we didn’t hear much about blood and blood vessel issues in ME/CFS, but they’re now a major theme. Even though no blood vessel study was found in the mix, evidence of blood and blood vessel problems showed up in most of the compartments tested.
Whether it was signs of activated platelets and coagulation pathways in the cerebral spinal fluid, secretome changes in the serum, hemoglobin issues in the extracellular vesicles, platelet activation in the immune study – indications that something was awry in the blood/blood vessels showed up all over the place.
If two major themes are present, we really want to find a way to connect them together. One of the studies did that in spades. Time will tell whether it turns out to be a major factor.
A Complementary Finding
If any part of the immune system has the potential to link immune remodeling and the blood vessels, it’s probably the complement system. Not only is the complement system a master at turning on mast cells, it can also degrade the connective tissues and dramatically affect the blood vessels.
Could dysregulation in the complement system be the bridge between the immune system and the blood vessels? (Image by Architha-Srinivasan, Wikimedia Commons)
Back in 2003, CDC researchers found exercise increased complement fragmentation in ME/CFS. Twenty-three years later, in a relatively large study (n=171), CDC researchers identified higher C3 levels in ME/CFS patients overall and found that almost 40% had a genetic predisposition to altered complement activity. They were able to backstop some of their genetic findings by noting that similar genetic variants showed up in the Decode ME study. (It’s notable that this is the only paper in this analysis that’s going to postulate a cause…).
The complement system recently popped up big time in several long COVID studies, including a large proteomic study that linked complement activation to coagulation.
The Complement Connection in Long COVID: Microclots, Herpesviruses and More – Could it Explain Much?
Because complement problems may be widespread in ME/CFS, but only a subset of patients have a genetic predisposition to aberrant complement activity, it’s possible that many roads may lead to Rome; e.g., to the complement problems in ME/CFS.
More than the Mitochondria
The “more than the mitochondria finding” has been emerging for some time. Widespread metabolic changes and lipid abnormalities in the serum, B-cells, and extracellular vesicles again suggested that metabolic problems were widespread. While the mitochondria may be affected, ME/CFS appears to be more than a mitochondrial problem. Instead, it appears to be a pervasive state of energy dysregulation affecting many tissues, particularly exacerbated by stress.
The Brain
While the brain is the body’s master regulator, it’s also the most isolated organ. If any organ is going to look different, it’s going to be the brain. On the other hand, finding similar processes occurring in the brain and the body would suggest that core problems have been found.

Widespread findings of neuroinflammation and evidence of complement dysregulation and clotting in the brain seemed to echo what was happening in the body.
One recent paper suggested that the brain indeed plays a central role in ME/CFS. Using more advanced imaging techniques, this paper demolished past (negative) results and found indications of widespread neuroinflammation. The fact that neuroinflammation was associated with increased symptoms suggested it was having a dramatic effect.
Because the white matter in the brain is particularly sensitive to vascular problems, the widespread white matter abnormalities found could be caused by the blood/blood vessel (platelet activation, and endothelial cell issues) and the innate immune activation, as other studies have found. The cerebral edema found could also reflect blood vessel problems as well as inflammation, immune cell infiltration, and others.
Indeed, the first factors out of the gate in the CSF proteome study were none other than the complement system and clotting. Those findings jived well with indications that the extracellular matrix (read “connective tissues”) in the central nervous system had been “remodeled”. They also appeared to align with extracellular matrix remodeling recently found in muscle tissues in Germany, suggesting that this remodeling (read “blood vessel problems”) may be occurring throughout the body and brain.
Meanwhile, a pathway analysis suggested that neutrophil degranulation (there’s the innate immune activation again) and platelet activation (blood/blood vessels) was particularly prominent in POTS. The worse off the POTS patient was, the more these pathways kicked in (complement, more coagulation, insulin-like growth factor), most of which were highlighted by other studies.
Despite the brain’s isolation, it looked like the same processes may be occurring in it and the body.
A Failure to Respond
The idea that when pushed, systems break is not a new one in ME/CFS, but these recent studies highlighted in how many ways this may be occurring. The Hanson paper, “Temporal Dynamics of the Plasma Proteomic Landscape Reveals Maladaptation in ME/CFS Following Exertion“, found that exertion stressors produced pretty much across-the-board problems in immune, metabolic, and neuromuscular pathways.
Meanwhile, the brain fMRI study indicated that, as in the body, an exertional stressor causes connections to fray. A reward circuit that bottomed out after mental exertion could help explain the mental exhaustion that makes it so difficult to take on tasks when PEM is present. (The reward/motivation pathway is central to energy production.)
The suppression of T- and B-cell signaling reported in the Hanson paper aligns well with the adaptive immune dysregulation paradigm. The emergence of inflamed TRP channels was particularly intriguing given the recent Australian paper that pretty much solidified the TRPM3 NK cell ion channel findings in ME/CFS.
TRPM3 ion channel problems have only, to my knowledge, been examined in NK cells thus far, but watch out if they’re present in other cells. Because these calcium channels play a major role in energy production/metabolism, if found in other cells, they could affect immune, sensory, and autonomic nervous system function, as well as blood vessel problems and exercise performance.
This recent spate of studies indicates, once again, that the best way to understand ME/CFS is to push the systems with a stressor and watch them fall apart.
A Network Disorder
Lastly, this short review of recent ME/CFS studies also makes it clear that ME/CFS is a “network” disorder. Anyone hoping for a single disturbed pathway is going to be disappointed. Instead, it appears that the normal cross-talk across multiple systems, particularly after exertion, is off. The problems are showing up everywhere – the immune system, the brain, the muscles, the blood, and…the gut.
Note that bizarre networks also showed up in a major, AI-driven ME/CFS gut study.
Still Downstream…
We appear to be getting a grasp of the downstream problems, but what started the ball rolling in the first place?
It was good to see lots of convergences show up, highlighting many interconnected systems. That, in itself, is a clue – but it’s a downstream clue. We’re kind of stuck swimming around in an estuary that many rivers flow into. We can identify the rivers, but what we really want to know is what’s happening in the headwaters that’s producing this maze of problems.
The Big Picture
The key finding is that a maladaptive reset of the body’s stress-response network has occurred. Every challenge is met with dysregulation. The fact that the problem has to be system-wide cuts out a lot of options. I asked ChatGPT what could have produced such a fundamental reset across so many systems.
“A self-reinforcing loop sitting at a central control point has gotten locked in”
A self-reinforcing loop centered, perhaps, at the brainstem.
The most likely location for this may be the brainstem – a key player in autonomic nervous system regulation. The brainstem regulates heart rate, blood pressure, breathing, arousal, blood flows in the brain, and even immune functioning to some extent. Problems in the brainstem could, in turn, destabilize the endothelium/microcirculation.
We know that brainstem problems play a key role in a subset of patients. The big question is how many.
“A persisting infection/viral reactivation that chronically activates and dysregulates the immune response and could also be impairing blood flows, etc.”
This scenario, thankfully, is being very actively pursued in long COVID. Thus far, it appears pretty clear that this is happening in some long-COVID patients but not all. The big question is how it’s happening. If LC researchers can figure that out, we’ll have a template that can be applied to ME/CFS and similar diseases.
“An immune–vascular/endothelial loop that is keeping the blood from getting through.”
Or is a wonky immune network producing the loop?
This is similar to the infection model but assumes the immune system is simply stuck. Every time any part of the body, whether it’s the brain, the muscles, etc. is stressed, the immune system goes bananas and shuts down blood flows. This could involve an autoimmune process. Note that blood flows play a role in each of these scenarios.
A cellular stress-response / immunometabolic defect – a deep metabolic dysregulation causes cells across the body to shut down their power plants when put under stress. Unable to activate the proper energy production systems, a widespread failure results.
Locking Down What’s Happening
OK – how could we lock down what’s happening? The answer was basically to do the study I’ve wanted for decades. Get a big group of ME/CFS patients, put them on a bicycle, and then measure EVERYTHING.
Hanson, Klimas, Lipkin, Systrom, and others have been moving in this direction. Hanson’s molecular explorations of the effects of exercise, in particular, have produced some profound results. We don’t yet have the exercise study to end all exercise studies, though. I thought the NIH’s Intramural study would be that study, but they chose not to use the exercise session as a stressor.
Remember that these recommendations are all based on the results from the last ten or so studies – not the ME/CFS field as a whole. I also prompted ChatGPT, which did not suggest metabolomics/proteomics/transcriptomics be assessed in its first pass, so I asked it to consider them.
In short, it recommended a deeply phenotyped ME/CFS (Canadian Consensus Criteria; stratified by sex, orthostatic intolerance, age, activity level, infectious/non-infectious) and sedentary healthy control cohort (n=160 total) exercise study.
Three challenges – an orthostatic challenge (tilt table), a cognitive (Stroop, n-back, sustained attention), and an exercise stressor – would be employed. Everyone would take all three tests (!). A small, plucky group of patients would also undergo a 2-day CPET.

The goal – catching ME/CFS/long-COVID patients’ systems as they go haywire during exertion.
The effects of each stressor would be assessed immediately after the stressor, and then at 24 and 48 hours. The effects of the exercise stressor, though, would also be assessed early in the exercise test, as the ventilatory threshold is being reached, and after it is reached, as well as at the end of the exercise, and 10 minutes, 2 h, 6 h, 24 h, 48 h, 72 h later.
(Ok – three stress tests cuts out quite a few patients, but does that really matter? The Open Medicine Foundation’s Severe ME/CFS patient study suggested that severity is a matter of degree, not difference; i.e., severe patients are simply worse off in the same way as less severe patients).
Lactate, pyruvate, catecholamines, purine breakdown products, endothelial markers, complement markers, microvascular imaging, mitochondrial functioning, calcium fluxes, TPM3, NK/T-cell function, blood flows to the brain, brainstem imaging, markers of white matter inflammation, proteomics, metabolomics, and more would all be assessed at different timepoints.
A study like this could pin down what gets triggered first by exertion. My sense is that we will get to that answer over time, but how nice it would be to have a big study assess all these things at once. Does the immune system go haywire first, or is it the autonomic nervous system? Could oxidative stress quickly knock out the mitochondria? What happens to the blood vessels? We know the brain gets affected, but we don’t know how. (Reduced blood flows, reduced energy production, increased inflammation?…)
The idea is to see what comes first and what follows as a matter of course. Once you identify the initial breakdown(s), a proof-of-concept study targeting the upstream areas is conducted in an attempt to resolve the downstream problems.
As ME/CFS researchers are elucidating how exertion affects the body, a large NIH effort called MoTrPAC, which has been underway for about 10 years, is determining what happens at the molecular level during exercise. Among the things it’s been identifying is what has to go right for exercise to work. An upcoming blog will check out how MoTrPAC findings may help us understand what’s gone wrong in ME/CFS, long COVID, fibromyalgia, etc.



“One involved a self-reinforcing loop in the brainstem that whacked the autonomic nervous system, producing blood vessel and immune irregularities.”
This is my dominant working hypothesis right now. The conference in Canada last October had a paper on suppression of dopamine beta hydroxylase, now found in post cancer fatigue and ME. The brain stem cannot send signals to the hypothalamus to regulate blood flow if it lacks noradrenaline (norepinephrine). The lack of hypothalamic blood vessel regulation results in exertion intolerance and orthostatic intolerance, both due to failure to vasodilate or vasoconstrict small blood vessels. This is clearly evidence in the inherited form of this enzyme deficiency, which is relatively rare.
The way I think of this enzyme problem is healthy people can make more just like turning on the tap. It takes a little time and the hormone is replaced. We are on trickle charge, or a drip, drip, drip. It takes a long time to replenish noradrenaline, often involving rest or quiet time, or just very low activity.
This working hypothesis explains nearly every symptom. In particular this one problem leads to not one but two forms of tissue hypoxia, and hypoxia in ME is a topic I have been writing on since about 1998.
One of several possible causal hypotheses I have been considering is a sensor/signal problem, the brain stem thinks we have an infection due to issues with tissue nutrient starvation. Still thinking about this, but it fits. Alternative theories involve immune signaling. All the hypotheses one why dopamine beta hydroxylase is suppressed are as yet unconvincing however.
I have believed for more than 15 years that the primary causal issue lies in the brain. I still think that’s the most likely.
I have long thought that there’s some sort of ‘chronic sickness behaviour’ at play, fundamentally involving interactions between brain and immune system.
Does the brain stem thinking we have an infection explain why the glands in my neck swell and feel painful when I have been dealing with physical or emotional stress?
The swelling of the glands in my neck has always been an early warning signal to me that I have pushed my limits physically or emotionally, so typically I will force myself to slow down and I use horizontal time to help me recover.
I agree the brainstem bloodflow etc…..
Do ypu feel the blood flow to your brain is restricted?
Any one else?
Thanks for the huge effort cort
It is not only a feeling, it has been proved 🙂
https://www.mdpi.com/2227-9032/12/24/2566
I can feel it in my head when the inflammation in the brain builds leading to a feeling of some pressure and pain. Palmitoylethanolamide or PEA and B6 help to reduce this discomfort.
When I read this, I wonder what the mechanism is at the source/basis of this complex pattern of dysfunction.
What happens when you ask ChatGPT Pro to compare the dataset you used in this blog post with the information in Robert Naviaux, MD PhD’s foundational article, “Metabolic Features of the Cell Danger Response”?
https://www.sciencedirect.com/science/article/pii/S1567724913002390
Great idea, Jerry. My guess is that paper has had a major impact in how many people think about ME/CFS.
It certainly had a major impact on my own thinking about ME/CFS. I’m hoping it will be feasible for you to get ChatGPT Pro to weigh in on possible correlations between the information in Dr. Naviaux’s treatise and the data you’ve had ChatGPT Pro analyze in this post we’re discussing here.
After 43 years of CFS and FM diagnosed, a specialist GP gives me 3 new labels – hEDS, MCAS and nTOS. All of these ‘odd’ diagnosed have to fit under the same umbrella. Research on hEDS is focusing on multiple genes cause no particular DNA has been found.
All of those effect or can effect the connective tissues. (I looked up nTOS – neurogenic thoracic outlet syndrome – compression of the blood vessels and/or the nerves.) I just spoke with an ME/CFS specialist who is finding more and more venous compression syndrome; i.e. the veins are getting tweaked – not allowing proper blood flows – and presumably causing reduced preload AKA David Systrom. That ultimately reduces blood flows to the tissues. It’s no wonder that Dr. Ruhoy is so interested in connective tissues.
https://www.healthrising.org/blog/2025/09/24/pelvic-venous-syndromes-pots-chronic-fatigue-long-covid/
Well, that’s given me lots to look at. I now have a rectal prolapse to add to the list. My body still holds a secret in that every month on either 20th or 21st I get an agonising pain in my right flank area which causes neurological symptoms.This has been happening for about 40 years. Sooo many investigations 🥺 it only happens in the evening and no one has ever seen me to investigate at that time. Now, looking at those venous issues from the blog, I have new enthusiasm for more research. I’ll be 80 in July and I’m not giving up til I find the source of this. Thanks so much for linking the blog.
I just talked to a doctor who had thigh pain and it turned out to be venous compression and the development of a lot of collateral blood vessels. Oddly enough, the first scan by one group didn’t find anything – the next scan by a different group found a badly compressed vein. Good luck!
Thank you.
I think youre right cort. Eagle syndrome, nutcracker syndrome and all various expressions of as you say vessels being tweaked may be at play.
Its a relatively easy study to create at scale too
I get a little tingle of excitement reading about AI’s discoveries.
For me, for years now, as I have encountered one person after the next who doesn’t believe in this illness or its severity, I can’t get out of my head a brief scene from a movie I saw long before I got ill.
The movie is Apollo 13. The spacecraft has had a catastrophic malfunction mid-flight, and in this scene the astronauts cut loose the damaged module and report to Houston what they see as it drifts away. Here is the 18-second clip.
https://clip.cafe/apollo-13-1995/jlm-houston-were-getting-our-first-look-at-the-service-module-now/
Thank you Cort for you continued dedication and commitment to our collective cause.
So grateful that we have you keeping us all up to date with the latest empirical stuff.
I really hope this year goes better for you and your doggie crew.
Love your suggestions for “your ideal piece of research.
Hoping 2026 brings us all closer to “The Answer”.
Thanks, Karina. The dog’s health issues were scary. One emergency surgery, and two more surgeries – it really seemed touch and go – but a month later they are back to full health! It’s just amazing how quickly they’ve recovered.
So grateful for your amazing work especially when you have challenges yourself but continue to support us with your reporting.
Thanks. I hope smoother sailing is ahead. It’s not so much the things that have happened but how they get in the way…
Cort,have you followed any of the three people that you reported on that had the spinal surgery.i believe you reported one or two of them went overseas to have the surgery done. Just wondering if the surgery had lasting effects?
I haven’t. Good idea, though. From what I’ve heard there are a variety of results – not unexpectedly. We really need a more comprehensive view of how people have done. Thanks for the reminder.
Wow, Cort! You’ve been through the “wringer”! I hope that things really settle down for you and pups now.
What you did with AI is great. Thank you always for keeping this community informed of what is going on that we would otherwise never hear of.
Thanks, I just had a very nice win – got the pour mouse out. Turns out the blower motor, which dates back to 1996, is nice and accessible in contrast to newer models. :)…Otherwise I might have been looking at a hefty repair to take the dash apart.
The findings of a dysfunctional TRPM3 ion channel are getting more and more solid, both for ME/CFS and long COVID, and may be a major overlapping factor.
The TRPM3 ion channel function can be restored with low-dose naltrexone (LDN, around 3 mg/day), and it’s interesting to see that LDN not only helps relieve key symptoms in ME/CFS and long COVID but also in related/similar disorders such as fibromyalgia, MS, RA, hEDS and Crohn’s (etc, the list doesn’t end here).
However, LDN is not known to cure people, and there may well be one or several upstream mechanisms to the TRPM3 dysfunction that needs to be understood. LDN is known to affect the TRPM3 channel through the mu-opioid receptor, but it also affects the TLR4 receptor which is important for inflammation.
Interestingly, TRPM3 also regulates vascular tone and TRPM3 levels are higher in female arteries than in males’….
Very interesting! The Aussies at Griffiths I think it is have really stuck with these channels. I hope they can check them out in other cells and tissues.
I think the Opus model by Anthropic (Claude) is unrivaled when feeding it large chunks of medical data. Even when applying the best prompt engineering GPT pales in comparison. Claude has found a much completer picture of what I am dealing with in trrms of illness, than anyone ever has. And it will probably save my life down the road
Of the search engines I’ve tried ChatGPT has seemed the most comprehensive and careful thus far with Perplexity not far behind. Google Gemini is good but it’s too glib and I don’t trust it as much. Copilot can be very helpful with other tasks but I’ve caught it a couple of times in some real howlers.
I actually just got the free version of Claude yesterday and will look for Opus. Thanks for the tip 🙂
Sorry to hear you’ve been having so many challenges recently Cort!
I was wondering if you have used the RTHM Intelligence platform? I don’t know which AI it uses, but I have found it to be helpful. It may be better for individuals rather than analyzing multiple studies. Just curious.
I keep feeling like we’re getting closer to answers that really move the needle, but this illness is so complex!
I work in AI. My guess is that RTHM is using a less powerful model under the hood.
The only benefit is that you get unlimited queries and can attach your health data.
For analyses like what Cort is doing, the consumer facing models are best.
Good to know – thanks.
Any recommendations on the best AI engines to dig into ME/CFS, long COVID, FM, etc. research?
Claude in general is considered the best of the famous ones at the moment. You are more likely to run out of usage per session/ week, because each prompt is more intensive.
Seconded, Claude is the best for heavy-hitting, but also the most limited in terms of number of queries. Best to reserve only your most critical work. I use ChatGPT as a backup for more pedestrian questions.
I do want to check RTHM out…
Remember LLM AI is based on what is known, with a bias towards what is most stated. In simple words, “medicine by hearsay”. You are looking at the past… and has the past cured ME/CFS….
I am a former University Instructor of AI and LLM (Anthropic,Claude, etc) is a poor choice. My own preference are PREDICTIVE models — which AI does not do. Hence I developed microbiome prescription that uses Fuzzy Logic Expert System running on 14,425,408 facts (as of this AM) extracted from studies published on PubMed.
It does a very good job in predicting symptoms SOLELY based on a detail microbiome sample.
Yeah, I get what you’re saying about LLM. But I think you’re doing the same thing in reverse—just narrowing everything down and calling it predictive. Though I am sure what you built is very impressive for what it can generate. However these illnesses aren’t one-system problems
I try to do the opposite by throwing everything in: labs, mri, doctor notes, my own logs, and then mapping that against the entire correspondng literature (me/cfs, long covid, post viral) to see what actually lines up with my personal data. I would add that slice of microbiome information. Not replace it with And ofcourse put guardrails on predictive output. Probability score vs possibility
Thank you, Ken, for this reminder. The problem is probably that folks don’t want to understand what LLM is and what it can do because they want to see something else in it, something with which they themselves can make a contribution to the research.
I understand that aspiration but I think that it would be better if patients asked their AI companions how to do a fundraiser to support biomedical research.
It’s probably easier to understand why LLMs are not able to come up with new ideas when you have an academic training and have learned how to create new research questions and how you do it based on incongruities in the literature and data while you can’t find it formulated in the literature and data. Which is why LLMs can’t offer it to you.
I agree! Claude is by far the best (although not perfect, you always need to confirm understanding and requirements)!
Thank you Cort for taking the time to do this analysis. It is very interesting. I hope that things are going well for you.
I was really surprised to see the convergences pop up to tell the truth. I thought – too many different kinds of studies for that. Time will tell!
I am still convinced that the root cause is a microbiome dysbiosis which results in an ugly mixture of metabolites (chemicals) being pumped into the body. It would account for ALL OF THE FINDINGS… and more important, it is ACTIONABLE TODAY (and not waiting on future clinical trails that will not be completed for 5 years). I was taught to always go with the SIMPLEST MODEL that explains the most observations. For evidence, review:https://blog.microbiomeprescription.com/modifying-your-microbiome/analysis-posts-on-long-covid-and-me-cfs/
https://blog.microbiomeprescription.com/modifying-your-microbiome/analysis-posts-on-long-covid-and-me-cfs/
Wow Cort! You are on (an unfortunate) roll! You started the Year of the Fire Horse early. 🙁 Hopefully things will start settling down for you now! I have a question about AI I sent you by email. This was a very good use of AI and very interesting outcome. Look forward to looking through some of the articles individually but thiscompilation saves a lot of time. Thanks!
Ha! The year of the Fire Horse…That sounds exciting! 🙂
I believe the appropriate word is “chaotic!” And yes with the exclamation point as part of the word. 😉
Great blog and approach! More importantly, wishing you a much calmer rest of the year!
Yes Cort, you are right, there is a significant impact of autoimmune processes affecting the entire system.
Unfortunately, many ME/CFS patients have never received proper hematological testing or a comprehensive diagnosis.
The day after I shared my case report, Medical Summary – Hemostasis Evaluation Results,
https://swaresearch.blogspot.com/2026/04/case-report-medical-summary-hemostasis.html
I discovered the following:
“CD19 CAR-T therapy induces remission in refractory autoimmune hemolytic anemia with ITP and antiphospholipid syndrome”
https://www.cell.com/med/fulltext/S2666-6340(26)00078-4?_returnURL=https%3A%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS2666634026000784%3Fshowall%3Dtrue
Context and significance
Growing evidence supports the ability of CD19-directed CAR-T cell therapy to highly efficaciously reset dysregulated B cells in autoantibody-driven autoimmune diseases. However, data on refractory AIHA or antiphospholipid syndrome are very limited. Here, we present a patient with severe, treatment-refractory AIHA with coexisting ITP and APLAS who received CD19-directed CAR-T cell therapy on the basis of compassionate use. AIHA was transfusion independent from day 7 and hemoglobin normalized within 25 days. No cytokine release syndrome or neurotoxicity occurred. The pathologically elevated antiphospholipid antibodies normalized, and ITP stabilized without any additional therapy. This case demonstrates rapid, durable remission of severe, refractory cold-agglutinin AIHA with simultaneous improvement in coexisting APLAS and ITP on a highly favorable toxicity profile. This case supports further clinical validation of the concept.
I WAS PREPARED TO CRITICIZE AI FOR A NUMBER OF REASONS, BUT, JUST TO BE FAIR, I THOUGHT I WOULD CONDUCT A LITTLE TEST THROUGH CHAT-GBT. EVERY AFTERNOON, I GET AN INTENSE COLD FEELING INSIDE MY HEAD. NO DOCTOR HAS BEEN ABOUT TO COME UP WITH A REASON, BUT CHAT-GBT DID ALMOST IMMEDIATELY. SINCE I HAVE HAD A VERY BAD YEAR, THREE EPISODES OF SYNCOPE, THE LAST ONE RESULTING IN A BROKEN WRIST AS WELL AS RIB AND HIP BRUISES, I DECIDED TO DIVE IN FURTHER. CHAT-GBT IS UNBELIEVABLE. I HAVE A COMPLEX MEDICAL HISTORY AND IT UNDERSTOOD IT ALL; MADE RECOMMENDATIONS AND EVEN WROTE A LETTER TO GIVE TO ANY NEW DOCTOR. NO GAS-LIGHTING, NO EYE ROLLING. AND I CAN GO BACK AND ADD TO MY CHAT WITHOUT LOSING ANYTHING. IT IS REMARKABLE. IS IT CORRECT? I DO A LOT OF RESEARCH IN MY WORK AND I COULDN’T FIND ANY FLAWS.
CORT, I WISH YOU HAD AN EDIT FUNCTION SO WE COULD CORRECT OUR COMMENTS. I NEVER SEE THE MISTAKES UNTIL AFTER I HAVE HIT SUBMIT “NO DOCTOR HAS BEEN ABLE (NOT ABOUT)”
Thanks for a lot of interesting information. I’m in a major round of PEM, so focusing in all the details is neither wise nor easy.
What did light up my brain were mentions of the autonomic nervous system. I have been using an OTC VNS (Nuropod) for about four weeks with all kinds of good results.
I started at the recommended dose, felt great, and within two days was having very difficult PEM. Immediate support from the manufacturer was not available, so I went to Claude.ai (which knows a lot about my health) and it recommended a much reduced dose on a much slower ramp up.
In the middle of week three I felt good enough to try an experiment of two high (cognitive and physical) stress for me. I assumed I ‘d have PEM and was interested to see how quickly it resolved. The answer is TOO long. It’s a week later and I am just starting to recover.
I have a list of comorbitities that makes my doc’s shake their heads, all exacerbated by the fact that I am 81 and HSP as well as 2e ADD/Giftedness.
When I did finally connect with a nuropod doc, she said that she suspects that the reason for my initial intolerance is based in my extreme sensitivity, not my CFS. That said I’m a big fan of VNS, BUT wary of recommending it for CFS except at low starting dose. I started at 2 minutes in the morning and am now up to 4 minutes in the AM and 2 minutes late afternoon. Both Nuropod Doc and Claude that that is likely as I need to ever go since I am getting significant improvements in HRV, ADD, Depression, constipation, spinal pain. All of which lead to a much rosier outlook on life as long as I am careful to tend to my energy envelopes with care.
Congratulations, Gary. I had a similar experience with Mestinon – took too much too quickly – did great then crashed – and then ramped down (thanks to ChatGPT) and am doing better. Our systems are so easily overwhelmed. Please keep us informed how its going.
Cort,
Thanks for the analogy.
Three questions, please:
1. know naught of mestinon. Did it help(what) at the right dose…which was??? How did you get a doc to prescribe it? I use the VA system and getting them to go off-label is often a gordian knot.
2. Are you HSP or neuro-atypical? Context:does CFS alone warrant caution on using VNS?
3. Are you using ChatGPT rather than Claude (or other) for a specific reason/ Or is that you you started and know how to use it effficiently
Sorry to hear about all the mishaps lately, Cort! But, as always, you have provided an excellent, comprehensive summary of these recent studies. As I was reading your article, I kept shouting “YES!” at my computer screen and reading parts out loud to my husband.
I have always been convinced that my own ME has immune dysfunction at its heart and in recent years (I’m 24 years in now), it’s been clear that immune activation is a big piece (but as you explained here, not solely immune activation but a mixed bag of immune dysfunction).
These days, after decades of searching for (and finding) effective treatments – plus knowing my limits, I live a fairly active life and crashes from over-exertion are rare for me. BUT, longer relapses due to immune activation continue to plague me, including every fall and winter, and nothing seems to help those. When a sore throat and flu-like aches (i.e. symptoms of immune activation) set it, I know I am in for a long period spent lying on my couch.
I also read your article summarizing Dr. Lipkin’s 2025 study and plan to talk to my doctor about that.
Thank you, Cort, for all you do for this commnunity, even in the face of your own illness (and other challenges!). It is deeply appreciated.
Sue Jackson
Are they using AI to analyze. A Cfs patient. And or the disease Mecfs?